











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Aneurysmal bone cyst (ABC) diseases are known as benign tumors and tumor-like formations of the bone that involve the musculoskeletal system and cause disease, especially in children and young people in the first two decades, causing pain, pathological fractures, deformity in the extremity, functional loss, and neurological problems depending on the site of involvement1-3. In these diseases, the etiology of which has not yet been determined and can cause destructive bone lesion, conditions such as delay in diagnosis and inadequate or inappropriate treatment cause serious increases in national health expenditures together with high rates of morbidity. Although cystic bone lesions are common lesions encountered by all orthopedic physicians throughout their professional life, the fact that many benign and malignant tumors and tumor-like lesions are included in the differential diagnosis may put a physician in a difficult position to reach the correct diagnosis and treatment. Preservation of maximum function is essential in treatment, and percutaneous and minimally invasive surgeries are increasingly gaining prominence as the first choice in some of these diseases4,5.
In musculoskeletal disorders, C-reactive protein, sedimentation, and complete blood count are common tests routinely requested by physicians in the first stage, in addition to radiology and clinical findings, while diagnosing the disease. However, despite all these developments, difficulties in diagnosis sometimes persist, routine laboratory findings are often insufficient in evaluating the prognosis of these patients, and determining the course of treatment and the morbidity of the disease creates problems for physicians1. Molecules that have been studied in recent years such as apelin, adropin, irisin, presepsin, dynamic thiol/disulfide balance, and visfatin have been found to play a role in the pathogenesis of many diseases. For this purpose, studies are carried out on various molecules and enzymes. With the developing medical technology and treatment options, new methods are gaining more and more importance in determining the course and prognosis of musculoskeletal diseases4,5.
Visfatin, an adipocytokine secreted from adipose tissue, has been found to be decreased in numerous inflammatory diseases2. Given that ABC are associated with inflammation, we hypothesized that visfatin might also be involved in this condition. This is a prospective study and visfatin values of patients with ABC s were compared with those of healthy individuals.
Method
Patients and groups
This study consists of patients diagnosed with ABC, who applied to the orthopedics and traumatology clinic of Dicle University Faculty of Medicine. Our study consists of 20 patients diagnosed with ABC (Group 1) (Fig. 1) and 30 healthy patients (Group 2). Age, gender, cyst sizes, and visfatin values of all patients were recorded and evaluated.

Visfatin measurement
For the visfatin test, the blood was taken into flat biochemistry tubes, centrifuged, serum separated, and stored in a deep freezer at −80°C. Enzyme-linked immunosorbentassay (Human Elabela ELISA, Human Visfatin ELISA) method was used for the visfatin test. Serum visfatin levels were measured using the BioTek ELx50 Microplate Washer and BioTek ELx800 Microplate Reader (BioTek Instruments, Inc. USA) devices in accordance with the commercially obtained kit content (E Visfatin; Elabscience Biotechnology, USA. Catalog No: E-EL-H1763).
Inclusion criteria
Patients who were diagnosed with ABC, whose visfatin value was studied at the time of diagnosis, and who agreed to participate in the study and healthy individuals were included in the study.
Exclusion criteria
The presence of another disease that could affect the concomitant visfatin value at the time of diagnosis was accepted as exclusion criteria.
Ethical approval
Ethical approval was obtained from the Local Ethical Committee of the Dicle University with number 385/2021.
Statistical analysis
Statistical analysis was performed for patient data, including descriptive statistics, frequency, and other characteristics for all categories. Continuous data were expressed as mean ± standard deviation. Continuous variables were analyzed with the Shapiro-Wilk and Kolmogorov-Smirnov tests to determine whether the data fit the normal distribution. Continuous and normally distributed variables were compared using Students t-test. Non-parametric tests were chosen when the data were not normally distributed. Correlation analysis was performed by Pearson correlation test. Analyses were performed using the Statistical Package for the Social Sciences Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY, USA). All p-values were considered two-sided and p ≤ 0.05 was statistically significant.
