











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Lung transplantation (LT) serves as a therapeutic recourse for individuals grappling with advanced lung diseases of diverse origins1. The global prevalence of chronic respiratory diseases has surged, encompassing over 540 million people, marking a substantial 39.8% increase since 19902. Concurrently with this surge, there has been a documented increase in the establishment of specialized LT centers and a corresponding enhancement in the availability of organs for transplantation2,3. Despite its efficacy, LT outcomes, particularly in terms of survival, exhibit variability contingent on the underlying disease and generally manifest at lower rates compared to the transplantation of other solid organs such as the heart, liver, and kidney4.
At present, our understanding of the physiological changes during lung transplants in high-altitude cities is limited5. Altitude-induced physiologic alterations become prominent at elevations beyond 1,500 m above sea level (masl) and intensify with increasing altitudes. Exposure to hypoxia at high altitudes induces physiological changes, including hyperventilation spurred by the hypoxic ventilatory response, leading to an increase in oxygen partial pressure and a decrease in carbon dioxide partial pressure5,6. This is accompanied by heightened heart rate and cardiac output due to sympathetic activation, as well as hemoconcentration6,7. In addition, hypoxia enhances the response to carbon dioxide by lowering the ventilatory recruitment threshold and increasing ventilatory sensitivity to this gas8. At the pulmonary level, non-cardiogenic pulmonary edema may arise due to excessive hypoxic pulmonary vasoconstriction, resulting in an exaggerated increase in capillary pressure and pulmonary arterial pressure6,7.
Given these physiological nuances, it is imperative to compare the results of LT in high-altitude cities with those below 1,500 masl, particularly considering the potential impact of altitude-induced changes on patient outcomes6-8. This study aims to elucidate the survival rates at 1 and 5 years post-transplantation and the clinical characteristics of patients within a high-altitude lung transplant program in Latin America. Furthermore, we seek to juxtapose our clinical findings with the latest publications from the International Society for Heart and LT (ISHLT) and other global groups, thereby contributing to a comprehensive understanding of the unique challenges and outcomes associated with LT in high-altitude settings5,6,8.
Method
This observational analytical single-center study was conducted using data from the institutional registry of patients undergoing LT at La Cardio-Fundación Neumológica Colombiana in Bogota, Colombia, spanning the years 2014 to 2022.
Criteria for eligibility
The eligibility criteria encompassed consecutive patients who underwent LT and had available clinical data during a 5-year follow-up period. Exclusion criteria comprised individuals with incomplete medical history data and those who succumbed within 30 days of hospital admission.
Variables studied
Key variables included age, sex, and clinical characteristics of patients, encompassing the pathology necessitating transplantation, the type of transplant, and short-term complications. Transplant etiologies covered pulmonary fibrosis with a non-usual interstitial pneumonia (N-UIP) pattern, chronic obstructive lung disease (COPD), pulmonary fibrosis with a usual interstitial pneumonia (UIP) pattern, lymphangioleiomyomatosis, bronchiolitis, bronchiectasis non-cystic fibrosis, cystic fibrosis, and others. Survival analysis was conducted, involving patients with a minimum 5-year follow-up post-transplantation.
Sample size
All subjects meeting the selection criteria were included, with consecutive admissions until the study concluded. To minimize biases, an experienced researcher undertook evaluation, transcription, and double verification of the obtained values.
Statistical analysis
Statistical analysis was performed using STATA version 17 software (STATA Corp., Texas, USA). Quantitative variables were summarized by measures of central tendency and dispersion, using means and standard deviations (SD) for normal distributions, medians, and interquartile ranges (IQR), for non-normal distributions. The Shapiro-Wilk test was used to assess normality, considering a value of p < 0.05 as significant. The qualitative variables were summarized in frequencies and percentages. To compare quantitative variables, the Student’s T and Mann-Whitney U-tests were used. According to the distribution of the data, and for the qualitative variables, the Fisher exact test was used. Survival at 1 and 5 years was evaluated through tables, and it was plotted with the Kaplan-Meier method, and the Log-Rank test was used to evaluate the statistical differences in the survival curves, according to the independent variables.
Ethical considerations
The study adhered to international ethical guidelines (Helsinki Declaration, Belmont Report) and national standards (Resolution 8430 of 1993, Colombian Ministry of Health). Patient data confidentiality was maintained in compliance with habeas data law 1266 of 2008, and the research protocol received prior approval from the Ethics and Research Committee (2017-203441) of La Cardio - Fundación Neumológica Colombiana.
