











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Inguinal hernia is a frequently encountered problem among pediatric patients requiring surgical intervention that occurs due to failure of processus vaginalis closure1-4. Its incidence is approximately 1-5% in full-term babies, and it is 6 times more common in boys5.
Understanding the surgical procedure thoroughly during a case enhances the anesthesiologists' vision of the anesthetic and analgesic techniques and algorithms they are to use. The open procedure of herniotomy involves separation of the hernia sac from the neighboring structures such as cremasteric muscle, round ligament, vas deferens or the testicular vessels; through a peritoneal incision6. There are different options in inguinal hernia surgery, such as laparoscopic and open surgeries. Open surgery is generally recommended for boys, unilateral female hernias, premature newborns, unsuccessful laparoscopic repairs, patients with comorbidities, and cases where technical equipment is inadequate7.
A complicated fiber network from the ilioinguinal (II), iliohypogastric (IH), and genitofemoral (GFN) nerves innervates the inguinal region. The origin of II and IH nerves is the first lumbar (L1) spinal nerve root, sometimes with addition from the 12th thoracic nerve root. Besides, L1 and L2 nerve roots make up the GFN8. Therefore, where one targets efficient pain control for inguinal hernia repair surgery, sensorial blockage of the cutaneous branches of subcostal (T12), ilioinguinal (L1), and iliohypogastric (T12-L1) nerves becomes vital. These nerves run in the transversalis fascia before entering the plane between the transversus abdominis and internal oblique muscles. After passing through the transversus abdominis plane, these nerves emerge into the plane between the external and internal oblique muscles and finally provide the lateral cutaneous branches8,9.
Although herniotomy is an outpatient surgery, severe pain may occur in the post-operative period and relief of post-operative pain is multifactorial10. Transversalis fascia plane (TFP) block has been favored during several procedures like inguinal herniotomy, C/S and iliac crest bone harvesting in adult population, so far11-14. In 2018, the first report on TFPB application after C/S was published, where effective post-operative analgesia was guaranteed15. The first pediatric report of TFP block was by Ahiskalioglu et al. in two different cases; reimplantation of the ureter into the urinary bladder and unilateral inguinal herniorrhaphy operations16.
We hypothesized that performing TFP block would be more efficient for analgesia compared with the standard analgesia protocol. The primary goal of this study is to evaluate the effect of TFPB on post-operative analgesia scores in the pediatric population having open inguinal hernia repair surgery. The secondary aims are to investigate analgesic consumption and parent satisfaction.
Method
The Ethical Committee of Ataturk University's ethical approval was attained for this prospective randomized study 29/11/2018-7/3), and registration bofore patient enrollment with a clinical trial registry (ClinicalTrials.gov, NCT04272320) on February 17, 2020, was performed. Sixty American Society of Anesthesiologists (ASA) Classification I-II patients aged 1-8 years who had unilateral open inguinal hernia repair surgery from September 2021 to January 2022 were included in the study. The patients with a history of clinically significant cardiac, hepatic, renal, or neurological dysfunction, coagulopathy, known allergies to amide local anesthetics, and systemic or local infection at the puncture site were to be excluded from this study.
Patients were randomly assigned to two equal groups using Microsoft Office 365 Excel (Microsoft, Redmond, WA, USA) with the RAND function. In the operating room, an anesthesiologist who was not involved in the study used and opened an opaque sealed envelope. Patients were assigned at random to either the TFP block group (Group TFPB, n = 30) or the control group (Group C, n = 30). Patients were assigned at random to either the TFP block group (Group TFPB, n = 30) or the control group (Group C, n = 30) on the basis of the patient randomization chart.
