











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Due to the special anatomical position and irregular stereotypical structure of the calcaneus bone, calcaneal fracture surgeries present difficulties related to exposure, reduction, and fixation and are accompanied by many post-operative complications1. The most common complication associated with the surgical treatment of calcaneus fractures is delayed wound healing, likely a reflection of the limited surrounding soft-tissue envelope, as well as the extent of soft-tissue trauma associated with the injury. The most common neurological complication following operative treatment of fractures of the calcaneus is an iatrogenic injury to a sensory cutaneous nerve, particularly the sural nerve, during an extensile lateral approach2. Effective treatment of displaced intra-articular calcaneal fractures is challenging for all orthopedic surgeons. Proper incisions can fully reveal the fractured end of the calcaneal bone and the collapsed joint surface, which is conducive to reduction and fixation and reducing incision-related complications. This is a key to the treatment of displaced intra-articular calcaneal fractures. The extensile lateral L-shaped approach to the calcaneus is the method for surgical fixation of displaced intra-articular calcaneus fractures3,4. Related complications such as incision infection, non-healing incisions, skin necrosis, and nerve injuries are frequently reported4,5, and the occurrence of any problem will affect the patient’s recovery. Although the sinus tarsi approach and the enlarged sinus tarsi approach can reduce incision-related complications, their application has limitations; mainly for Sanders II and III AB type fractures6-8. The coronal view of the calcaneus model was used to demarcate the maximum length of the connection between the talus and calcaneus. This gap between talus and calcaneus is divided into three equal parts through three points: a, b, and c; the lateral point of sustentaculum tali is marked as point c. Based on points a, b, and c, three fracture lines were depicted as A, B, and C according to the Sanders system of classification. The model with double fracture lines (AB, AC, or BC) represented the Sanders Type III (AB, AC, BC) fracture9.
With the continuous development and progress of minimally invasive technology, modified incision of the tarsal sinus can greatly reduce the incision range but has no impact on the full exposure of the subtalar articular surface. Doctors can also perform fracture reduction under direct vision, and this approach can reduce the damage to the blood supply to the foot and ankle. The purpose of the current study was to describe a modified tarsal sinus incision and evaluate the results of open reduction and internal fixation through the modified tarsal sinus incision as a surgical treatment of displaced intra-articular calcaneal fractures.
Methods
Patients and methods
The clinical data of patients with intra-articular calcaneus fractures treated by open reduction and internal fixation through a lateral hook curvy incision from May 2014 to July 2017 were analyzed retrospectively. The inclusion criteria were acute calcaneal fractures (within 2-3 weeks) involving the joints and Type II and III fractures, based on the Sanders classification10. The exclusion criteria were patients with old calcaneal fractures, Type I and IV fractures based on the Sanders classification, extra-articular fractures, and calcaneus fracture of a diabetic foot.
A total of 139 patients with calcaneal fractures admitted to our hospital were retrospectively analyzed. Among them, 13 cases of old calcaneal fractures, 28 cases of Sanders Type I and Type IV fractures, 16 cases of extra-articular fractures, and three cases of diabetic foot were excluded from the study. In 79 patients with calcaneal intra-articular fractures, 25 patients were treated with open reduction and internal fixation using a lateral hook incision.
Among the 25 patients included in this study, 21 were men and four were women. The average age was 44.6 years (range: 25-64 years). The right side was involved in 11 cases, the left side in 10 cases, and bilateral calcaneus fractures were present in four cases. The mechanism of injury was a fall from height in 22 patients and a traffic accident in one case, a heavy pound injury in one case, and falling in one case.
Twenty-five feet had closed fractures, and four cases were open fractures. Two patients had associated lumbar compression fractures and pelvic fractures without surgical treatment. One case had an associated radial fracture with open reduction and internal fixation. One case had an associated lateral malleolar fracture. One patient had an open fracture with a medial soft-tissue defect, and a secondary flap graft was performed to repair the wound.
At the time of admission to the hospital, anteroposterior, lateral, and internal oblique radiographs of the injured foot and an axial radiograph of the fractured calcaneus were taken. A pre-operative CT scan was made for all cases to evaluate the size of the displaced fracture fragments and help the surgeons reduce the displaced fracture fragments. From the plain radiographs, the pre-operative Bohler angle and Gissane angle were measured. The posterior articular surface was divided into three columns by two fracture lines according to the coronal view of CT images. Line C separated the medial fragment from the posterior talar facet of the calcaneus11,12. There were 15 cases of Type II fractures, seven Type IIA, and eight Type IIB. Fourteen cases were Type III fractures, 10 were Type IIIAB, one was Type IIIAC, and three were Type IIIAC. In 18 patients with calcaneal fractures, the calcaneocuboid joint surface was involved. If the wrinkle sign was observed at the lateral side of the heel, surgery was performed.
