











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The global increase in sports and recreational activities has resulted in a rise in the number of anterior cruciate ligament (ACL) injuries. ACL injuries are a significant problem, particularly because they occur more frequently in young and working-age individuals1.
In Vojvodina, a region in the Republic of Serbia with a population of around two million, there are approximately 400 ACL reconstructions performed each year2,3. Although ACL reconstruction is considered a minimally invasive and safe procedure with minimal blood loss, even small amounts of bleeding can have negative effects on the knee joint structures4. The most common complications associated with ACL reconstruction are hemarthrosis, movement deficits, and infections5. Hemarthrosis causes post-operative pain, knee swelling, and a loss of knee joint range of motion, which can lead to limited mobility and poor functional outcomes6. In addition, hemarthrosis can be toxic to the articular cartilage and increase the risk of infection5. Slow post-operative recovery and prolonged rehabilitation can lead to increased morbidity, poor short-term and medium-term results, and higher costs for both individuals and the health-care system4,6.
Several studies have been conducted to reduce the risk of post-operative hemarthrosis after ACL reconstruction. These studies examined the effects of intravenous (IV) tranexamic acid (TXA) which requires careful consideration of the patient´s health condition and constant monitoring by the anesthesiologist and surgeon. Although previous research has shown encouraging results, there are inconsistent opinions among authors about the dosage regimen7-10. Due to the complexities of IV administration, there have been studies on the clinical benefits of intra-articular (IA) administration of TXA during ACL reconstruction. However, there is still no unified opinion among researchers for its routine application10-12.
Our study aims to evaluate the effect of IA administration of TXA after ACL reconstruction on post-operative bleeding, frequency of complications, occurrence of hemarthrosis, and pain intensity during six post-operative weeks.
Methods
The clinical research included 124 patients with a diagnosis of an ACL rupture and an indication for operative treatment. The study included patients who were 18 years or older and underwent arthroscopically assisted ACL reconstruction for the 1st time. Exclusion criteria used in the study included: A history of previous surgery on the same knee joint, kidney dysfunction, coagulation parameters showing pathological values, thrombophilia, treatment with drugs interfering with coagulation or TXA clearance, and history of previous allergic reaction to TXA (Fig. 1. Flowchart of case selection). Knee ACL reconstruction was performed according to the appropriate surgical protocol (modified clancy technique) for all patients. After the ACL reconstruction is completed, and after checking its isometry and stability in the knee joint, a drainage drain with a graduated vacuum bottle (redon-vacuum aspirator safe 500 mL OP-system) is placed, to monitor the amount of blood loss. A pneumatic surgical tourniquet was used routinely in all patients. All operations were performed by the same surgical team led by the same orthopedic surgeon, and the duration of the operation was recorded in the protocol.