For premedication, 15 min. before transfer to the operation room, 0.03 mg/kg midazolam was given to patients with IV access. For the ones without IV access, 1 mg/kg oral midazolam was given 30 min. before transfer to the operation room. Vascular access was obtained (22 or 24-gauge IV) after induction with sevoflurane and loss of the eyelash reflex. On delivery in the operation room, heart rhythm and heart rate by electrocardiogram, non-invasive blood pressure measurement, and peripheral oxygen saturation (SpO2) were monitored, and end-tidal CO2 (EtCO2) was recorded intraoperatively. Induction of anesthesia was performed with sevoflurane, Fentanyl 1 μg/kg, and Rocuronium 0.6 mg/kg, then rapid serial intubation was carried out. After intubation, ventilation parameters were adjusted to meet these values; EtCO2 of 30-35 mmHg, FiO2 of 50%, tidal volume 6-7 mL/kg, and ventilation support was initiated. Anesthesia maintenance was provided with sevoflurane (Sevorane, Abbott) 2-3% and rocuronium 0,1 mg/kg intermittently if necessary. Before extubation, all patients were given atropine and neostigmine for reversal as clinical routine practice.
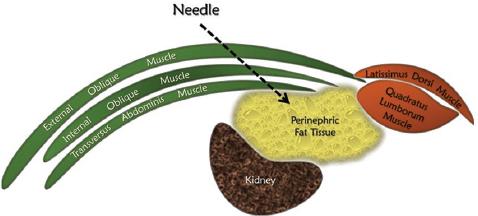
For Group 1 patients, after intubation, a TFP block was performed under aseptic conditions with XperiusTM US systems (XperiusTM Ultrasound System, B. Braun, Melsungen, Germany) with high-frequency linear ultrasound (L12-4 MHz). The patients were placed in the supine position, and the ultrasound probe was placed in a transverse orientation on the abdominal wall so that the external and internal oblique muscles and transverse abdominis muscles were all included in the ultrasound image. Moving the probe laterally, perinephric fat layer, transversalis fascia, and quadratus lumborum muscle were visualized. The sonovisible 50 mm needle was advanced until its tip reached the perinephric fat layer, and after ensuring negative aspiration of blood 0.5-1 mL of 0.9% NaCl as a test dose of was used to confirm appropriate needle tip placement. 0.25% bupivacaine of 0.5 mL/kg volume was used for this procedure (Figs. 1 and 2).
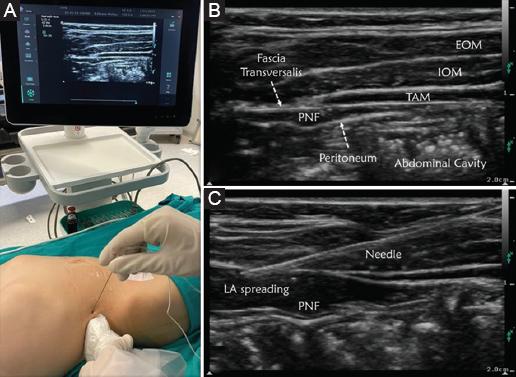
Figure 1 A: patient and ultrasound set-up for TFP block. B: sonographic landmarks. EOM: external oblique muscle; IOM: internal oblique muscle; TAM: transversus abdominis muscle; PNF: perinephric fat. C: transversalis fascia plane block after local anesthetic injection and needle trajectory.
For patients in Group 2, standard analgesia protocol was used, and wound infiltration was applied with 0.2 mL/kg volume of 0.25% bupivacaine before surgical incision.
Surgical procedures
The surgical procedure began with an incision along the inguinal skin crease. On exploration, a hernial sac was discovered without any opening in the inguinal canal. High ligation was carried out using one transfiction and one free ligation. Subsequently, the surgical procedure concluded by suturing the subcutaneous tissue and the skin separately using interrupted sutures.