Patients were clinically evaluated using the AOFAS ankle-hindfoot score (best score = 100 points)6. This clinical rating system combines subjective scores of pain and function provided by the patient with objective scores based on the surgeon’s physical examination of the patient (to assess sagittal motion, hindfoot motion, ankle-hindfoot stability, and alignment of the ankle-hindfoot). The scale includes nine items that can be divided into three subscales (pain, function, and alignment). Pain comprises one item with a maximum score of 40 points, indicating no pain. Function comprises seven items with a maximum score of 50 points, indicating full function. Alignment comprises one item with a maximum score of 10 points, indicating good alignment. The maximum score is 100 points, indicating no symptoms or impairments. The AOFAS score was divided into groups according to the literature: a score of 90-100 was graded as an excellent result, 75-89 as good, 50-74 as fair, and < 49 points was graded as a failure or poor outcome3.
Anatomical basis and design of the modified tarsal sinus incision
Incision design: an incision was made in the side midline of the calcaneus to open the flap on both sides to render calcaneus exposure and operation easier. Accordingly, the central point of the calcaneocuboid joint was A, and the middle point from the bottom of the sinus tarsus to the metatarsal side of the calcaneus was B. A line was made through A and B. Point C was the intersection point of a 1 cm horizontal line in front of the Achilles tendon and a vertical line to the Achilles tendon from 1 cm above the lateral malleolus. Point D was the intersection of the extension line at a 30° angle between point C and the Achilles tendon and the extension line at two points, A and B. Points C, D, and A were connected into a hook curvy incision, which was extended to both ends through points A and C as required (Fig. 1A). The incision line corresponded to the midline of the lateral wall of the calcaneus, which is the approach for exposing the subtalar joint and the calcaneocuboid joint (Fig. 1B).
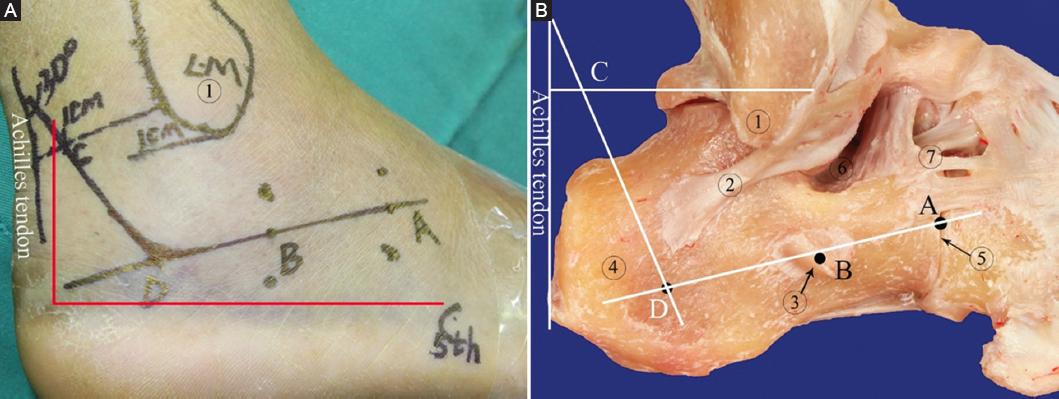
Figure 1 The design of the modified tarsal sinus incision. A: the line ABDC is the lateral hook curvy incision. B: the relationship between the lateral hook curvy incision and calcaneus. a: The midpoint of the calcaneocuboid joint. b: The calcaneal midpoint at the level of the sinus. c: The intersection point of 1 cm horizontal line in front of the Achilles tendon and vertical line to the Achilles tendon from 1 cm above the lateral malleolus. d: The intersection point of slash at a 30 less tendon and vertical line to the Achilles tendon f connection. 1: The lateral malleolus; 2: calcaneofibular ligament; 3: peroneal trochlea; 4: calcaneal tuberosity; 5: Calcaneocuboid joint; 6: Tarsal sinus; 7: Anterior tubercle of calcaneus. The red line is the extended lateral L-shaped approach.