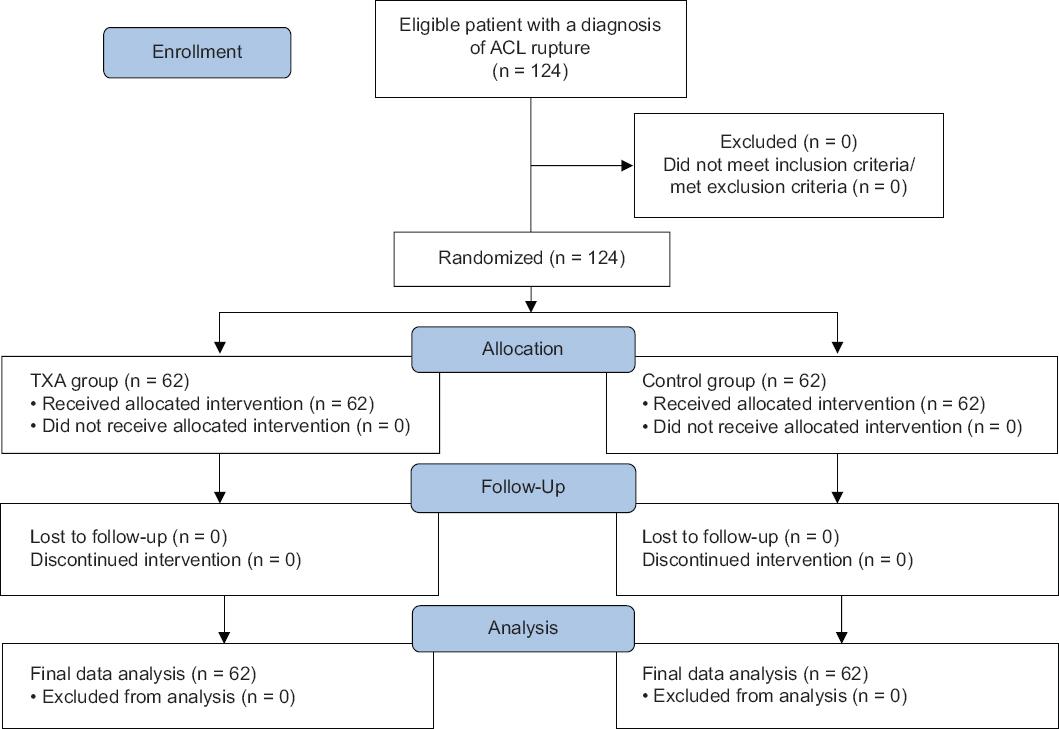
Figure 1 Consolidated standards of reporting trials flow diagram. ACL: anterior cruciate ligament; TXA: tranexamic acid.
For this research, we designed a randomizer to select and categorize our research sample with complete objectivity. On the day of surgery, we decisively divided the participants into two groups: The TXA group and the control group. Allocation was performed by computer-generated randomization by a non-involved contributor, leaving no room for any potential bias in the selection process. The surgeon, anesthetist, and patients were blinded regarding the use of TXA. Immediately before releasing the pneumatic surgical tourniquet, a 20 mL solution of TXA (5 mg/mL) was applied IA to the examined group of patients, while the patients in the control group were treated in the same way with an equivalent amount of sterile solution (normal saline). The drain was clamped for 30 min after the operation was completed, and then it was opened. On the 1st day after surgery, the patients drain was removed. The volume of blood drained in the graduated vacuum bottle was recorded in their medical records. During the immediate pre-operative preparation of the patient, 30 min immediately before the procedure, antibiotic protection was applied. During the post-operative period, the analgesia regimen included IV administration of a non-steroidal anti-inflammatory drug, according to the standard protocol of the clinic and the manufacturer´s recommendation.
Our research uses a Visual Analog Scale (VAS) to measure pain intensity. The VAS is a widely used subjective measurement scale in clinical practice, research studies, and clinical trials to assess pain intensity in a variety of settings, including acute and chronic pain conditions, post-operative pain, cancer pain, and more. Individuals can express their pain intensity by marking a point along a continuous line from 0 to 10, with 0 representing no pain and 10 representing the worst possible pain. During the post-operative phase, patients were requested to assess their pain intensity using a VAS at different time intervals, including 3, 6, 12, and 24 h, and for the following 7 days. The patients were followed up to 6 weeks after surgery, during which the presence of swelling, degree of hemarthrosis, and hematoma were evaluated. From the 1st post-operative day, the patients were put on an established protocol of early rehabilitation and performed exercises involving passive bending of the operated knee joint with the aid of a device for continuous passive mobilization (Kinetic-device) during their hospital stay. After 2 weeks of surgery, partial support was allowed on the operated limb, and full support was allowed after 6 weeks. All patients were put through the same rehabilitation program, which included a set of kinetic exercises to strengthen and restore the strength of the muscles of the front and back of the upper leg, immediately after the end of anesthesia. The duration of hospitalization was the same for all patients in both groups, and all patients completed the study.
The ethics and investigation committee of our institution approved the study design. All patients provided written informed consent.