Results
Demographic characteristics and key results
Fifty individuals who underwent LT were enrolled, with 56% (28/50) being male, possessing a median age of 54 years (IQR: 39-59 years), and a mean body mass index of 24 kg/m2 (SD: 4.0), as detailed in table 1. Notably, 90% (45/50) of the patients underwent two-LT. The primary indication for LT was pulmonary fibrosis with a N-UIP pattern, accounting for 42% (21/50), followed by COPD at 12% (6/50), and pulmonary fibrosis with a UIP pattern at 10% (5/50). Within the cohort, 20% (10/50) experienced chronic rejection, defined as rejection following two courses of steroid treatment. Throughout the follow-up period, 28% of patients (14/50) were diagnosed with SARS-CoV-2 infection.
Table 1 General characteristics
| Number of patients, n (%) | 50 (100) |
|---|---|
| Male, n (%) | 28 (56) |
| Age, median (IQR) | 54.0 (39-59) |
| Body mass index, mean (SD) | 24 (4.0) |
| Bipulmonar transplant, n (%) | 45 (90) |
| Transplant etiology, n (%) | |
| Pulmonary fibrosis non-UIP | 21 (42) |
| Chronic obstructive lung disease | 6 (12) |
| Pulmonary fibrosis – UIP | 5 (10) |
| Lymphangioleiomyomatosis | 5 (10) |
| Bronchiolitis | 4 (8) |
| Bronchiectasis non-CF | 3 (6) |
| CF | 2 (4) |
| Others causes | 4 (8) |
| mPAP, median (IQR) | 29.5 (24-36) |
| Chronic rejection, n (%) | 10 (20) |
| COVID-19 infection, n (%) | 14 (28) |
| Cause of death, n (%) | |
| COVID-19 infection | 7 (14) |
| Others causes | 13 (26) |
SD: standard deviation; IQR: interquartile range; UIP: usual interstitial pneumonia; CF: cystic fibrosis; mPAP: mean pulmonary arterial pressure.
Overall survival analysis
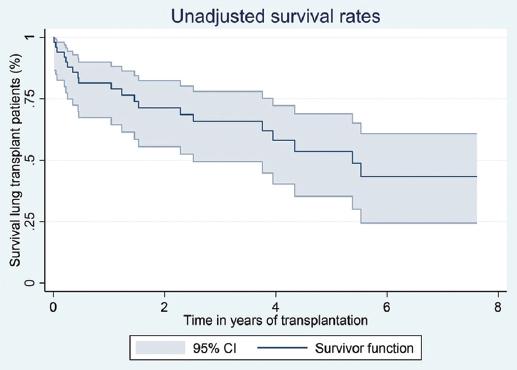
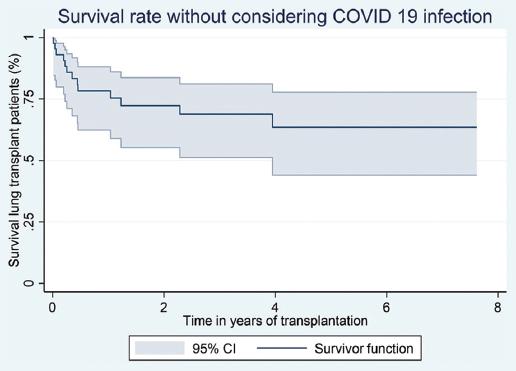
A total of 40% (20/50) of patients succumbed during the follow-up period, with severe COVID-19 identified as the cause of death in 35% (7/20) of cases. The unadjusted survival rates post LT were 81.4% at 12 months, 65.8% at 3 years, and 53.6% at 5 years. On excluding mortality attributed to COVID-19, survival rates remained substantial at 78.2% at 12 months, 68.8% at 3 years, and 63.5% at 5 years (Figs. 1 and 2).
Survival analysis by disease group
An in-depth survival analysis by disease group revealed that pulmonary fibrosis with a N-UIP pattern exhibited a robust survival of 85% at 1 year and 54% at 5 years, while pulmonary fibrosis with a UIP pattern demonstrated a solid survival rate of 80% at 1 year and 60% at 5 years (Fig. 3).
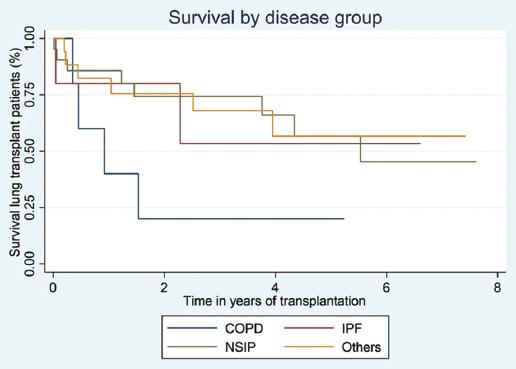
Figure 3 Survival rates after lung transplantation by indication of lung transplant, Kaplan-Meier curve. COPD: chronic obstructive lung disease; IPF: pulmonary fibrosis with a usual interstitial pneumonia; NSIP: pulmonary fibrosis with a non-usual interstitial pneumonia.