Post-operative analgesia management
All patients received 15 mg/kg paracetamol every 6 h. The primary outcome of this study was designed to be FLACC pain scores postoperatively, at 30 min., 1, 2, 4, 6, 12, and 24 h. Patients with FLACC > 4 in post-anesthesia care unit (PACU) were given 1 mcg/kg fentanyl intravenous, repeated after 10 min if necessary. Patients with FLACC > 2 in the ward received 7 mg/kg oral ibuprofen. Opioid consumption at PACU and ibuprofen consumption at the ward were recorded. A 3-point Likert scale (1: poor, 2: fair, 3: good) was used to measure parental satisfaction at the 24th h. Data at the 24th h were obtained by calling the parents by phone. Other side effects were also recorded (block-related complications, local anesthetic toxicity, motor weakness, and vascular or abdominal organ puncture).
Sample size and statistical analysis
Conducting a pilot study, the required sample size was determined. The pilot study indicated that our primary outcome, mean FLACC score at the first post-operative hour, should be 2.20 ± 1.65 in the control (n = 10) and 0.95 ± 0.55 in the TFP block group (n = 10). Hence, in total, a sample size of 27 was calculated for the groups through G*Power version 3.1.9.2 (Heinrich Heine University Düsseldorf) with an effect size of 1.016, an α probability of 0.05, and a power of 0.95. Assuming possible dropouts, we decided to include 30 patients in each group.
Statistical Analysis was completed with the SPSS 20.0 for Windows' (SPSS Inc., IL, ABD) program. The data were checked to fit into a normal distribution using the Kolmogorov–Smirnov test. Data that fit the normal distribution were evaluated with an independent sample t-test. Data that did not fit the normal distribution were evaluated using the Mann–Whitney-U test. Categorical data were evaluated using the X2 or Fisher's exact tests. Values of p < 0.05 were significantly meaningful.
Results
A total of 75 patients were assessed for enrollment in this study, 11 of those did not meet the inclusion criteria while 4 of them did not agree to participate and were therefore excluded from the study. In the end, 60 patients were randomly allocated in two groups of 30 patients each. In Fig. 3, the CONSORT flow diagram of participants is demonstrated. There is no statistically significant difference between groups regarding demographic data, ASA classification, anesthesia duration, and operation time (p > 0.05) (Table 1).
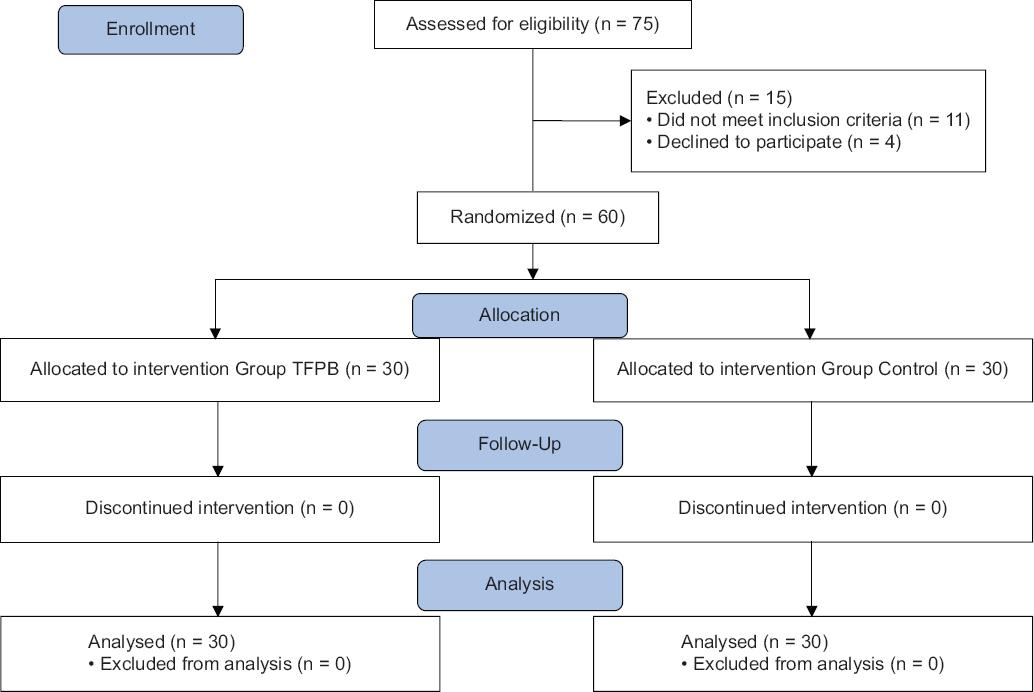
Table 1 Demographic data and comparison of operative procedures between groups