Statistics
The IBM Statistical Package for the Social Sciences (SPSS) Statistics 21.0 package was used for data analysis. Numerical characteristics were measured using mean values and measures of variability, whereas attributive characteristics were measured using frequencies and percentages. The χ² test was used to evaluate differences in frequency distribution for attributive features. To compare the average values of numerical features between two groups of data, the Student´s t-test was used for parametric data, while the Mann-Whitney test was used for non-parametric data. The analysis of variance (ANOVA) test was used for repeated measurements to compare the values of three or more dependent samples with a measurement scale. For values with an ordinal measurement scale, the Friedman two-way ANOVA was used. Further mutual comparison was done using the Wilcoxon test of equivalent pairs. To determine the sample size, a significance level of α = 0.05, a power of the test of 1-β = 0.80, and an effect size of d = 0.62 were used. The estimated significant difference between the average amount of drained blood in the TXA and control groups was 50 mL (standard deviation = 80 mL), which was used to define the size of the effect. Based on this data, the minimum sample size for the study and control groups was 40. Oversampling of patients in each group was done due to potential withdrawals and losses. All tests used are two-sided, and a significance level of p < 0.05 is considered statistically significant.
Results
Out of the 124 patients who took part in this study, 102 (82.3%) were male, and 22 (17.7%) were female. Their average age was 31.0 ± 8.1 years. All the patients who were randomized for the study were accounted for. In both groups, there was a proper distribution of gender with 51 men and 11 women. Both groups were similar in all variables (Age, body mass index, American Society of Anesthesiologists, and type of anesthesia), except for the duration of the surgical intervention. In the TXA group, operative procedures were on average shorter (TXA group 79.35 ± 20.56 vs. control group 86.94 ± 21.45, p = 0.047) (Table 1).
Table 1 Socio-demographic and perioperative data of patients
| Variables | Category | TXA group (n = 62) | Control group (n = 62) | p |
|---|---|---|---|---|
| Sex, n (%) | Male | 51 (82) | 51 (82) | > 0.05 |
| Female | 11 (18) | 11 (18) | ||
| Age, year | 29.37 ± 7.93 | 26.76 ± 7.93 | 0.069ns | |
| BMI, kg/m2 | 25.80 ± 3.48 | 24.68 ± 3.21 | 0.064ns | |
| ASA | I | 38 (61.3) | 46 (74.2) | 0.147ns |
| II | 24 (38.7) | 15 (24.2) | ||
| III | 0 (0) | 1 (1.6) | ||
| Type of anesthesia, n (%) | General | 27 (43.5) | 23 (37.1) | 0.667ns |
| Spinal | 34 (54.8) | 34 (54.8) | ||
| Combined | 1 (1.6) | 4 (6.5) | ||
| Femoral nerve bloc | 0 | 1 (1.6) | ||
| Operative time (min) | 79.35 ± 20.56 | 86.94 ± 21.45 | 0.047 |
ns: non-significance; BMI: body mass index; ASA: American Society of Anesthesiologists.
The data in table 2 illustrate the difference in the amount of blood drainage after ACL reconstruction and the occurrence of hemarthrosis relative to IA injection of TXA. The average amount of post-operative bleeding in the examined group was 71.29 ± 40.76 mL, while in the control group, it was 154.35 ± 81.45 mL. The difference in post-operative blood loss between the groups was statistically significant (p < 0.001). After comparing the control group and the tested group of patients, it was found that the patients in the tested group had significantly lower pain intensity scores 3 h (p = 0.030) and 12 h (p = 0.039) after surgery. There was no significant difference in pain intensity score between the two groups 6 h and 24 h after surgery (p = 0.092, p = 0.051) (Table 2). During the 6 weeks following surgery, there were no instances of DVT or infections within the observed groups. In the TXA group, we have two patients who had aspiration. During the 3rd post-operative week, one patient had hemarthrosis (40 mL), and after the sixth post-operative week, another patient had hemarthrosis (60 mL). In the control group, two patients experienced hemarthrosis in the 6th post-operative week. In both cases, 60 mL of blood was aspirated (Table 2).
