











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Fractures of the proximal humerus are the second most common upper limb fractures in adults and make up 5% of all fractures1. The prevalence of these fractures is highest among the elderly, but the younger, more active population is becoming increasingly susceptible.
Shoulder fractures are fraught with controversy, not only in terms of the indications for surgery (that is, which fractures should or should not be operated on), but also in terms of the surgical procedures and implant choices that should be used for the fixation. Many different methods of treating proximal humerus fractures have been published in the medical literature, but there is still no consensus on the best way to treat these injuries2-6. The purpose of surgery is to achieve anatomic fracture reduction and stable primary fixation to accelerate the healing process and start post-operative rehabilitation as soon as possible, with the least amount of time spent in immobilization as possible7,8.
The most frequently applied methods of osteosynthesis of proximal humeral fractures include minimally invasive techniques using K-wires, sutures and/or screws, plate fixation, intramedullary locking nails, or arthroplasty procedures (partial or reverse prosthesis). The choice of surgical approach is determined by fracture type, patient age, bone quality, comorbidities, and functional requirements2,7,9-12.
The purpose of this study is to analyze the operative treatment of two- and three-part fractures of the proximal humerus, categorized by Neer13, at the Clinic for Orthopedic Surgery and Traumatology, University Clinical Center of Vojvodina in Novi Sad, utilizing plates and screws and intramedullary nailing.
Materials and methods
The study was approved by the Ethics Committee of the University Clinical Center of Vojvodina. This retrospective analysis included 40 patients of both genders with displaced two-part and three-part fractures of the proximal humerus who were surgically treated between June 2010 and October 2019. Classification of fractures was based on a true AP and Y radiograph projection, validated by the same surgeon utilizing Neer classification13. The indication for surgical treatment was made according to the Neer criteria13 −45° of humeral head angulation and 1 cm dislocation of fragments (head, greater, and lesser tubercles and the body of the humerus). Large tubercle dislocations > 5 mm were deemed to be unstable fracture patterns6,14, and were an indication for surgical treatment. The study excluded patients with fractures that involved humeral diaphysis and articular surface of humeral head ("head splitting fractures"), patients with open or ipsilateral fracture of the same arm, polytraumatized patients, patients with neurovascular lesions of the operated arm, and those who had refused to participate in the survey.
Data for analysis were obtained from medical history, as well as during outpatient examinations at the Clinic for Orthopedic Surgery and Traumatology.
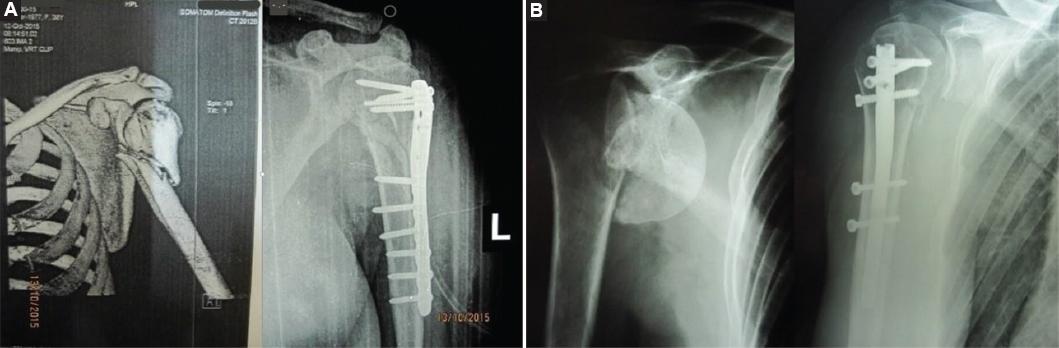
Osteosynthesis of the fracture was achieved using plate and screws or intramedullary locking nail (Fig. 1). Surgery was performed on the radiolucent table with the patient in the "beach chair" position. Deltopectoral approach was utilized for plating of the fractures, whereas the nailing was performed and managed through a minimally invasive anterolateral technique (deltoid splitting approach). During surgery, the position of fragments was verified with C-arm. Regardless of the type of osteosynthesis, post-operative Desault immobilization was indicated for a period of 4-6 weeks, with the upper arm in 45° of abduction, elbow in 90° of flexion, and neutral rotation of the forearm. The duration of immobilization depends on the fracture pattern, the patient´s age, the quality of reduction, and the fixation strength. For the first 48 h, parenteral antibiotic prophylaxis, which included first-generation cephalosporins, was administered. Post-operative X-rays were made 10 days, after the surgery, after 3 and 6 weeks, 3 and 6 months postoperatively. The mean follow-up time was 4 years (1-9 years). All patients were operated on by the same surgeon.
