











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Electroconvulsive therapy (ECT), a medical treatment that´s been available since the 1930s, has been both hailed as a lifesaver and condemned as controversial in the field of psychiatry. Administered under intravenous sedation or general anesthesia, ECT works by inducing a generalized cerebral seizure with an electric current, an approach that has evolved considerably over the decades with refinements such as the introduction of muscle relaxants and advancements in anesthesia1. Despite its long history, ECT continues to polarize opinion; some experts regard it as the most effective psychiatric treatment and entirely safe, while others raise concerns about its efficacy and potential for causing brain damage2.
This complex intervention is not a one-size-fits-all remedy; its outcomes are influenced by various factors, including electrode placement, electrical stimulus dosage and waveform, and treatment frequency. ECT can be considered as the first-line treatment option in cases such as depressive stupor, severe psychomotor retardation, refusal to eat or drink, high risk of suicide, severe excitement, neuroleptic malignant syndrome, some systemic diseases, and psychiatric disorders of the perinatal period. In addition, treatment-resistant cases constitute the most common indication for ECT3.
Treatment resistance affects 20-60% of patients with psychiatric disorders and is associated with increased health-care burden and costs up to ten-fold higher relative to patients in general. Treatment resistance is recognized across a range of psychiatric disorders, including schizophrenia, major depressive disorder, and bipolar disorder. Guidelines highlight three core components required to establish the definition of treatment resistance seen across disorders; these are that the correct diagnosis has been made, that adequate treatment has been given, and that there has been inadequate response. However, there are still significant differences in details between the guides. In general, lack of adequate response despite adequate use of at least two drugs defines treatment resistance4.
The global suicide mortality rate amounts to 1.4% of all deaths worldwide. Most suicides are related to psychiatric disease, and almost all psychiatric disorders are correlated with increased suicide risk. A rough estimate is that suicide attempts are 10 times more likely than completed suicides, and suicide plans are 10 times more likely than attempts5. When viewed from this perspective, the devastation caused by suicide and the importance of its treatment can be seen better6,7.
As the utility of ECT continues to be a subject of clinical interest, particularly in its application for severe psychiatric disorders, this study is predicated on the hypothesis that distinct patient populations those with a history of suicide attempts and those who are treatment-resistant may exhibit differing responses to ECT in terms of clinical outcomes and treatment course8-10. We posit that the intensity and frequency of ECT sessions, as well as the duration of induced seizures, may correlate with the diagnostic category and severity of the psychiatric condition.
In this study, we aimed to evaluate how ECT affects treatment-resistant depression, bipolar and schizophrenic patient groups, and suicide attempt histories and to evaluate the relationship between treatment variables and patient outcomes.
Materials and methods
Design of the study
This research conducted a comparative retrospective analysis, centering on two groups of patients between January 2021 and March 2023. A total of 103 patients were included. Patients receiving ECT were divided into two groups based on their indications for undergoing ECT. Group 1 (n = 76) consisted of patients who received ECT due to suicidal attempts, and Group 2 (n = 27) consisted of patients who were resistant to pharmacotherapy. Both groups had undergone ECT at our institution. We compared age, gender, distribution of the diagnosis, neutrophil counts, lymphocyte counts, neutrophil-to-lymphocyte ratio (NLR), number of applied ECT, and total seizure time.
Inclusion criteria
Our study included patients over the age of 18 who had been diagnosed with bipolar disorder, schizophrenia, and depression according to DSM-5-TR diagnostic criteria. The study was single-centered, encompassing patients who presented to the psychiatric department of Çam and Sakura City Hospital and underwent inpatient treatment, including the administration of ECT.
Exclusion criteria
Patients were excluded if they had a history of neurological disorders, substance abuse within 6 months before ECT, or incomplete medical records. Those who received < 4 sessions of ECT were excluded from the study, assuming they still needed to complete treatment. Pregnant cases were excluded because we classified our cases according to indication, and pregnancy could create a different indication, such as reducing drug exposure. Furthermore, cases that could fall into both suicidality and treatment resistance groups were excluded.