| Variables | Group TFP (n = 30) | Group control (n = 30) | p |
|---|---|---|---|
| Age (years) | 4.25 (2.25-6) | 5 (2.5-8) | 0.583* |
| Weight (kg) | 16.5 (11-23) | 18.5 (11-24.5) | 0.640* |
| Height (cm) | 111 (97.5-127.5) | 122.5 (95-140) | 0.414* |
| Gender (f/m) | 11/19 | 9/21 | 0.785** |
| ASA (I-II) | 27/3 | 29/1 | 0.612** |
| Duration of anesthesia (min) | 45 (40-50) | 40 (32.5-45) | 0.052* |
| Duration of surgery (min) | 27.5 (20-30) | 30 (20-30) | 0.659* |
*p > 0.05 Mann–Whitney U-test.
**p > 0.05 Fishers exact test. Values are expressed median (25-75%) or number, ASA: American Society of Anesthesiologist. Kg: kilogram; cm: centimeter; f: female; m: male; min: minutes.
FLACC scores in PACU at 1, 2, and 4, h were statistically lower in Group TFP. At 8, 12, and 24 h, there is no significant difference between the groups. Opioid consumption in PACU was statistically higher in the control group than in the TFP group (12/30 vs. 3/30, respectively, p = 0.015). The rate of ibuprofen usage at the ward was higher in group control than in group TFP (11/30 vs. 2/30, respectively, p = 0.010) (Table 2)
Table 2 Comparison of the FLACC score assessment between groups
| Variables | Group TFP (n = 30) | Group control (n = 30) | p |
|---|---|---|---|
| Flacc PACU | 0 (0-1) | 3 (2-5) | < 0.001* |
| Flacc 1st | 0 (0-0) | 2 (1-3) | < 0.001* |
| Flacc 2nd | 0 (0-0) | 1 (0-2) | 0.001** |
| Flacc 4th | 0 (0-0) | 0 (0-1) | 0.03** |
| Flacc 8th | 0 (0-0) | 0 (0-0) | 0.429*** |
| Flacc 12th | 0 (0-0) | 0 (0-0) | NS |
| Flacc 24th | 0 (0-0) | 0 (0-0) | NS |
| Opioid consumption (Y/N) | 3/27 | 12/18 | 0.015**** |
| Ibuprofen in ward (Y/N) | 2/28 | 11/19 | 0.010**** |
*p < 0.001 Mann–Whitney U-test.
**p < 0.05 Mann–Whitney-U test.
***p > 0.05 Mann–Whitney U-test.
****p < 0.05 Fishers Exact test. Y: yes; N: no. Values are expressed median (25-75%) or number. PACU: post-anesthesia care unit.
There was no statistically significant difference between the groups regarding post-operative nausea and sedation scores. (p = 0.671 and p = 0.518 respectively). Parents' satisfaction at the end of 24 h was significantly superior in the TFP group (p < 0.001) (Table 3).
Table 3 Comparison of the parents satisfaction and side effects between groups
| Variables | Group TFP (n = 30) | Group control (n = 30) | p |
|---|---|---|---|
| Parents satisfaction (f/g/e) | 2/12/16 | 10/18/2 | < 0.001* |
| Nausea (Y/N) | 2/28 | 4/26 | 0.671** |
| Sedation (I/II/III) | 23/6/1 | 19/9/2 | 0.518** |
*p < 0.001 Fishers exact test.
