











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Perthes disease impaired vascularization in the femoral head and may cause incongruence of the hip joint during the hip remodeling period1. Hip joint osteonecrosis leads to various deformities of the hip joint, and in later life, secondary end-stage degenerative osteoarthritis may occuR2. Despite numerous studies, an algorithm could not be established for this clinical entity.
Maintaining hip containment during the disease reduces the deforming forces on the femoral head. During the disease process, the shape of the femoral head and its congruency with the acetabulum affect the prognosis. The "Biological plasticity" concept allows the acetabulum to serve as a mold to the femoral head during the healing process. The treatment goal is to obtain a congruent hip joint with a good range of movement by achieving a spherical femoral head and a well-shaped acetabulum at skeletal maturity. The risk of developing coxarthrosis in the joint may be reduced or delayed3,4.
In the late stage of LCP (Legg-Calve-Perthes) disease, the anterolateral deformed femoral head protrudes outside the acetabulum, and during hip abduction, impingement occurs. Hinge abduction causes incongruity of the hip joint and restricts hip movement. Various surgical procedures ranging from cheilectomy to shelf acetabuloplasty for surgical containment have been described to overcome "hinge abduction." In the presence of severe femoral head deformity, valgus extension osteotomy may be required as a salvage procedure because it overcomes the hinging and creates a more congruent surface of the femoral head within the acetabulum5,6. Tectoplasty provides an extra-articular weight-bearing surface and a more congruent acetabular roof6.
The basis of treatment in Perthes disease is to provide and maintain containment in the hip joint. According to the lateral colon classification, Hering group C patients have a poor prognosis. Femoral head deformation and decreased acetabular depth cause containment problems and create discongruence in the hip joint. In case of discongruence in the hip joint, remodeling is impaired. In the combined treatment we performed femoral valgus extension osteotomy to overcome the hinged abduction while the anterolateral part of the femoral head impinges during abduction. The aim of tectoplasty is to create an extra-articular load-bearing surface area on the acetabular side.
The purpose of this study was to evaluate the long-term clinical and radiographic outcomes of femoral valgus extension osteotomy combined with tectoplasty in severe LCP patients. In a previous study, we evaluated the short-term clinical and radiographic outcomes of this technique in 11 Herring group C LCP patients7.
Method
The study had institutional review board approval (reference number 2020/170). We evaluated retrospectively the long-term clinical and radiographic outcomes of 13 LCP patients who underwent femoral valgus extension osteotomy combined with tectoplasty between 2002 and 2009. In our study, all patients were diagnosed with LCP and classified according to lateral pillar classification as Herring group C. All patients had intraoperative radiographic and clinically diagnosed hinge abduction.
The study group of 13 patients analyzed consisted of one female and 12 males; in eight cases, the right hip was affected, and in five, the left (Table 1). The mean age at diagnosis was 8.6 ± 2.2 years. The mean age at surgery was 9.3 ± 1.7 years. The mean age at the most recent follow-up was 23.3 years. All patients were followed at least 11.5 years after surgery (mean 15.5 ± 3.3 years). Clinical assessments of all patients were made in terms of pain, range of hip motion, fixed hip contractures, leg length discrepancy, and presence of limp. All patients were examined preoperatively under general anesthesia to confirm the presence of hinge abduction. With the presence of hinge abduction femoral valgus extension, osteotomy was performed in all the patients in our study. A lateral approach was performed to the proximal femur. The femoral neck was prepared for an angled blade plate or K wires. A transversal cut between the femoral shaft and lesser trochanter was performed, and an extension and valgus were built into the osteotomy. The correction angles required for adequate femoral coverage, were determined by comparison of the contralateral side. After femoral valgus extension osteotomy, fluoroscopic evaluation was performed intraoperatively. Tectoplasty procedure was added to patients who were detected to have inadequate femoral head coverage. The tectoplasty procedure aims to enlarge the weight-bearing area at the hip joint and obtain a more congruent joint. It was performed in a supine position by an anterior Smith-Peterson incision with the technique described by Saito et al.8. In this technique, care was taken not to damage the lateral acetabular growth cartilage. All surgical procedures were led by a single experienced pediatric orthopedic surgeon (C, B). Patients were mobilized non-weight bearing with crutches to the operated side until graft healing was observed. After graft healing and osteotomy union were observed radiologically, partial weight-bearing was permitted, and commencing full weight-bearing began at 3-4 months.