ECT procedure
Patients in our study received bilateral ECT treatments twice to 5 times a week with Thymatron® DGxTM (Somatics, LLC). Doses for the first ECT sessions were calculated through the half-age rule. Efforts are being made to find an ECT dosing approach that minimizes the occurrence and intensity of neurocognitive deficits linked to the treatment while preserving its therapeutic advantages. In employing this method, individuals adjust the "percent energy dial" to half the patient´s chronological age or round it up to the nearest higher available setting11. Throughout the ECT series, doses were progressively increased to ensure seizure durations met or exceeded the 20-s minimum. Physiological parameters were continuously monitored using pulse oximetry, noninvasive blood pressure, electrocardiography, and electroencephalography. ECT was administered until the patient achieved full remission10.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Başakşehir Çam and Sakura Training and Research Hospital (Approval number: [2023-347]). Informed consent was waived due to the retrospective nature of the study.
Statistical analysis
Data were analyzed using the JAMOVI software, version 2.4. Continuous variables were expressed as means ± standard deviation and compared using the t-test or the Mann-Whitney U test, as appropriate. Categorical variables were compared using the X2 test or Fishers exact test. A p < 0.05 was considered statistically significant.
Results
The average age of patients in the suicide group was 33.4 ± 12.1 years, while the treatment resistance group averaged 35.8 ± 12.7 years; this age difference was not statistically significant (p = 0.374). Gender distribution among the groups showed that 63% (n = 48) of the suicide group were male compared to 74% (n = 20) in the treatment resistance group, which was not a significant difference (p = 0.304). The diagnostic composition between the groups revealed significant differences (p = 0.027). Within the suicide group, 17% (n = 13) were diagnosed with bipolar disorder, 63% (n = 48) with schizophrenia, and 19% (n = 15) with major depression. Conversely, the treatment resistance group had a higher proportion of bipolar disorder at 40% (n = 11), while schizophrenia and major depression were represented at 37% (n = 10) and 22% (n = 6), respectively (Fig. 1C). The mean neutrophil count was 5.9 ± 2.3 for the suicide group and 5.2 ± 2.2 for the treatment resistance group, which did not differ significantly (p = 0.202). Lymphocyte counts were also similar between the two groups (suicide: 2.3 ± 0.7; treatment resistance: 2.3 ± 0.9) (p = 0.763), as were the NLR measurements (suicide: 2.9 ± 2.2; treatment resistance: 2.7 ± 1.9; p = 0.674).
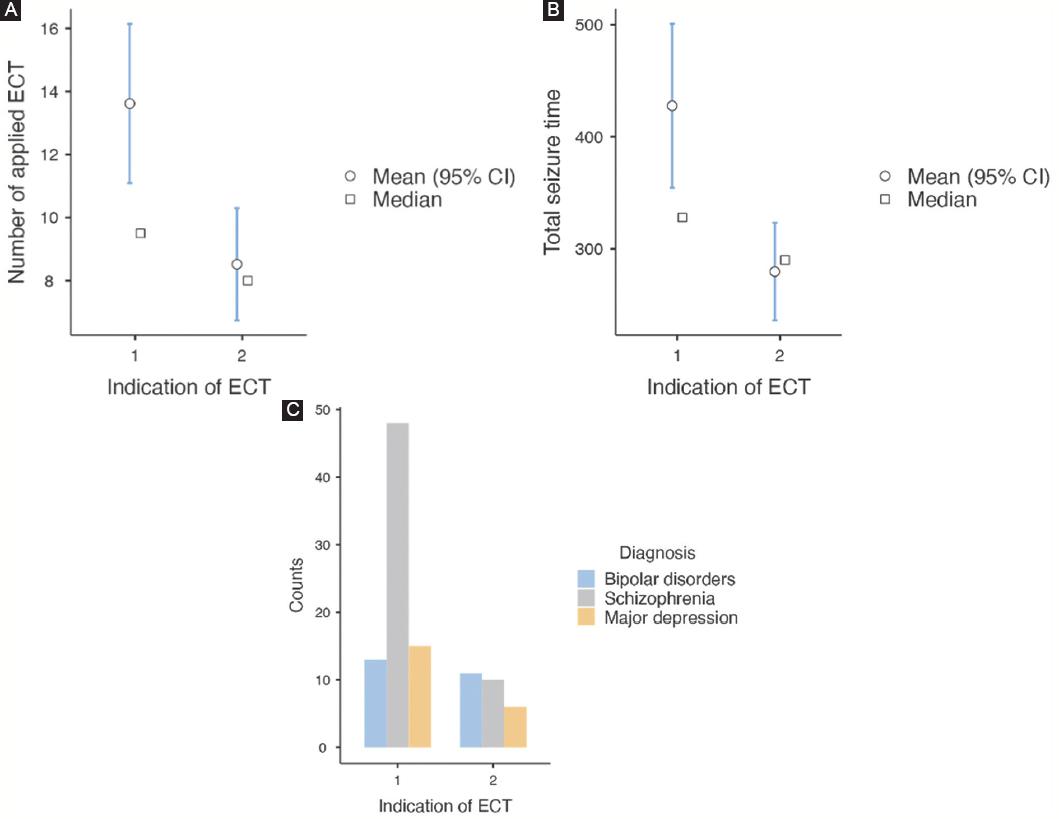
Figure 1 A: the number of applied electroconvulsive therapy. B: total seizure time. C: indication and diagnosis. Group 1 = suiside group; Group 2 = treatment resistant group.