We evaluated the results of treatment using Constant´s scoring scale as well as Disabilities of the Arm, Shoulder, and Hand (DASH score)15,16. A goniometer was used to quantify range of motion (ROM), while muscular strength was determined by the amount of kg weight in kilograms, the patient could hold in 90° shoulder abduction16. Values of ROM and muscle17 strength were compared between the operated and healthy shoulder. Constant´s score is the difference between the values obtained after the examination of the healthy and operated shoulder and can be graded as excellent (< 11), good (12-20), fair (21-30), or poor (> 31). The DASH score is a numerical measure that assesses the disability and functional limitations of the upper extremity, including the arm, shoulder, and hand, typically represented on a scale from 0 to 100, with higher scores indicating greater disability and lower function. The obtained results were statistically analyzed using the Student t-test and χ2 test with a significance level of 0.05.
Results
Out of the 40 patients enrolled in this study, 16 were males (40%) and 24 were females (60%). Twenty patients were treated with a plate and screws and 20 with an intramedullary locking nail. We created 10 pairs of patients that were matched in age, gender, and fracture type, with the sole difference being the osteosynthetic material used (10 pairs with two-part dislocated fractures and 10 pairs with a dislocated three-part fracture, where it affected a lesser or greater humeral tubercle). The minimum follow-up time was 1 year.
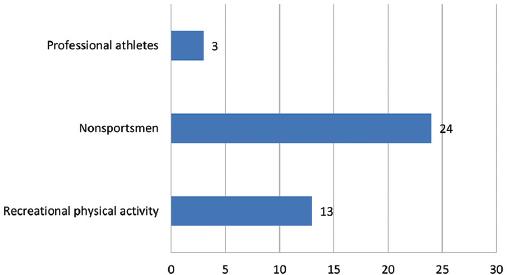
The average age was 58 ± 13 years. The oldest participant was 77 years old and the youngest 28 years old. The average age of patients treated with plate and screw osteosynthesis was 58.2 ± 11.8 years, while the average age of patients treated with intramedullary locking nail was 59.4 ± 12.9 years. Considering the average body mass index (BMI), our sample fell into the overweight category (BMI = 26 ± 5). Of the patients included in study, 22 sustained injuries to their right arm, whereas 18 sustained injuries to their left arm. The dominant hand was injured in 60% of patients. The majority of patients did not engage in any sort of athletic participation activity −24. The large proportion of patients with a humerus fracture was recreational athletes13, whereas only two were professional athletes (Fig. 2). The leading causes of injury in our sample were falls (29 patients, 72.5%), motor vehicle accidents (eight patients, 20%), and recreational activities (three patients, 7.5%). The diagnosis of fractures of the proximal humerus was made on the day that the accident occurred, and the fractures were treated within 7 days of the injury.
The mean value of Constants scoring scale was 78.05 in patients who were treated with plates and screws and 67.55 in patients treated with intramedullary nails. Statistical analysis did not find a significant difference between these two groups, although the Constants score showed higher values in the patient group treated with plates and screws (Table 1).
Table 1 Results of constant´s scoring scale
| Constants scoring scale outcome | Plate osteosynthesis (%) | IM nail osteosynthesis (%) | Total (%) |
|---|---|---|---|
| Excellent | 7 (35) | 5 (25) | 12 (30) |
| Good | 5 (25) | 3 (15) | 8 (20) |
| Fair | 3 (15) | 3 (15) | 6 (15) |
| Poor | 5 (25) | 9 (45) | 14 (35) |
| Mean value | 78,05 | 67,55 | 100 |
| Total | 20 | 20 | 40 |
The values of the DASH score are presented in table 2, and no statistically significant difference is observed between the two groups. The results are largely consistent with the Constant score, with slightly better outcomes observed in the group treated with plates and screws.
Table 2 Results of DASH scoring scale
| DASH scoring scale outcome | Plate osteosynthesis (%) | IM nail osteosynthesis (%) | Total (%) |
|---|---|---|---|
| Minimal to no disability | 13 (65) | 9 (45) | 22 (55) |
| Mild disability | 3 (15) | 3 (15) | 6 (15) |
| Moderate disability | 3 (15) | 5 (25) | 8 (20) |
| Severe disability | 1 (5) | 3 (15) | 4 (10) |
| Extreme disability | 0 | 0 | 0 |
| Total | 20 | 20 | 40 |
DASH: disabilities of the arm, shoulder, and hand.