Table 1 Patients demographics
| Number of patients | 13 |
|---|---|
| Number of hips | 13 |
| Age at diagnosis (years)* | 8.6 ± 2.2 |
| Age at surgery (years)* | 9.3 ± 1.7 |
| Gender (M/F) | 12/1 |
| Involved site (R/L) | (8/5) |
| Length of follow-up (years)* | 15.5 ± 3.3 |
| Length of post-op (months)* | 188.4 ± 34.6 |
| Age at last follow-up (years)* | 15.5 ± 3.3 |
| Lateral pillar classification (A/B/B/C/C) | -/-/-/13 |
| Patients with Hinge abduction | 13 |
*The values are given as the mean, with the standard deviation in parentheses. M: male; F: female; R: right; L: left.
All the patients had pre-operative, early post-operative, and final follow-up clinical and radiographic evaluations (Fig. 1). The radiographic examination included an anteroposterior view of the pelvis in neutral and frog-leg position. Pre-operative staging and severity of disease were determined using modified lateral pillar Herring classification9. These subjective assessments were carried out independently by two of the authors (MK and ME-B). The radiographic parameters included Center-Edge angle (CE angle), Sharp angle, femoral head size ratio, neck shaft angle, acetabular depth width index, caput index, subluxation ratio, femoral head coverage ratio, and femoral head extrusion index. Osteoarthritic changes were evaluated using the Tönnis classification10. At the final follow-up, the radiographic outcome was assessed using the Stulberg classification to evaluate femoral head sphericity and hip remodeling11. The spherical femoral head (Stulberg 1 or 2) was rated as good, the ovoid femoral head (Stulberg 3) as moderate, and the flat femoral head (Stulberg 4 or 5) was rated as poor outcomes. The clinical assessment includes; the hip range of motion, limb-length discrepancy, the presence of a Trendelenburg sign, and a visual analog scale (VAS) (ranging from 0 to 10). All participants completed the Harris hip scoring system (maximum score, 100 points). A total Harris hip score below 80 points was considered a poor or fair result, and 80-100 was a good or excellent result12.
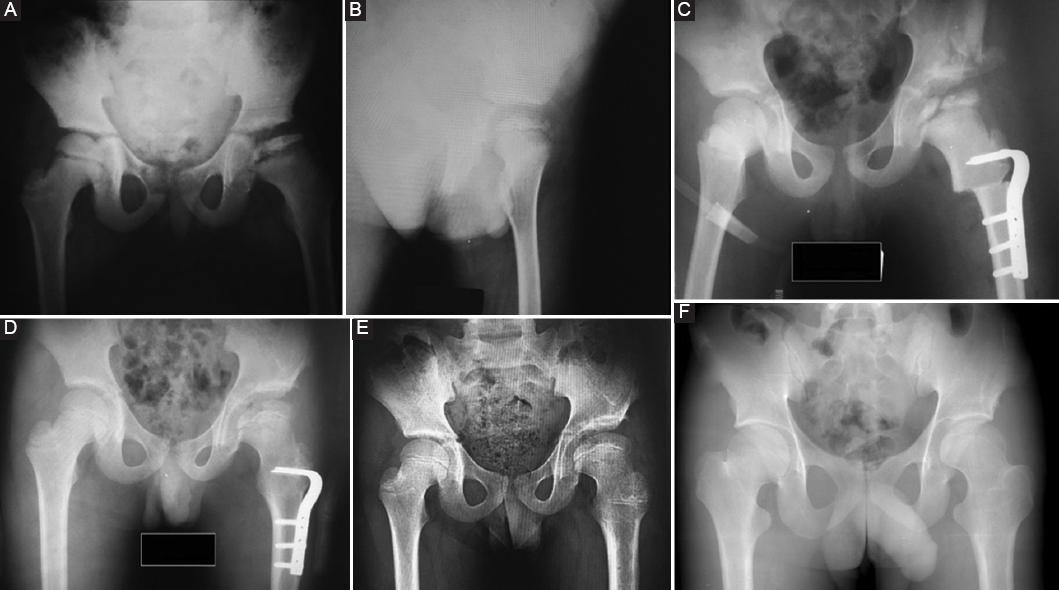
Figure 1 Plain radiographs of an 11-year-old boy following femoral valgus extension osteotomy combined tectoplasty. A: pre-operative anteroposterior radiograph. Herring group C Perthes. Femoral head subluxation and flattening B: pre-operative lateral radiograph C: early post-operative anterior-posterior radiograph D: post-operative 1-year anterior-posterior radiograph E: post-operative 4-years anterior-posterior radiograph F: last follow-up post-operative anterior-posterior radiograph. There is good and lasting coverage with satisfaction of the femoral head.