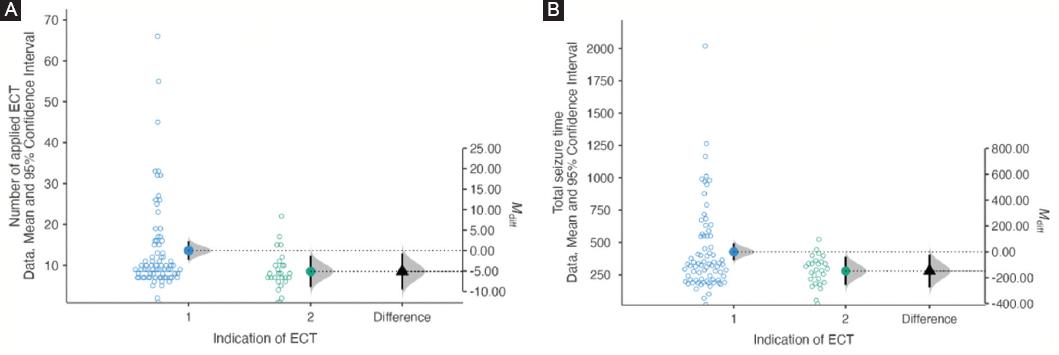
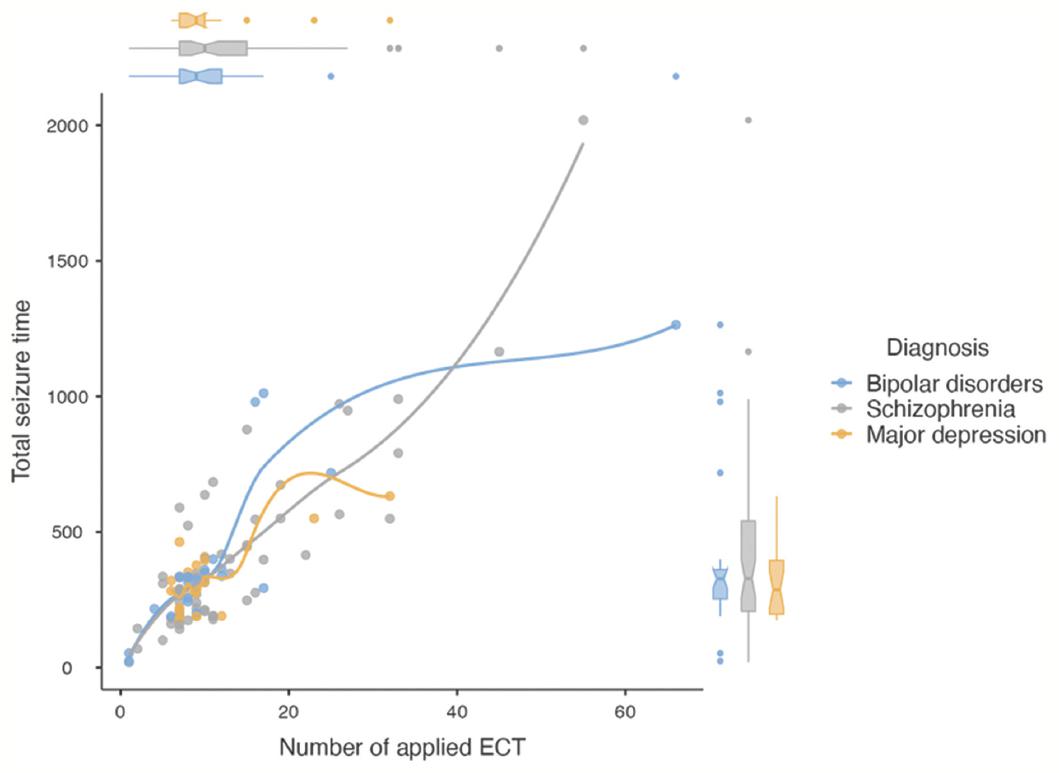
However, the number of ECT sessions applied varied significantly between groups, with the suicide group receiving a higher number of treatments (13.6 ± 11.2) compared to the treatment resistance group (8.5 ± 4.7) (p = 0.025) (Fig. 1A). In addition, the total seizure time was significantly longer in the suicide group (427 ± 325 s) than in the treatment resistance group (279 ± 115 s) (p = 0.023) (Table 1 and Fig. 1B). The differences of the number of applied ECT and total seizure times in terms of indications were shown in figure 2A and B. figure 3 illustrates the scatter plot of number of applied ECT, total seizure time, and diagnosis.
Table 1 Demographic and comparisons
| Variables | Suicide (n = 76) (%) | Treatment resistance (n = 27) (%) | p-value |
|---|---|---|---|
| Age | 33.4 ± 12.1 | 35.8 ± 12.7 | 0.374 |
| Gender (M) | 48 (63) | 20 (74) | 0.304 |
| Diagnosis | 0.027 | ||
| Bipolar disorder | 13 (17) | 11 (40) | |
| Schizophrenia | 48 (63) | 10 (37) | |
| Major depression | 15 (19) | 6 (22) | |
| Neutrophil | 5.9 ± 2.3 | 5.2 ± 2.2 | 0.202 |
| Lymphocyte | 2.3 ± 0.7 | 2.3 ± 0.9 | 0.763 |
| NLR | 2.9 ± 2.2 | 2.7 ± 1.9 | 0.674 |
| Number of applied ECT | 13.6 ± 11.2 | 8.5 ± 4.7 | 0.025 |
| Total seizure time (sec) | 427 ± 325 | 279 ± 115 | 0.023 |
*ECT: electroconvulsive treatment; NLR: neutrophil-to-lymphocyte ratio.
Discussion
This study provides an in-depth analysis of ECT as a treatment method for two specific groups: individuals with suicide risk and those showing resistance to pharmacological treatments. Our findings contribute to the nuanced understanding of ECTs clinical outcomes and demographic correlations, underpinning its application in psychiatric treatment strategies.