Anatomical basis: the blood supply of the lateral calcaneus region derives from the arterial network comprising the lateral calcaneus artery, sinus tarsus artery, lateral tarsal artery, and basolateral plantar artery, and rich vascular chains form in the skin and subcutaneous tissue (Fig. 2A)13,14. Although the plantar and lateral skin of the heel is supplied by different angiosomes, this is also the anatomical basis of the laterally expanded L-shaped incision. However, there is an extensive vascular network between the two angiosomes at the lateral side and the plantar skin junction of the heel. Anatomical specimens perfused solely through the anterior tibial artery showed an extensive vascular network between the lateral region and pelma of the heel. The skin below the midline of the calcaneus can also obtain blood supply through the traffic branch of the lateral tarsal artery (Fig. 2B).
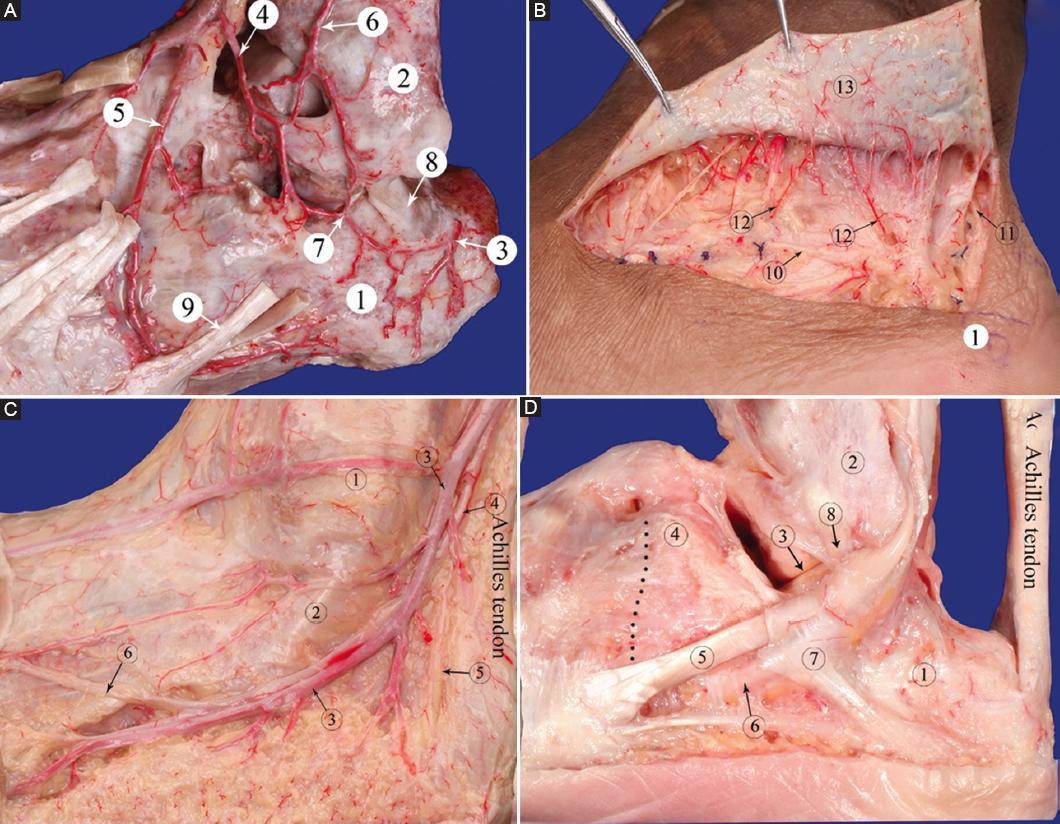
Figure 2 A: the artery network of the lateral area of the calcaneus. B: the extensive subcutaneous capillary network in the proximal end of the hook-curvy incision. C: the sural nerve and less saphenous vein. D: the lateral wall of the calcaneus and the peroneal tendons. 1: Calcaneus; 2: lateral malleolus; 3: the lateral calcaneal artery; 4: tarsal sinus artery; 5: lateral tarsal artery; 6: descending branch of external superior malleolus artery; 7: communicating branches; 8: calcaneofibular ligament; 9: tendon of peroneus brevis; 10: the sural nerve; 11: subdermal vascular plexus; 12: Perforating Vessels. c1: the lateral malleolus; c2: tendon of peroneus brevis; c3: the less saphenous vein; c4: the sural nerve; c5: the lateral calcaneal nerve; c6: lateral dorsal cutaneous nerve of foot. d1: calcaneus; d2: lateral malleolus; d3: the subtalar joint; d4: anterior superior tubercle of calcaneus; d5: tendon of peroneus brevis; d6: Peroneus Longus Tendon; d7: retinaculum musculorum peroneorum inferius; d8: calcaneofibular ligament. The black dotted line is the calcaneocuboid joint.