There was no statistically significant difference in the ROM between groups, although it tended to be larger in the group of patients treated with plate and screw osteosynthesis (Table 3).
Table 3 Range of motion in observed groups
| Motion type | Cumulative range of motion - Plate Group | Cumulative range of motion - Nail Group |
|---|---|---|
| Flexion (°) | 135.45 ± 42.5 | 119.7 ± 45.6 |
| Abduction (°) | 123.4 ± 45.5 | 113.75 ± 45.6 |
| External rotation (°) | 52.25 ± 14.5 | 41.7 ± 18.3 |
| Internal rotation (°) | 65 ± 17.6 | 61 ± 19.2 |
We observed complications in four patients. Superficial wound infection was observed in two patients in the screw and plate fixation group. Chronic pain due to migration of osteosynthetic material was found in two patients treated with intramedullary nail.
During the follow-up, neither delayed union nor non-union was noted in any of the patients.
Discussion
Upper arm fractures are of major significance in contemporary orthopedic trauma because they are one of the most prevalent causes of morbidity and disability in the elderly and can have severe repercussions in young, working populations18. The primary aim of surgical therapy for fractures of the proximal humerus is to achieve anatomic fracture reduction and stable fixation that allows early functional rehabilitation. Modern implants for extramedullary and intramedullary fracture stabilization provide optimum stability, while less invasive surgical techniques promote rapid bone healing and excellent revascularization7,19.
Out of 40 patients included in our study, 20 of them were treated with plate and screw osteosynthesis of the proximal humerus. They achieved Constants score value of 78.05. Südkamp et al.20 studied the outcomes of 1087 patients who received surgical treatment for proximal humerus fractures with plate and screw fixation and observed an average Constant's score of 70.6, which is lower compared to our results.
This disparity in outcome results may be due to the absence of grouping based on fracture type in the aforementioned paper, which included more complex fracture patterns, as well as a significantly larger sample size. This difference in sample size may account for our overestimation of Constant's score in comparison. A recent study21 which retrospectively analyzed 28 patients who were treated with second generation nails reported an average Constant's score of 83.1 at 1-year follow-up. Advances in operative technique over the years resulted in better overall results in patients treated with an intramedullary nail. Guo et al.21 also showed that there was no statistical significance when comparing the nail to the plate and screw fixation.
Gradl et al.22 compared the treatment results of 152 patients who underwent surgery with plates and screws and intramedullary nails. The average value of Constant's scoring scale for plate fixation was 77%, and for nail fixation, it was 81%. Despite the better score value for patients treated with nail fixation, this difference did not reach statistical significance. Trepat et al.23, in their study involving 29 patients, also found no statistically significant difference in results between the two treatment techniques. In a 2016 randomized controlled trial evaluating 72 patients, Gracitelli et al.24 reported that there was no significant mean difference in the Constant-Murley score at the 12-month follow-up (70.3 points for the nail group vs. 71.5 points for the plate group; p = 0.750). Our results indicate no statistically significant difference in outcome between patients treated with plate and screw fixation (78.05) and intramedullary nailing (67.55), confirming the findings of the previously mentioned studies. In contrast to our results, Boileau et al.18 demonstrated a better post-operative outcome in patients treated with plate and screw fixation. They justified their results by emphasizing the importance of accurate reduction and strong fixation of the greater tubercle, leading to smaller/negligible loss of abduction and external rotation, and consequently, better functional results.
In accordance with the findings of prior investigations25, older patients in our study had worse Constant score outcomes. Several studies comparing locking plates to third-generation intramedullary nails concluded that there is a high risk of secondary displacement and fracture non-union in elderly patients with poor bone quality26,27. This can be a consequence of reduced regenerative capacity of the tissues in these patients, reduced motivation, and the presence of comorbidities.
In our study, we included the DASH score as an additional tool for evaluating treatment outcomes in patients with proximal humerus fractures, alongside the commonly used Constant score. We compared the results of the DASH scores between two distinct groups of participants and found that there was no statistically significant difference between them. This finding is in line with previous research on the subject24,28. Furthermore, it is worth noting that the results obtained from the DASH score assessment were consistent with those obtained from the Constant score assessment in both groups of participants.