Table 2 Early post-operative outcomes
| Variables | Category | TXA group (n = 62) | Control group (n = 62) | p |
|---|---|---|---|---|
| Post-operative bleeding (mL) | 71.29 ± 40.76 | 154.35 ± 81.45 | < 0.001 | |
| VAS score | 3 h | 3.98 ± 3.31 | 5.26 ± 3.15 | 0.030 |
| 6 h | 4.81 ± 2.91 | 5.65 ± 2.58 | 0.092ns | |
| 12 h | 4.71 ± 3.25 | 5.92 ± 3.22 | 0.039 | |
| 24 h | 3.73 ± 2.66 | 4.61 ± 2.36 | 0.051ns | |
| Post-operative week 1 | VAS | 0.53 ± 1.02 | 0.97 ± 0.97 | 0.018 |
| Hemarthrosis, n (mL) | - | - | - | |
| Post-operative week 3 | VAS | 0.0 ± 0.0 | 0.18 ± 0.39 | < 0.001 |
| Hemarthrosis, n (mL) | 1 (40 mL) | - | - | |
| Post-operative week 6 | VAS | 0.0 ± 0.0 | 0.05 ± 0.22 | 0.073 |
| Hemarthrosis, n (mL) | 1 (60 mL) | 2 (60/60 mL) | - |
ns: non-significance; VAS: Visual Analog Scale.
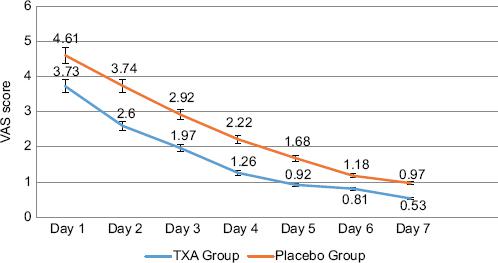
A comparison was made between the group that received TXA and the control group. The study found a significant difference in the intensity of pain experienced by the two groups on the 2nd day after surgery (p = 0.003), 3rd day (p = 0.003), 4th day (p < 0.001), 5th day (p = 0.001), and on the 7th day (p < 0.001). No significant difference in pain intensity was found between the two groups on the 1st day after surgery (p = 0.051) and the 6th day after surgery (p = 0.069) (Fig. 2).
Discussion
Our research found that the IA of TXA effectively reduces bleeding and pain following ACL reconstruction surgery, without complications such as DVT or infections.
Chiang et al. also reported similar findings in their research. They confirmed that IA administration of 10 mL of TXA (100 mg/mL) significantly reduced the amount of post-operative bleeding in the drain10. The research conducted by Karaaslan et al. provides compelling evidence that the administration of TXA can have a beneficial impact on both the early post-operative period and functional outcomes7. The results of their research indicate reduced post-operative drainage after IV application (TXA group 60 mL; Control group 150 mL), reduced post-operative hemarthrosis, and reduced need for knee aspiration7. This reinforces the importance of considering TXA as a treatment option in relevant cases. Reduced post-operative bleeding was also reported in the study by Felli et al.6 (TXA group 59.3 ± 29.5; control group 133.3 ± 56.1), but also in Pande and Bhaskarwar research8, which reports positive outcomes of TXA application, even though no drain was placed. The placement of the drain is still a topic of dispute for many authors. While some authors place a drain routinely, others associate it with the onset of infection13. IA drainage was inserted in our study, to monitor blood loss more precisely. During the 6th week of follow-up, we did not have any recorded complications in any group of patients, which we could relate to the placement of the drain.
Contrary to these results, Lee et al.11 found no significant difference in post-operative bleeding after IA application of 30 mg/mL TXA (control group 558 ± 236 [136-1088 mL]; TXA group 467 ± 242 [179-1127 mL]). However, they did not place a drain, so the estimated blood loss was controlled by the indirect method, which is also stated as a limitation of their study.