**p > 0.05 Fishers exact test. Values are expressed as a number. F: fair; g: good; e: excellent; Y: yes; N: no; I: awake and alert; II: quietly awake; III: asleep but easily roused.
Discussion
According to the findings of the current study, performing a TFP block before surgical incision was associated with lower post-operative pain scores in the early post-operative period, less need for rescue opioid consumption, lower post-operative ibuprofen requirements, and higher parental satisfaction than the wound infiltration group.
During the surgical treatment, the surgeon chose not to open the inguinal canal and instead performed a high ligation technique. The incision was confined to the subcutaneous tissue and skin, and the suturing process involved closing the hernial sac, subcutaneous tissue, and skin in a nearly identical manner. It is important to note that all of these tissues are associated with the peripheral nerves of the abdominal wall, not the visceral pleura. While a transversus abdominis plane (TFP) block may not provide visceral analgesic effects, it does have analgesic activity for the structures of the abdominal wall.
Technical simplicity, selective unilateral blockage, lower risk of complications, and comparable or better analgesic outcomes are some of the advantages of interfascial plane blocks on the contrary of neuraxial anesthesia or nerve plexus blocks. Caudal anesthesia is a common neuraxial technique that can be used for perioperative analgesia during open hip surgeries and inguinal herniorrhaphy. However, there are possible complications such as intravascular or intrathecal injection, convulsions, hemorrhage in the retroperitoneal region, urine retention, or renal puncture.17 Moreover, it leads to a bilateral block that might be undesirable for unilateral hernia repair operations where TFPB would be a proper alternative. Caudal anesthesia is commonly employed for herniotomy to provide effective post-operative analgesia. Anesthesia providers often utilize landmark techniques for this purpose. It is important to note that caudal anesthesia affects both sides of the body. However, unintended complications such as intravascular or intrathecal injections, convulsions, or urine retention may arise. On the other hand, the TFP (Transversus Abdominis Plane) block is performed under ultrasound guidance, enabling clear visualization of anatomical structures. This allows for simple and safe injection administration.
Before the advancement of ultrasonography guidance in regional anesthesia, the blind technique was used for TFP block as follows: 1 cm medial to the anterior superior iliac spine is defined as the suitable puncture side; the needle is advanced until a "pop" is felt as it passes through the external oblique muscle. However, this technique had a very unpredictable success rate18. Following the revolutionary introduction of point-of-care ultrasound guidance in regional anesthesia, the acquisition of this skill enabled practice with superior efficacy and safety as local anesthetics could be administered as close as possible to target nerves. A few studies have demonstrated ultrasound guided TFP block's efficacy in different procedures. According to the study by Aydın et al., TFP block is effective in lowering opioid consumption significantly at all-time intervals during the 24-h follow-up in women who underwent cesarean section under spinal anesthesia19.
In another study carried out in 2020 by AbdelBaser et al., 44 patients aged 12-60 months were included to evaluate the preemptive analgesic efficacy of TFP block. In correlation with the results obtained from this study, it demonstrated that TFP block application is associated with decreased post-operative analgesic consumption (paracetamol and fentanyl), lower post-operative pain scores recorded also with the FLACC scale, lower need for rescue analgesia, and enhanced parental satisfaction than the control group in pediatric patients as well8. The follow-up period was limited to 12 h in this study while we recorded pain scores for 24 h. This study compares an actual sham group with a TFP block. Unlike in this study, the control group of our study received wound infiltration rather than sham injection. Despite the fact that the control group had low pain scores, the TFP block provided more effective analgesia in the early post-operative period.