Furthermore, within the study cohort, 20% (10/50) of patients developed chronic rejection during follow-up, experiencing a survival rate of 75% at 1 year, with a subsequent decline to 50% at the 5-year mark.
Discussion
In this publication, we share insights from a lung transplant reference center situated in a high-altitude city. Our findings reveal an elevated survival rate among patients with pulmonary fibrosis featuring a N-UIP pattern after 1 year of follow-up. Interestingly, at the 5-year mark, those with pulmonary fibrosis featuring a UIP pattern exhibited the highest survival. When excluding patients who succumbed to COVID-19, survival increased to 68.8% at 3 years and 63.5% at 5 years of follow-up. Furthermore, patients experiencing chronic rejection during follow-up demonstrated lower survival rates compared to those without chronic graft rejection.
Post-transplant survival has demonstrated improvement over time, although it remains inferior to that reported for other solid organs. This discrepancy may stem from diverse factors, including recipient and donor characteristics, the dynamics of donor-recipient interaction, surgical methodologies, and the expertise of the transplant center9-12. Yet, limited research has delved into the impact of high altitude, with no available publications on high-altitude centers. Our resident population at a high altitude (2,640 meters above sea level) exhibits physiological adaptations to hypoxia, such as hyperventilation, hemoconcentration, pulmonary vasoconstriction, increased intracellular oxidative enzymes, and heightened muscle capillary density13,14. These altitude-induced adaptations may prompt distinct physiological responses in patients undergoing LT, potentially influencing outcomes.
Our patients’ overall survival in the 1st year of follow-up was 81.4%, and when severe COVID-19 was excluded as a cause of death, it was 78.2%. These figures closely align with the ISHLT report, reflecting survival rates near 80% at 1 year5. Comparative analyses with other cohorts, such as the Balsara group, reveal similar values11. Survival rates for patients with N-UIP pulmonary fibrosis in our study were 85% at 1 year and 54% at 5 years, surpassing those reported by the Balsara et al. (78.5% and 51.6%, respectively)11.
For residents at high altitude, chronic physiological adaptations to the local conditions seem to have no discernible impact on transplantation outcomes9-14. Conversely, patients referred from lower altitudes undergo pulmonary rehabilitation processes before transplantation, potentially facilitating their adaptation to high altitude – a phenomenon documented in individuals engaging in sports activities at elevated altitudes6.
Examining our study population, the median age was 54 years, aligning with the ISHLT registry data indicating a median age of 55 years for lung transplants as of 20,103. Comparisons with other cohorts often reveal median ages close to 50 years3,11. Notably, our center predominantly performs lung transplants for pulmonary fibrosis with a N-UIP pattern, diverging from other populations where chronic obstructive pulmonary disease and cystic fibrosis are more prevalent indications3,15. This divergence can be attributed to our center’s role as a national reference, resulting in fewer adult patients with cystic fibrosis compared to those with progressive fibrosing pathologies.
Critical to post-transplant success is adherence to immunosuppressive treatment. In our center, the immunosuppression protocol involves tacrolimus as a calcineurin inhibitor, mycophenolate as a cell cycle inhibitor, and prednisolone as a corticosteroid – an approach in accordance with international recommendations for lung transplant patient management16,17.
Limitations
Strengths of this study include the assurance of complete follow-up for all 50 included patients, marking the inaugural publication from a reference center situated at high altitude. Nevertheless, limitations arise from the modest sample size inherent to compiling the experience of a single reference center dedicated to LT at high altitude. In addition, the 14% mortality rate due to severe COVID-19 during follow-up introduces a potential constraint on the interpretability of our study results. Despite being a observational study based on medical records, measures were implemented to minimize information bias, such as the training of the personnel in charge of collecting medical data and the construction of the manuscript based on the checklist of items that should be included in cohort study reports (Table 1). Our results align closely with publications from the ISHLT and low-altitude lung transplant centers5.
Conclusions
In our investigation, patients with pulmonary fibrosis with a N-UIP pattern demonstrated superior survival after 1 year of follow-up, while those with pulmonary fibrosis with a UIP pattern exhibited the highest survival at the 5-year mark. Significantly, the exclusion of patients who succumbed to COVID-19 resulted in improved survival rates at both the 2-year and 5-year follow-up intervals.