Statistical analysis
The statistical analysis was performed using Statistical Package for Social Sciences (SPSS) Version 22.0 (SPSS, Chicago, IL) statistical analysis software. Normal distribution was defined by the Shapiro-Wilk test. All values were calculated as the mean and the standard deviation. The pre-operative and post-operative comparisons were performed using repeated measures analysis of variance. Data were analyzed for statistical significance using the paired t-test, and p < 0.05 was considered statistically significant. Spearman correlation analysis was conducted to analyze the pre-operative factors that were strongly associated with patient outcomes. Patients who were ≤ 8 years old at the time of diagnosis were compared with those who were > 8 years old. Harris hip score and the Stulberg classification were used to determine patient outcomes.
Results
All children presented with a painful limping gait preoperatively. At the time of surgery, all hips were classified according to lateral pillar classification as Herring group C. The mean Harris hip score improved from 70.23 ± 10.43 preoperatively to 91.76 ± 7.25 points at the final follow-up. The mean leg length discrepancy preoperatively was 1.46 ± 0.51 cm and after skeletal maturity at the last follow-up, was 0.53 ± 0.59 cm (p < 0.001). No patient had a limping gait or Trendelenburg sign at the final follow-up. The mean last follow-up hip flexion was 122.30° ± 11.65°. There were no significant complications or need for additional surgery. The pre-operative VAS score was 7.84 ± 0.22, and the last follow-up VAS score was 1.03 ± 0.25 (p < 0.001).
Follow-up radiographs were analyzed for 13 patients (13 hips) (Table 2). According to the Stulberg classification, good radiological outcomes were obtained in seven hips (seven hips were class 2), whereas fair or poor outcomes were noted in six hips (four hips were class 3 and two hips class 4). Six hips had mild degenerative changes (Tönis grade 1), five had moderate (Tönis grade 2), and two had severe changes (Tönis grade 3). The mean subluxation ratio was 1.66 preoperatively and 1.23 at the last follow-up (< 0.001). The mean femoral head coverage ratio was 67.53% preoperatively and 84.61% at the last follow-up (= 0.009). The mean femoral head size ratio was 1.1 preoperatively and 1.20 at the last follow-up (p = 0.077). Sharp angle decreased from 46.76 to 35.77 (p < 0.001). Centre edge angle increased from 14.30 to 40.07 (p < 0.001). It was no significant change in neck-shaft angle (p = 0.477). The acetabular depth-to-width index improved from 272 to 308 (p = 0.008).
Table 2 Clinical outcomes according to age at diagnosis
| Measure | Age at diagnosis | p | |
|---|---|---|---|
| ≤ 8 years (n = 5) | > 8 years (n = 8) | ||
| Stulberg classification | |||
| 1 or 2 | 4 | 2 | 0.159* |
| 3, 4 or 5 | 1 | 5 | |
| Last follow-up Harris hip score | |||
| ≥ 80 points | 4 | 7 | 0.742* |
| < 80 points | 1 | 1 | |
| Tönnis grade | |||
| 0 or 1 | 3 | 3 | 0.471* |
| 2 or 3 | 2 | 5 | |
*No significant difference between ≤ 8 and > 8 (p > 0.05).
Patients who were ≤ 8 years old at the time of diagnosis were more likely to have a lower Stulberg class; however, the differences were not significant (Table 3). There was no significant relation between age at diagnosis and last follow-up Harris hip score and last follow-up Tönis classification. There were no cases of failure of fixation, and all osteotomies went on to radiologically proven union. There were no significant deep infections.