Before performing TFPB, possible risks and complications must be studied and discussed. In order to avoid local anesthetic systemic toxicity, maximum doses of local anesthetics should not be exceeded, keeping in mind the physiological and pathological factors of each patient that may influence their metabolism, especially in pediatrics. Local anesthetics can be absorbed through the well-vascularized large surface areas of the fascial planes; and less cardiotoxic agents should be preferred ideally. In our study, bupivacaine was used as it is the only commercially available local anesthetic in Turkey that can be used for regional anesthesia. Lee et al. reported a case that demonstrated quadriceps femoris paralysis due to TFPB application after iliac bone grafting20. Local anesthetics administered at the TFP potentially extend over the quadratus lumborum, passing through paravertebral spaces and eventually blocking the roots or branches of the lumbar plexus. In a cadaver study by Rosario et al., this compartment between the transverse abdominis muscle and transversalis fascia was demonstrated to be continuous with the fascia iliaca compartment21. In our study, we did not face any complications related to quadriceps paralysis; however, parents must be informed of the quadriceps weakness risk while consent is being obtained.
Another possible complication linked to abdominal wall blocks is the trauma of the adjacent structures and organs. In performing QLB, there is a possible risk of renal injury because the kidney lies anterior to the QL muscle, separated only by perinephric fat and fascia. As the perinephric fat is smaller in size in pediatric patients, there is a higher risk of injury when QLB is performed on children. Ahiskalioglu et al. reported a case of incidental hepatomegaly during QLB block in a pediatric patient in an effort to emphasize that anesthesiologists should keep in mind that solid organ damage must be avoided in plane block applications22. To minimize peritoneal penetration and liver or kidney trauma, the block area should be posterior enough so that the perinephric fat is underlying the transversalis fascia. Because the site of intervention for TFP block is more posterior than TAP, there is perinephric adipose tissue under the fascia instead of the peritoneum or liver. Hence, the TFP block is considered as a simple block to apply. On the other hand, the need to move the patient into both lateral positions after the surgery is a disadvantage of QLB block19. In this study, none of the patients had any damage to the peritoneum or adjacent organs, and TFPB might be safer, and alternative to QLB for lower abdominal surgery.
In our institution, pediatric surgeons mostly perform open inguinal hernia repair, however, laparoscopy has been highly utilized throughout the world, as well. The advantages of laparoscopy include the ability to visualize contralateral defects, diminished post-operative pain, improved cosmesis, and lower complication rate. Potential disadvantages are proposed to be increased operation time, learning curves, higher incidence of PONV, and need of orotracheal intubation23. In laparoscopy, the periton is penetrated and pneumoperitoneum is required. Therefore, TFP block would not provide adequate intraoperative or post-operative analgesia during a laparoscopic inguinal hernia repair. Hence, it must be noted that laparoscopic surgery might require a more challenging pain control and further techniques must be studied for laparoscopic scenarios where TFP is not adequate.
Genital branch of the GFN partially contributes to the innervation of the inguinal sac, II and IH nerve blocks do not cover this nerve branch which potentially leads to visceral pain due to traction on the hernial sac. Sasaoka et al. demonstrated that GFN block, when applied with II and IH nerve blockade, attenuated the hemodynamic stress response to surgical manipulation of the inguinal hernial sac, but did not have any post-operative analgesic effect24. In the upcoming studies, TFPB accompanied by GFN block could also be compared with other analgesic techniques.
There are some limitations to the study. First, it was not possible to evaluate block success through dermatomal analysis as most children are unable to grasp the concept of paraesthesia, and even if they could, it would still not be possible as the patients were under general anesthesia when the block was being performed. In addition, we could not perform the block technique using the same volume saline solution to Group II patients. However, objectivity was key in this study; the same anesthesiologist performed the block each time, and another blinded anesthesiologist from our department's "Pain Crew" performed the post-operative follow-up.
Conclusion
Through this study, we suggest that ultrasound-guided TFP block provides lower post-operative pain scores in pediatric inguinal hernia repair; furthermore, it is a simple, safe and practical technique. Further studies are warranted to verify these findings and define the block's clinical characteristics better.