The sural nerve is accompanied by a small saphenous vein, wound to the lateral heel below the lateral malleolus, runs parallel to the pelma of the foot, and at the front of the calcaneus, moves obliquely across the peroneus brevis tendon and the peroneus longus tendon to the dorsolateral foot to become the lateral dorsal cutaneous nerve of the foot (Fig. 2C). The sural nerve is a cutaneous nerve. When injured, it mainly causes numbness and paresthesia in the innervated area of the nerve, which can be manifested as numbness in the posterolateral area of the calf, the lateral ankle area, the dorsolateral area of the foot, and the skin of the fourth and fifth toes. The fibular nerve is divided into two-to-three lateral cutaneous nerves behind the lateral malleolus, run downward perpendicular to the foot, and are distributed in the lateral skin of the heel. The proximal part of the sural nerve and the small saphenous vein are included in the flap located proximal to the incision, and the distal part is located in the flap of the distal end of the incision. The peroneus brevis tendon runs obliquely forward and down the lateral side of the calcaneus, from the back upward and is attached to the lateral calcaneal wall by the inferior peroneal retinaculum (Fig. 2D). The anterior tubercle of the calcaneus and calcaneocuboid joint is located above the front of the peroneal tendon. The peroneal tendon should be pulled down to expose the calcaneocuboid joint and the base of the sinus tarsus. The subtalar articular surface can be clearly exposed through the tarsal sinus, and a Kirschner wire (K-wire) can be inserted to poke the collapsed articular surface through this gap.
Surgical technique
The patients were positioned on the uninjured side with the ankle joint in a neutral position. Surgical pads were folded into squares and placed under the medial malleolus. The heel was slightly inverted in the air. The procedure was performed under a femoral tourniquet. (1) The skin and subcutaneous tissue were cut according to the hook curvy incision line, and the bleeding was carefully stopped (ligation and hemostasis; electric knife used with caution). The peroneal nerve was exposed on the superficial layer of the peroneal tendon, distal to the incision, and was freed and protected (Fig. 3A). (2) At the proximal side of the incision, a cut was made vertically to the periosteum without separation from deep tissue. The lateral calcaneal cutaneous nerve was severed. The lateral calcaneal artery was ligated for hemostasis. A separation was made along the periosteal surface to the malleolar tip, and the calcaneofibular ligament was cut to expose the subtalar articular surface. A separation was made along the surface of the periosteum in the middle of the incision through the deep layer of the peroneus brevis tendon and peroneus longus tendon. An attempt was made to free and protect the peroneus tendon sheath as much as possible to expose the tarsal sinus. A separation was made above the peroneus brevis tendon distal to the incision. The stop point of the extensor digitorum brevis was separated to expose the sinus tarsus, the anterior tubercle of the calcaneus, the calcaneocuboid joint, and the dorsal calcaneocuboid ligament. The proximal peroneus longus tendon was punctured with one-to-two 1.5 K-wires to the external malleolus, the flap was straightened, and the needle was slightly bent to the proximal end. Attention was paid not to squeeze the flap. A 1.5 K-wire was inserted into the talus neck through the front of the peroneus brevis tendon. The flap was straightened and bent medially. As this was necessary, the deep flap was slightly stripped on the surface of the peroneal tendon to reduce flap tension. (3) A large surgical towel was placed under the inner malleolus, and the calcaneus bone was slightly inverted. Slight poking at the subtalar joint with a 3.5 K-wire revealed the posterior articular surface of the calcaneus, and the collapsed posterior articular surface was restored through the sinus tarsal poking using the K-wire for temporary fixation (Figs. 3B and 4). A 3.5 K-wire was placed vertically into the calcaneal tuberosity, which was pulled down slightly to reset. The operator squeezed the calcaneal tuberosity with both hands and turned a K-wire to correct the calcaneus varus. After restoring the joint line of the calcaneal tuberosity, temporary fixation was applied from the calcaneal tuberosity through the posterior articular surface using a K-wire (Fig. 3C). After reduction, one-to-two 2.0 K-wires were temporarily fixed through the calcaneal tubercle to the anterior tubercle of the calcaneus. The calcaneal side and axial radiograph were taken using a C-arm perspective and replaced with the corresponding steel plate/screw fixation (Fig. 3D). (4) The mild valgus position of the heel was maintained, and a negative pressure drainage tube connected with negative pressure drainage was put in place. Subcutaneous intermittent suturing was performed to reduce the incision tension. Loose vertical mattress-type sutures were used for the incision. Soft gauze compressed the lateral wall of the calcaneus.