According to the research by Valkering et al.14, the first two post-operative days after the reconstruction of the ACL are the most painful, which was also confirmed by our research, whereas the TXA group had lower VAS score values. We noted that respondents in the TXA group showed a lower pain score at the third and twelfth post-operative hour, which can be related to the effect of an early IA injection of TXA, which is in accordance with the available literature15. During the 6th h and the first 24 h of the post-operative course, no significant difference was found between groups, although the pain intensity scores were lower in the test group at these times, as well. Moreover, a significant difference in pain intensity was observed between the test groups, on every subsequent day, except for the 6th day when the difference in pain intensity was in favor of the TXA group, although small. In our research, the assessment of pain intensity confirms a significant difference based on pain intensity on the 1st and 3rd week after surgery, but on the 6th week, no significant difference in pain intensity was found between the groups. In contrast to our research, Chiang et al.10 monitored the VAS scale score 2 times: on the 3rd day and the 4th week postoperatively, documenting a significantly lower intensity of pain on the 3rd day, while in the 4th week, they reported minimal differences in the VAS score between the groups10. Ma et al.12 reported a lower VAS scale in 1st and 2 weeks, but there was no reported difference in the VAS scale in 4th week between groups. Contrary to these studies, Lee et al.11 report no significant differences in pain intensity between groups, at all. Comparison of the VAS scale among the available studies should be viewed with a dose of caution, given that different anesthesia protocols, analgesia, and surgical techniques were used.
In the case of hemarthrosis, the patient usually needs aspiration (arthrocentesis). This is a procedure that causes discomfort to the patient and a potential cause of infection. Unlike the study by Chiang et al.10 who did not report the occurrence of hemarthrosis and Lee et al.11 who did not observe a statistically significant difference between the groups regarding the occurrence of hemarthrosis, in our study patients from both groups required knee aspiration at week 3 (n = 1 TXA group), that is, in the 6th week (n = 1 TXA group; n = 2 control group). According to the available data, three authors report the need for aspiration in patients who received TXA IV. Karaaslan et al.7 state the need for aspiration in 23 patients (four TXA group and 19 control group), Pande and Bhaskarwar8 in a total of 10 patients (three TXA group and seven control group), while Fried et al.9 performed aspiration in 49 patients (23 TXA group and 26 control group).
In conclusion, the meta-analysis conducted by Johns et al.15, it was found that IV use of TXA is preferable over IA administration. Their analysis included only one study where TXA was administered IA15. Considering previous research, the conclusions of two meta-analyses suggest that the use of TXA in ACL reconstruction reduces drainage output and knee swelling, pain intensity, incidence of hemarthrosis, and the need for aspiration in the post-operative period. Given that there were no reported complications, the use of TXA could be useful in arthroscopic surgery16,17.
In our study, it was proven that the bleeding in the knee joint was reduced, as well as the low intensity of pain during the entire monitoring period. Thus, IA administration of TXA could be considered a safe solution to reduce post-operative bleeding and pain after ACL reconstruction. Due to the need for aspiration of the knee joint that occurred in both groups of patients in our study, additional research would be useful to confirm the late effect of IA TXA administration on the occurrence of hemarthrosis. The studies available so far differed in the way and doses of TXA applied, not only in ACL reconstruction but also in orthopedic prosthetic surgery. Studies comparing the same route of administration at different doses in the same study group may be of great importance18. It would certainly be important to conduct extensive research on the assessment of the optimal dose and time of exposure of the knee joint structures to the effect of TXA, to take a common position on the IA application of TXA during ACL reconstruction.
Study limitations
Our study has some limitations that need to be addressed. Firstly, the sample we examined consisted of professional athletes whose previous physical fitness and self-discipline may differ from those who engage in sports only recreationally or not at all. This difference could have affected the extent of pain tolerance and changes in the VAS scale. In addition, we did not consider the difference in time between injury and surgery. Finally, due to the low representation of female subjects, we were unable to confirm with certainty whether IA injection of TXA has been linked to post-operative bleeding, VAS scale values, and the incidence of hemarthrosis in patients of both genders.
Conclusion
Based on our research, applying TXA in the joint effectively reduces post-operative bleeding in the first 24 h, minimizes hemarthrosis occurrence in the early period, and reduces pain intensity during the 1st week. The group of patients who underwent the IA application didnt experience any systemic side effects during the follow-up period. Although we have some knowledge regarding the benefits of using TXA in ACL reconstruction, we believe that more research is necessary to collect data on the relationship between TXA effectiveness and different methods of administration, dosage, duration of exposure, and the impact of TXA use on long-term functional outcomes.