ECT maintains its essential place in the treatment of psychiatric patients, although stigmatization problems persist. Many large-scale studies reveal the characteristics of patients receiving ECT and the effectiveness of the treatment7,8,10. There are also studies comparing the effectiveness of ECT on a diagnostic basis and the prominent features in different groups7,8,12. However, there are a limited number of studies comparing ECT according to indications. In this respect, our study is one of the first steps in filling a significant gap.
The most common indication of 176 ECT treatments performed for 5 years in a hospital located in another province in Turkey was suicidality, followed by treatment resistance. The order of the indications is similar to our study13. However, in the study conducted by Tor et al. in Singapore, unlike our study, the indication for treatment resistance was significantly higher than suicidality8. The fact that all three studies were single-centered suggests that the different characteristics of the centers may affect the rates. Similar rates in two Turkey-based studies, our study and the study of Bolu et al., may indicate the relationship between diseases and sociocultural or genetic structure13.
Demographic analysis in our study revealed no significant age differences between the suicidal and treatment-resistant groups; this suggests that the therapeutic decision for ECT transcends the age factor in the context of these two conditions. Similarly, the gender distribution did not show a significant difference, implying that the decision for ECT application is primarily driven by clinical indications rather than gender. This is consistent with the non-discriminatory application of ECT across different demographic groups, reflecting its broad acceptability in psychiatric practice13.