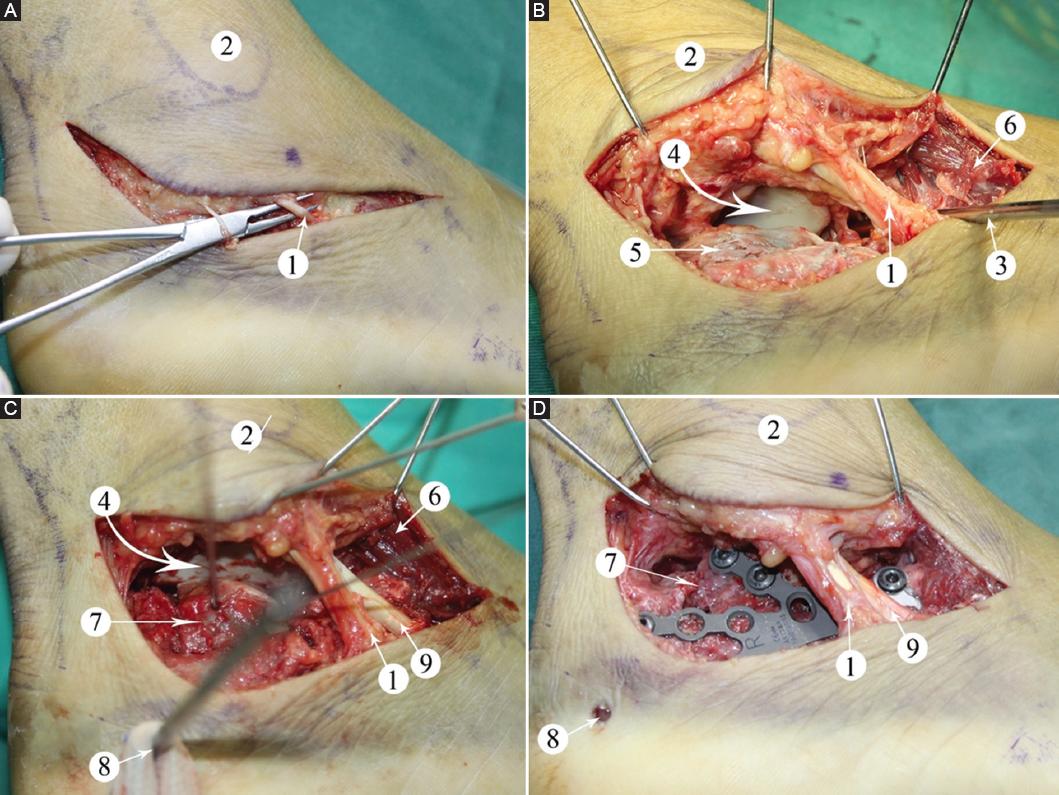
Figure 3 A: the incision and sural nerve. B: contactless traction of the Kirschner wire revealed the subtalar joint and the lateral wall of the calcaneus, and the Kirschner wire poke the collapsed articular surface. C: reduce the articular surface, and temporarily fix with the Kirschner wire. D: replace with plate fixation and remove temporary Kirschner wire. 1: sural nerve; 2: lateral malleolus; 3: Kirschner wire poking articular surface; 4: subtalar articular surface; 5: lateral wall of calcaneus; 6: extensor digitorum brevis; 7: reduction of the collapsed fracture block; 8: Kirschner wire for traction of calcaneal tubercle; 9: tendon of peroneus brevis.
Post-operative management
We evaluated the peroneal function within 24 h after the patient’s surgery, and the injury mainly caused innervation numbness and paresthesia. On the day after surgery, patients can be instructed to perform back extension, plantar flexion, and straight leg elevation exercises under non-weight-bearing ankle joint conditions. Low-molecular-weight heparin calcium anticoagulant therapy was provided after surgery until discharge. Patients were encouraged to carry partial weight on crutches at 4 weeks after surgery and were allowed to carry full weight when signs of bone healing were observed on re-examination X-rays at 6-10 weeks after surgery. The Bohler and Gissane angles were measured by X-ray 6 months after surgery. All patients were followed up for 2 years to assess their recovery.