Results
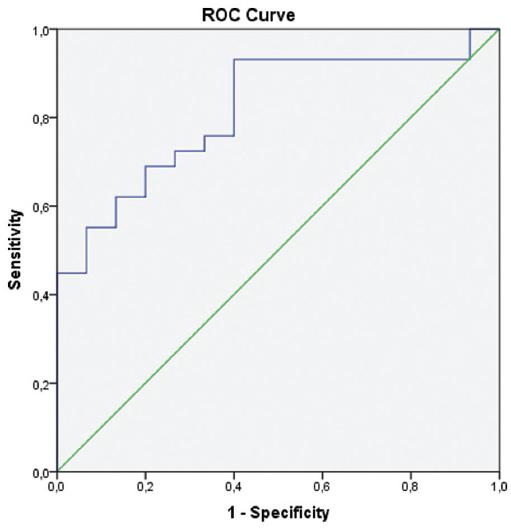
A total of 50 patients, 20 from Group 1 and 30 from Group 2, were included in our study. The mean age was 13.80 ± 3.98 years in Group 1 and 14.67 ± 4.24 years in Group 2, and no statistically significant difference was found between the groups (p > 0.05). While 60% of the patients in Group 1 were male, in Group 2, 53% of the patients were male. The cyst area was recorded as 1171 (512-2310) mm2. Our results show that the visfatin value was 10.70 ± 5.91 ng/mL in Group 1 (ABC) and 15.23 ± 5.86 ng/mL in Group 2 (control group). The visfatin value in the ABC group was found to be statistically significantly lower than the control group (p < 0.05) (Table 1). No correlation was found between cyst area and visfatin (p > 0.05) (Table 2). To determine the diagnostic value of visfatin in ABC s, a ROC analysis was performed. The area under the ROC curve (AUC) was 0.81, suggesting a good diagnostic performance. The optimal cutoff value for visfatin was determined as 8.2 ng/mL, which yielded a sensitivity of 93% and a specificity of 60% (Fig. 2).
Table 1 General findings
| Characteristics | Group 1 (n = 20) | Group 2 (n = 30) | p |
|---|---|---|---|
| Age | 13.80 ± 3.98 | 14.67 ± 4.24 | > 0.05 |
| Gender (male) | 60% | 53.3% | > 0.05 |
| Cyst area (mm2) | 1171 (512-2310) | ||
| Visfatin (ng/mL) | 10.70 ± 5.91 | 15.23 ± 5.86 | < 0.05 |
| Median (IQR) |
IQR: interquartile range.
Discussion
ABCs are benign lytic bone lesions that are typically found in kids and teenagers. A simple bone cyst is a fluid-filled, or partially separated lesion that is cystic in nature. The traditional ABC is a large, hemorrhagic tumor that typically exhibits a distinctive translocation. A third of ABCs, without translocation, is secondary and develops in response to another, typically benign, bone lesion. ABCs are a challenging lesion that can be confused for other diseases1.
Visfatin is a new insulin-like adipocytokine secreted from adipose tissue. Visfatin, otherwise named nicotinamide phosphoribosyltransferase (NAmPRTase or Nampt), is also known as pre-B cell colony-enhancing factor 1 (PBEF1). Nampt/PBEF/visfatin was originally cloned as a putative cytokine shown to enhance the maturation of B-cell precursors in the presence of interleukin-7 and stem cell factor; it was therefore named "pre-B cell colony-enhancing factor" (PBEF)4.
In a study by Chan et al. with 20 gestational diabetes mellitus (GDM) and 20 normal healthy pregnant women, serum visfatin levels were found to be significantly lower in women with GDM compared to the control group6. In comparison to controls, osteoarthritis (OA) patients have higher levels of circulating and local visfatin, with levels in OA synovial fluid being higher than paired OA plasma. As compared to control samples, it has been demonstrated that OA cartilage and synovium release more visfatin. In addition, OA IPFPs express visfatin at levels higher than the relating subcutaneous adipose tissue7. According to Gonzalez-Gay et al.,8 finding's the serum visfatin level in rheumatoid arthritis is not associated with the level of inflammation or the severity of the disease. In the research carried out by Sezen et al.,9 it was found that the visfatin level in the serum samples taken from Behcet's patients was significantly lower than that of the healthy control group. This probably plays a role in the pathogenesis of inflammatory diseases.
The most significant limitations of our research are the limited sample size (a relatively small number of patients participated), the fact that it was carried out only in a single location, and the fact that the healthy participants made up the control group. However, to the best of our knowledge, this study is the first prospective controlled study investigating the diagnostic value of visfatin in ABCs in pediatric patients.
In our study, a total of 50 patients, 20 from Group 1 and 30 from Group 2, were included. Cyst area was recorded as 1171 (512-2310) mm2. The visfatin value was 10.70 ± 5.91 ng/mL in Group 1 and 15.23 ± 5.86 ng/mL in Group 2. The visfatin value in the ABC group was found to be statistically significantly lower than the control group (p < 0.05). No correlation was found between cyst area and visfatin (p > 0.05). Our findings suggest that visfatin may serve as a potential biomarker for ABCs. The ROC analysis revealed an AUC of 0.81, indicating a good diagnostic ability of visfatin, with a high sensitivity of 93% at a cutoff value of 8.2 ng/mL. However, the specificity was relatively low (60%), suggesting that while visfatin is good at detecting the presence of ABCs, it may also indicate other conditions. Further studies are needed to confirm these findings and to investigate the exact role of visfatin in the pathogenesis of these cysts.
Conclusion
Our study found that visfatin levels are significantly lower in patients with ABCs compared to healthy controls, suggesting its potential as a diagnostic biomarker. The ROC analysis showed a good diagnostic ability of visfatin with an AUC of 0.81, a sensitivity of 93%, and a specificity of 60% at a cutoff value of 8.2 ng/mL. More research is needed to confirm these results and to further explore the clinical significance of visfatin in the context of ABCs.