Table 3 Comparison of pre-operative and post-operative radiological outcomes
| Measure | Pre-operative | 1 year post-operative | Last follow-up | p | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Subluxation ratio | 1.66 | 0.33 | 1.47 | 0.26 | 1.23 | 0.12 | < 0.001* |
| Femoral head coverage ratio (%) | 67.53 | 11.68 | 100.30 | 6.27 | 84.61 | 11.75 | = 0.009* |
| Femoral head size ratio | 1.13 | 0.11 | 1.23 | 0.18 | 1.20 | 0.13 | = 0.077 |
| Sharp angle | 46.76 | 6.85 | 33.38 | 4.92 | 35.77 | 2.95 | < 0.001* |
| Sharp ratio** | 1.13 | 0.11 | 1.22 | 0.18 | 1.19 | 0.12 | = 0.077 |
| Center-Edge angle | 14.30 | 5.21 | 43.23 | 6.33 | 40.07 | 9.38 | < 0.001* |
| Neck shaft angle | 142.61 | 8.55 | 152.46 | 7.63 | 145.38 | 10.16 | = 0.477 |
| Caput index | 0.69 | 0.12 | 0.67 | 0.15 | 0.74 | 0.12 | = 0.166 |
| Acetabular depth-to-width index | 0.27 | 0.03 | 0.31 | 0.05 | 0.30 | 0.04 | = 0.008* |
| Femoral head extrusion index | 32.13 | 5.66 | 0.57 | 0.22 | 13.38 | 6.23 | < 0.001* |
| Acetabular depth-to-width ratio | 272.3 | 31.6 | 315.3 | 50.4 | 308.4 | 39.1 | = 0.008* |
*Statistically significant (p < 0.05).
**The ratio of the Sharp angle of the affected hip versus the contralateral normal hip. SD: standard deviation.
Discussion
We evaluated the long-term clinical and radiographic outcomes of femoral extension valgus osteotomy combined tectoplasty as a means of surgical containment for Herring group C LCP patients with hinge abduction. In our study, we aimed to provide a spherical femoral head within a well-shaped acetabulum in the final process. Even in the case of collapse and deformation, the femoral head tends to be remodeled if it is well-contained in the cartilage13. All patients in our study were severely affected and had a massive femoral head involvement with lateral subluxation.
The treatment algorithm in severely affected Perthes patients is still controversial. In a multicentric prospective study, it was shown that the lateral pillar classification and age at the time of onset of the disease are strongly correlated with outcomes13. Some reports stated that group C hips frequently had poor outcomes unrelated to treatment14,15. However, in those studies, the surgically treated group received either a femoral or acetabular osteotomy, not a combination of these procedures. It was shown in a study of severely affected patients, that a femoral varus osteotomy improved the sphericity of the femoral head compared to conservative treatment16. Combined procedures in severely affected patients provide better congruency of the hip joint17. In another study, the combined procedure group obtained significantly better outcomes both clinically and radiologically in severely affected hips compared with the single procedure group18.
Hinge abduction is the process of severe Perthes disease, causing the deformed and extruded anterolateral femoral head impingement to the lateral lip of the acetabulum during the abduction. Operative and non-operative treatments were reported to deal with this entity. Traction and bed rest, Shelf acetabuloplasty, and triple pelvic osteotomy treatment methods were performed. Another treatment method is femoral valgus extension osteotomy, which was first described by Catterall. It rotates the deformed extruded femoral head away from the lateral lip of the acetabulum, and the abnormal hinge movement aimed to get resolved. This relieves pain, reestablishes the abductor mechanism, and improves leg length. Unloading the lateral part of the femoral head and the lateral acetabular physis may produce favorable hip remodeling. We added the tectoplasty procedure to enlarge the weight-bearing surface without decreasing the volume of the acetabulum. Thus, the development of femoroacetabular impingement was prevented. A deformed femoral head and acetabulum cause an obliquity of the weight-bearing joint surface that changes the rotation center of the femoral head. As a consequence, the loading pressure in the reduced articular area increases. Osteotomies are designed to reduce the loading of the joint surface by increasing the area of the weight-bearing surface. Femoral valgus extension osteotomy stretches the superior zone of the joint capsule and its synovial membrane. It stimulates the remodeling capacity of the hip19. There was no other study that reported the long-term outcomes in the literature of the femoral valgus extension osteotomy combined tectoplasty procedure for hinge abduction in Herring group C perthes patients20.