Results
The modified tarsal sinus incision adequately exposed the posterior facet, the lateral wall of the calcaneus, and the calcaneocuboid joint. A traction valgus of calcaneal tuberosity can correct varus deformity. With the talus articular surface as a reference, the inferior talus’ articular surface fracture block was restored through tarsal sinus poking and temporarily fixed with a K-wire (Fig. 4). The articular plane was reduced to squeeze the lateral wall of the calcaneus. Titanium bone plates of appropriate type were selected, trimmed, and shaped according to fracture morphology and then inserted into the lateral calcaneal bone after subperiosteal dissection. After the percutaneous insertion of the guide by the template positioning method, drilling holes and screws were inserted to fix the plate. All 25 cases were followed up for an average of 18.7 (12-24) months. Bone healing was achieved in all patients at 12-month follow-up. The skin incision healed well in all cases without necrosis, infection, or sural nerve damage (Fig. 4). The fracture had healed in all cases after an average period of 8 weeks (6-10 weeks). Due to the different elastic modulus and compositional structure of metal and bone, the stress shielding effect would occur, which could lead to the easy recurrence of fractures around the fixed object. Accordingly, the plate-screw internal fixers were removed in 12 patients through the original incision 1-3 years after surgery, and all of the incisions had healed well.
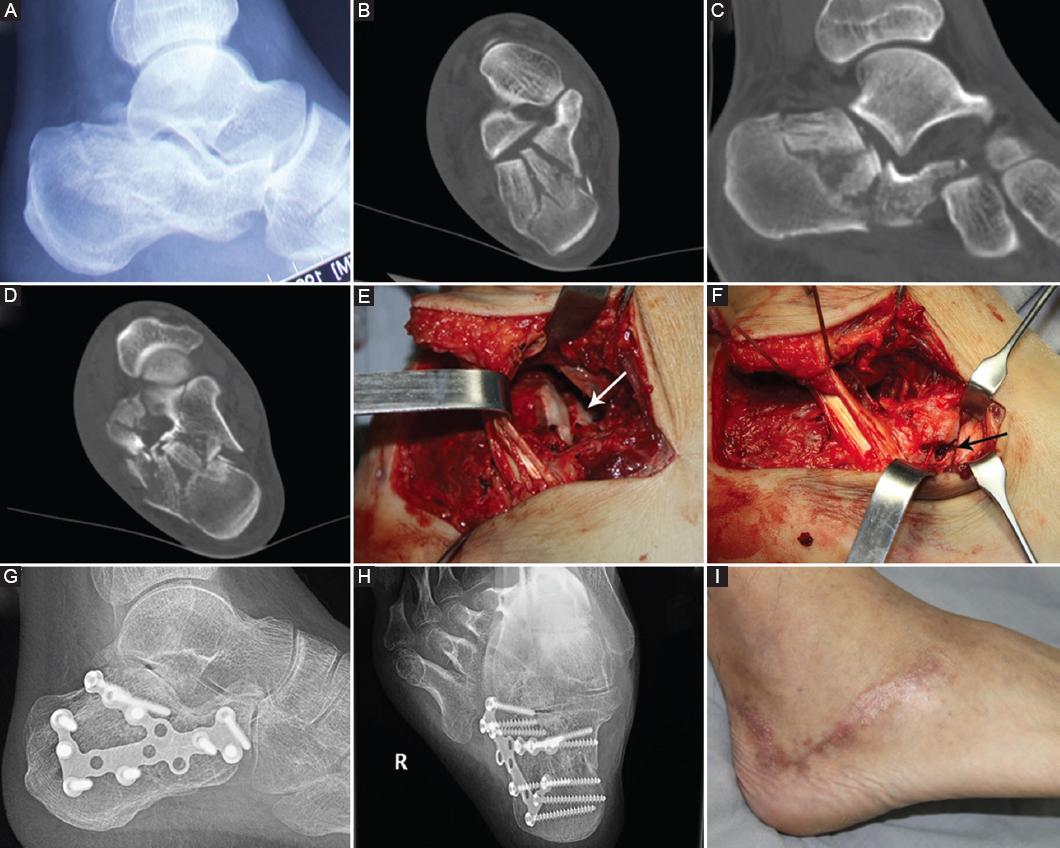
Figure 4 A: the lateral view of pre-operative radiographs. B-D: the images of the CT scan, Sanders type IIIBC. E: the fracture line of the posterior facet of calcaneus (white arrow). F: the fracture line involved the calcaneocuboid joint (black arrow). G and H: the lateral view and axial view of the post-operative radiographs. I: the healed lateral hook curvy incision.