Lekic et al.29 conducted a retrospective study that included 24 shoulders, divided into equal groups of 12 treated with intramedullary nail osteosynthesis and 12 treated with a locking plate. They assessed the ROM in these patients, specifically forward elevation of the arm, and compared the two groups. The average forward elevation of the arm in patients treated with intramedullary nail fixation was 134° (range, 60-160) and with locking plate was 141° (range, 90-180), showing no statistically significant difference. A similar outcome was observed in flexion (forward elevation) with 119.7° in patients treated with intramedullary nail osteosynthesis and 135.5° in patients treated with plate and screw fixation. In a retrospective study, Schulte et al.30 included 43 patients who underwent plate and screw osteosynthesis. The average flexion in their patients was 140°, and external rotation was 58°, which was comparable to the results we measured: an average flexion of 135.5° and external rotation of 52.2°. For the majority of everyday tasks requiring shoulder flexion and abduction up to 90°, patients in our research were able to fully and independently execute necessary daily activities.
We observed complications in four patients (10%). Superficial wound infections were found in two patients in screw and plate fixation group and were treated conservatively with regular dressing changes and administration of antibiotics. Two patients treated with an intramedullary nail reported the presence of chronic pain, a consequence of the migration of osteosynthetic material. These patients were treated symptomatically with non-steroidal anti-inflammatory drugs and cryotherapy. Upon radiographic evidence of fracture healing union, the osteosynthetic material was removed, resulting in complete pain relief.
Our study showed no statistical difference in the complication rates in either group of patients, but the complications in the nail group required reoperation. Our results are consistent with those of Gracitelli et al.24 who showed a higher complication rate in the nail group with no statistical difference, emphasizing the fact that there were more complications in the nail group that required reoperation.
Lekic et al.29 in their sample of 24 shoulders, 12 had undergone intramedullary nailing, with 5 of them (42%) encountering complications. Two patients in this group (16.6%) had deltoid muscle calcification, which resulted in mild pain: one patient (8.3%) experienced painful heterotopic ossification within the subacromial area and two patients (16.6%) acquired painful hardware in the proximal shoulder.
In the same study, there was also report of locking plate technique complication, in shoulders (33%): screw penetration in joint cavity in (three [25%] and one asymptomatic head osteonecrosis [8.3%]). Our results show a 10% of complication rate, which is substantially lower than found by Lekic et al. (37%). Upon reviewing the paper, we could not find any drastic deviation in the operative protocol (osteosynthesis used or operative approach) nor could we find any significant deviation in the patient sample. Despite the complication observed in this study, all fractures demonstrated complete union by 3 months.
Our results also show that union was achieved in all fractures by 4 months.
Studies that used rigid fixation generally showed an incidence of osteonecrosis of the humeral head ranging from 0% to 25%2,7,9. In our sample, we did not have partial nor complete osteonecrosis of the humeral head. We hypothesize that the higher incidence of osteonecrosis in procedures with rigid osteosynthesis (IMF and LP) may be the result of implant cutout, which can occur in 7-25%29,31, more aggressive tissue dissection, but could also be attributable to the longer follow-up time in these studies. Egol et al.31 identified glenohumeral cutout in 16% of patients following angular stable plate fixation; however, only 50% of these patients underwent revision surgery. The author explains that a high rate of screw penetration can be attributed to poor bone stock. In the case of antegrade nailing, Mittlmeier et al.8 advised not overdrilling the medial cartilage and selecting fixation screws 2-3 mm shorter than planned.
Numerous studies have examined which implant produces the best outcome for specific types of fractures, and they have all reached the same conclusion: with three-part fractures, osteosynthesis with plate and screws yields better outcomes, but with two-part fractures (fractures of the surgical neck), intramedullary nailing yields superior results and faster recovery2,7,13. While analyzing our results, we could neither confirm nor deny the superiority of one particular method, but from clinical experience, we share the same opinion as the above authors. In addition to this conclusion, we emphasize that even though better results are achieved with intramedullary fixation in the treatment of two part fractures, the occurrence of complications when using IM nails in our study showed a greater need for reoperation. These complications increase the risks for patients and the cost of overall treatment.
Constraints of this study include its retrospective nature and its relatively small sample size, both of which may hinder a better understanding of the effectiveness of particular operative techniques. Nevertheless, despite these limitations, the study has provided us with valuable insight and direction for future research.
Conclusion
Our results show that patients with plate and screw fracture stabilization had a higher Constant score, as well as DASH score, than patients where locking intramedullary nail is used, without statistical significance. The same group of patients had a higher degree of mobility compared to those who underwent intramedullary nail surgery but also without statistical significance. All these factors points to plate fixation as a potential superior choice of osteosynthesis. However, due to more frequent complication with plate fixation in the form of implant cutout and osteonecrosis, there is still no consensus on which operative technique and type of implant give the best results in the surgical treatment of these fractures.