Our study showed a significant difference in diagnoses in the suicidality and treatment resistance indication groups. While schizophrenia patients were predominant in the suicidality group (68%), there was a relatively balanced distribution in the treatment-resistance group. In the study of Tor et al., positive psychotic symptoms dominated the treatment resistance group, followed by mania, depression, and psychotic depression, respectively8. The different diagnostic distinctions make it difficult to compare the two studies. The limited number of people who received ECT due to the risk of suicide (n: 8) also does not allow comparison. It was interesting and surprising that the number of schizophrenia patients was higher than depression in the suicidality group. It points out the importance of assessment of suicide risk in addition to the positive and negative symptoms of schizophrenia.
Mean neutrophil-to-lymphocyte counts and NLR are essential biomarkers. Many studies have shown that it is increased in psychiatric conditions such as depression and schizophrenia or first-episode psychosis, and a smaller number of studies have shown that it is increased in bipolar disorder14-16. Studies are showing the relationship between NLR and the presence and severity of suicidal behavior17,18. High NLR rates are also associated with treatment-resistant depression and schizophrenia19. Our study detected no difference between the two groups regarding neutrophils, lymphocyte counts, and NLR before ECT. Since the NLR will be high in both suicidality and treatment resistance, it can be interpreted that the high NLR does not make a difference between the two groups. Furthermore, our results appear to be consistent with a large-scale study claiming that a high NLR rate is a transdiagnostic marker in psychiatric diseases20. However, our study´s need for a healthy control group limits our interpretations.
The significant difference in the number of ECT sessions and total seizure time between the groups is a critical finding. Patients with suicide risk received more ECT sessions and had longer total seizure durations, indicating a more intensive treatment course. According to the study of İzci et al.,21 in which patients diagnosed with major depression receiving ECT were grouped into suicidality and treatment resistance, similar to our study, no difference was found between the number and total duration of ECTs in these two groups. This result contradicts ours in the context of depression. Tor et al. in a study evaluating ECT indications according to diagnoses also classified them according to the actual reasons for ECT8. According to this study, ECT was applied to 55% of the participants (n: 386) due to lack of response to medical treatment and 1.2% (n: 8) due to a high risk of suicide. The average duration of ECT was found mainly in the treatment of positive psychotic symptoms, followed by catatonia, mania, psychotic depression, and depression. Although the study design does not allow comparison with our study, the significant difference in session durations in different indications is a finding that overlaps with our study. According to the Royal Australian and New Zealand guidelines, catatonia generally responds more quickly to ECT treatment than depression and treatment-resistant schizophrenia and mania22. Another study comparing the number of ECT sessions did not find a significant difference in the number of sessions between diagnoses23. The study shows that only people over 65 receive more ECT sessions. Another study conducted in Turkey did not find a significant difference in the number of sessions between different diagnoses24. However, these two studies differ from our study because they evaluate the indication diagnostically. The number of studies examining the effects of different indications on the number and duration of ECT is limited in the literature, and conflicting results indicate that more extensive studies are needed on this subject.
Furthermore, our research has important implications for the patient management pathway, including the need for robust post-ECT follow-up, particularly for those with severe psychiatric presentations. The necessity for a personalized approach to ECT, considering the individuals diagnostic profile and previous treatment responses, is underscored by the variation in treatment regimens observed.
However, this study is not without limitations. The retrospective design inherently carries the potential for selection and information bias. The exclusion of patients due to incomplete medical records may also have led to an underrepresentation of the true clinical picture. The sample size, particularly of the treatment-resistant group, is small, which may limit the statistical power to detect differences and may not fully represent the broader population undergoing ECT.
Conclusion
The study affirms the role of ECT as a valuable treatment option for both suicidal and treatment-resistant patients, with specific clinical and demographic profiles associated with each group. The findings call for a tailored approach to ECT administration, considering the patient´s diagnostic background and severity of presentation. Prospective, larger-scale studies are required to further elucidate the intricacies of ECT outcomes, optimally inform clinical protocols, and ensure the best possible patient care.