According to the AOFAS anklehindfoot score, there were 20 excellent (80%), 2 good (8%), 2 fair (8%), and 1 poor patient (4%) outcomes. The 22 excellent and good cases were rated as satisfactory (88%); the three poor and fair cases were rated as unsatisfactory (12%). Pain at the lateral aspect of the heel was the main complaint of the majority of patients, particularly after long walks and heavy work. Six patients complained of feeling sore and uncomfortable in rainy weather; 12 patients (48%) returned to daily activities but could not bear heavy work; 3 cases (12%) felt mild pain when the surgical area was cold. A slight change in posture was observed in one patient (4%) with a bilateral calcaneal fracture. No pain developed related to irritation by the internal plate and screws. No cases of subluxation of peroneal tendons could be detected on follow-up. The one poor case (4%) was a patient with bilateral calcaneal fractures, Sanders IV right and Sanders IIAB left type, with poor post-operative recovery. When walking 100 m, the patient experienced unbearable pain, and foot movement was limited. This patient was found to have hyperplasia of the adjacent joints on X-ray 6 months after surgery. The average pre-operative Bohler’s angle was 6.8 ± 8.9°, and the average angle at follow-up was 33.6 ± 5.7°. The average pre-operative Gissane angle was 89.2 ± 20.0°, and the average angle at follow-up was 115.5 ± 5.5°.
Discussion
Calcaneal fractures are the most common tarsal fractures. Due to their irregular morphological structure and complex biomechanical functions, calcaneal fractures are considered one of the most challenging fractures, particularly displaced intra-articular calcaneal fractures. Restoring the shape of the articular surface, axis, and length and width of the calcaneus is essential for the recovery of the weight-bearing and walking abilities of the foot. In a randomized controlled trial, Buckley et al. found that patients with displaced intra-articular calcaneal fractures who did not receive worker compensation and underwent surgery had significantly higher satisfaction scores compared to non-surgical patients. The key to surgical treatment of displaced intra-articular calcaneal fractures is to fully expose intra-articular fractures to facilitate anatomical reduction and internal fixation. Open reduction and internal fixation through an extended lateral L-shaped approach have been considered the standard treatment15. However, the L-shaped incision was made from 3.5 cm below the lateral ankle along the plantar skin junction to the base of the 5th metatarsal bone with this surgical approach, giving rise to disadvantages such as a large dissection range, difficulty exposing the subtalar and calcaneocuboid joint surface, and a high learning curve.
Because the peroneal tendon travels obliquely through the lateral wall of the distal calcaneus, the pulling tendon to the dorsal side indirectly leads to the calcaneus valgus, which is not conducive to the exposure and reduction of the subtalar articular surface. The incidence of complications, such as post-operative incision infection, osteomyelitis, skin margin necrosis, plate exposure, and sural nerve injury is thus high, and the occurrence of complications is inversely correlated with the experience of the surgeon16.
With the continued development of minimally invasive and rapid rehabilitation concepts, the treatment of calcaneal fractures using a tarsal sinus incision has gradually been recognized in recent years. Some studies found that the incidence of soft-tissue necrosis, infection, and other complications after tarsal sinus incisions had been reduced to some extent5,13. However, this method is only suitable for less displaced intra-articular calcaneal fractures, such as Sanders II and IIIAB fracture types17. In addition, this incision has limited exposure to the posterior articular surface and a high learning curve, which limits its clinical application15.
The transverse arm of the lateral enlarged L-shaped incision is located between the blood supply area of the lateral and the plantar angiosomes, enabling the raised skin margin to obtain a sufficient blood supply from the feeding angiosome. Anatomical studies showed the presence of a rich blood supply in the lateral calcaneal region, and its feeding arteries include the lateral calcaneal artery, sinus tarsus artery, and lateral tarsal artery. These arteries have traffic branches that connect to vascular networks. The skin and subcutaneous soft tissue have an extensive vascular network. The lateral region of the heel is also connected to branches of the lateral plantar artery through traffic branches and the vascular network, enabling it to obtain a sufficient blood supply from the pelma area near the plantar region. This is the anatomical basis for the design of the lateral hook curvy incision of the calcaneus. The distal part of the incision can obtain sufficient blood supply from the terminal branches of the plantar and tarsal lateral artery to ensure the survival of the skin margin and significantly reduce the occurrence of complications related to the incision.
Compared with the lateral enlarged L-shaped incision from the metatarsal side of the calcaneus to the proximal end, the lateral hook curvy incision from the midline to the lateral side of the calcaneus is more likely to expose the subtalar joint surface, and the scope of the dissection is small. The hook curvy incision is oblique across the peroneal tendon, and the sinus tarsus and calcaneocuboid joint are exposed above the peroneal tendon, which is more conducive to the reduction and fixation of the fracture when the calcaneocuboid joint is involved. After clearing the tarsal sinus, the collapsed subtalar articular surface can be exposed. With the anterior calcaneus nodule as the fulcrum, a K-wire can be used to poke the collapsed joint surface. At the same time, through the lateral wall extrusion, it is easy to achieve an anatomical reduction of the inferior joint surface and restore the height of the calcaneal bone and the Bohler and the Gissane angles while reducing the dissection of the calcaneal fracture block. The proximal end of the incision may expose the upper edge of the calcaneal tuberosity, facilitating the reduction of the displaced calcaneal tuberosity.