Stulberg classification has been used to evaluate the surgical clinical outcomes in the literature21,22. In the treatment procedure, we aimed to prevent femoral head subluxation, obtain a congruent hip joint, eliminate hip irritation, restore adequate hip movement, and relieve pain. Treatment modalities performed on patients with severely affected hips vary widely in the literature20,23,24. These are femoral valgus osteotomy, shelf acetabuloplasty, tectoplasty, triple pelvic osteotomy, Chiaris' pelvic osteotomy, Salter pelvic osteotomy, and a combination of them. Chang et al. evaluated the outcomes of patients with 21 severely affected hips undergoing the Staheli procedure. According to Stulberg's classification, 33.3% were good (class 1 or 2), 38.1% were fair (class 3), and 28.6% were poor and bad (class 4 or 5)25. In another study, the results of patients who underwent Shelf acetabuloplasty were reported as 51.8% good, 29.6% fair, and 18.6% poor5. Huang and Huang reported 14 patients' results who underwent triple pelvic osteotomy as good at 35.7%, moderate at 42.8%, and poor at 21.4%26. We performed a femoral valgus extension osteotomy combined with tectoplasty, which had not been reported in the literature before. In our study, we evaluated the clinical outcomes as 53.8% good, 30.7% moderate, and 15.3% bad. This rate is comparable to reports using other surgical procedures in severely affected hips.
In our study, the femoral head coverage ratio improved from 67.53% preoperatively to 84.61% at the last follow-up. Chang et al. performed a Shelf acetabuloplasty procedure in severely affected hips, and in this study, the femoral head coverage ratio improved from 74% preoperatively to 98% postoperatively25. Huang and Huang performed triple pelvic osteotomy, and improvement was observed from 66% to 101%26. Our long-term outcomes concluded that the procedure improves the femoral head coverage ratio and may contribute to remodeling the hip joint. Daly et al. performed Shelf acetabuloplasty and observed that the femoral head coverage ratio decreased from 83% to 75%5. In our study, the femoral head size ratio increased from 1.13 preoperatively to 1.19 at the last follow-up. This result can be associated with the development of coxa magna in the follow-ups. In our study, the subluxation ratio decreased from 1.66 to 1.23. Chang et al. performed Shelf acetabuloplasty, and in this study, the subluxation ratio decreased from 1.6 to 1.1725. It was shown that the Sharp angle in Perthes hips is steeper than the unaffected side during the course of the disease27. In our study, the Sharp angle decreased from 46.76° preoperatively to 35.77°and the CE angle increased from 14.30° to 40.07°. Ghanem et al. performed Shelf acetabuloplasty in severely affected patients, and the Sharp angle decreased from 45° preoperatively to 35° postoperatively, and the CE angle increased from 12.5° to 44°3. In a study, it was shown that the acetabulum is wider and shallower at all stages of Perthes27. In our study, our results (272 increased preoperatively-308 postoperatively) show that the combined procedure had a stimulatory effect on the acetabular depth growth with the capsular tension effect.
Age at onset is considered one of the most important predictors of prognosis in perthes patients. Obtaining a spherical femoral head and establishing its congruence within the acetabulum is one of the main goals in Perthes disease treatment28. In our study, patients who were ≤ 8 years old at the time of diagnosis were more likely to have a lower Stulberg class, better outcomes, and lower Tönis class, but the differences were not statistically significant (Table 3).
If hinge abduction develops in LCP disease, hip containment is impaired. In this situation, valgus extension osteotomy is an effective method used as a salvage procedure. It is a procedure that reduces the uncovered femoral head into the hip joint and obstructs impingement during the abduction. One of our goals was to induce hip remodeling with this procedure, which we performed in cases where the acetabular growth capacity continued, and the triradiate cartilage was open.
The study has some limitations. The lack of a control group, the relatively small number of patients, and the retrospective study design are some limitations of our study. However, the follow-up was 15 years, which was long enough to evaluate the clinical and radiographical combined surgical procedure. In addition, this study has limited value for femoroacetabular impingement evaluation.
Many reports emphasized that severely affected hips in LCP had poor outcomes. In our study, we aimed to increase joint congruency and achieve satisfactory clinical results. It improved hip functional scores at skeletal maturity and relieved pain scores dramatically. We concluded that valgus extension osteotomy combined tectoplasty procedure in severely affected hips with hinge abduction is an effective treatment method and had satisfactory 15-year follow-up outcomes. Our method could be an alternative treatment option for late-stage Perthes patients.