Because the posterior articular surface of the calcaneus is difficult to reveal, and the soft-tissue blood supply of the lateral calcaneus is weak, the selection of appropriate surgical methods is very important for the treatment of calcaneus fractures. The lateral calcaneal L-shape incision is commonly used for the surgical treatment of calcaneal fractures involving the posterior articular surface, as it provides a wide surgical field of view and is firmly fixed with a plate that applies an overall compression force to the calcaneal bone, thereby restoring calcaneal width and preventing varus and valgus deformities. However, it was reported in the literature that lateral calcaneal L-shaped incision is prone to damaging the lateral calcaneal artery, and the incidence of post-operative soft-tissue necrosis, incision split, exposed plate, and infection is high18. In addition, both proximal and distal L-shaped incisions pose a risk of damage to the sural nerve. Therefore, many studies have focused on minimally invasive surgery for calcaneal fractures to minimize soft-tissue damage. The standard tarsal sinus incision is a longitudinal straight incision from the tip of the lateral ankle and extends to the base of the fourth metatarsal bone. As one of the minimally invasive techniques widely used in clinical practice, this approach can directly observe the posterior articular surface, making post-operative incisor-related complications less likely to occur. Li treated 53 cases of calcaneal fracture with incision reduction and internal fixation of the tarsal sinus, and the incidence of post-operative sural nerve injury was 9.6%19. The standard tarsal sinus incision is made below the anterior lateral malleolus, exposing the articular surface above the short and long peroneal tendons, where pulling the tendons downward may cause traction injury to the local sural nerve. Scholars conducted anatomical studies on the distribution of the sural nerve in 110 Korean carcasses, and the results showed that 58.8% of the carcasses had isolated a branch of the medial cutaneous nerve of the dorsal foot extending to the sural nerve within the standard tarsal sinus incision20. Therefore, a standard tarsal sinus incision may not be able to completely avoid sural nerve injury. A modified tarsal sinus incision can provide sufficient anatomical exposure to complete the reduction and fixation of calcaneal fractures. If it is necessary to extend back to the anterior process of the calcaneus, it will be easier to do so while protecting the long and short peroneal tendons, sural nerve, and accompanying blood vessels. The standard tarsal sinus incision makes it difficult to restore calcaneal width due to the limited exposure of the subtalar articular surface. A modified tarsal sinus incision can be used to reduce the fracture and fix the calcaneal fissure with a shapeable anatomical titanium plate. The location of the screw hole is determined percutaneously using the mold positioning method, after which the locking sleeve is placed. This avoids soft-tissue injury and reduces the possibility of injury to the lateral cutaneous nerve of the foot and subsequently obtains better biomechanical strength.
This study has the following limitations: the included sample size is small, and future studies with larger samples and multiple centers are needed to prove the efficacy of the presented approach. We did not report the effect of injury mechanisms and smoking history on surgical outcomes, which will serve as a limitation of this study and is expected to be explained in future studies. In addition, the researchers did not perform gait or plantar pressure distribution analyses; as such, it is uncertain whether there are significant abnormalities in post-operative gait patterns. Finally, this study did not compare the modified tarsal sinus incision with other surgical methods, and it is anticipated that future studies will be compared by statistical methods to highlight the advantages of the modified tarsal sinus incision.
Conclusion
Despite the limitations of the current study, the modified tarsal sinus incision has shown to be one of the safe methods for the treatment of displaced intra-articular calcaneal fractures. The lateral hook curvy incision can fully expose the subtalar articular surface and the calcaneocuboid joint and avoid ineffective exposure and negative traction reduction, which is conducive to the reduction and healing of the fracture.
Authors’ contributions
Conception and design of the work: Fu CS and Wei BF; Data collection: Pei HJ, Xue CY, Zhou JJ, and Zhong GD; Supervision: Fu CS and Wei BF; Analysis and interpretation of the data: Fu CS, Wei BF, Pei HJ, Xue CY, Zhou JJ, and Zhong GD; Statistical analysis: Fu CS, Wei BF, Pei HJ, and Zhong GD; Drafting the manuscript: Fu CS and Wei BF; Critical revision of the manuscript: all authors; Approval of the final manuscript: all authors.

