











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Boerhaave’s syndrome or spontaneous esophageal perforation is an uncommon but potentially fatal condition, as it may lead to severe mediastinitis, sepsis, and consequently multiple organ failure1. It usually manifests in adult (40-60 years old)2 alcoholic male patients3. Its symptoms are usually non typical, while the Mackler triad with vomiting, chest pain, and subcutaneous emphysema is found in < 33% of the cases1,4. Treatment can be surgical or conservative5. We present the successful conservative treatment of Boerhaave’s syndrome in an 83-year-old female patient.
Case report
An 83-year-old female patient presented to the Emergency Department 15 h after the sudden onset of left-sided chest pain immediately after a vomiting attempt. She experienced shortness of breath, tachypnea, and difficulty swallowing. She was hemodynamically stable (blood pressure = 125/80 mmHg and heart rate = 89 pulses/min). Oxygen saturation was 92% and temperature 37.3°C. Physical examination of the abdomen was normal, bowel sounds were normal, whereas thoracic examination revealed decreased breath sounds in the lower left lobe and crepitus consistent with subcutaneous emphysema. Blood test results revealed slightly elevated white blood cells and C-reactive protein, while the rest biochemical exams and electrocardiogram were normal. She underwent a chest X-ray, which revealed pneumomediastinum and hydropneumothorax and subcutaneous emphysema of the left hemithorax.
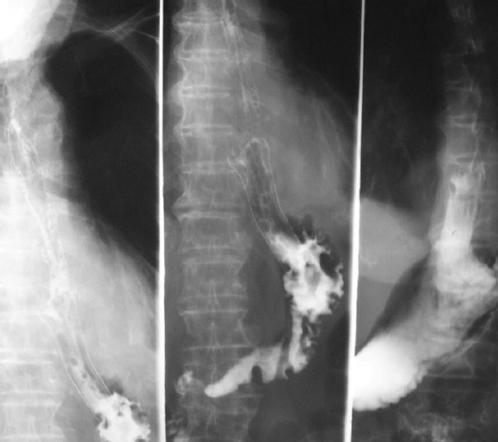
A chest tube was inserted under local anesthesia to drain the hydropneumothorax and the patient was submitted to a computed tomography (CT) scan of the chest and abdomen which also demonstrated the same findings of pneumomediastinum and hydropneumothorax and subcutaneous emphysema of the left hemithorax with no significant findings from the abdominal cavity (Fig. 1). A possible diagnosis of spontaneous esophageal rupture was considered which was confirmed with a gastrografin esophagography demonstrating a rupture in the left lower third of the esophagus (Fig. 2).

Figure 1 Gastrografin esophagography demonstrating a rupture in the left lower third of the esophagus and significant extravagation of gastrografin.
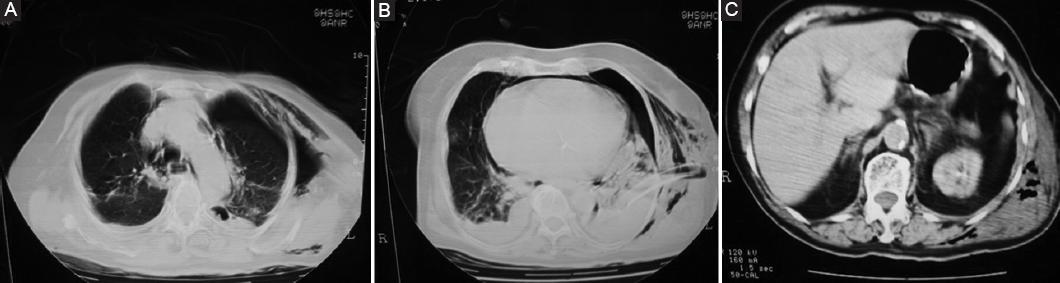
Figure 2 Thoracoabdominal computed tomography scan showing pneumothorax. A: pneumomediastinum and subcutaneous emphysema. B: hydropneumothorax, pneumomediastinum and subcutaneous emphysema. C: no significant findings from the abdomen except subcutaneous emphysema.
Based on patient’s age, comorbidities, American Society of Anesthesiologists physical status score of III, anticipated morbidity and mortality of a surgical repair and time since the onset of symptoms (24 h from the esophageal rupture after the definitive diagnosis) it was decided that the patient should be treated conservatively. Patient’s hemodynamic stability and lack signs and symptoms of sepsis were also taken into consideration. Thus, except of the closed thoracostomy with one drain, the patient was kept null per os, while intravenous fluids, broad-spectrum antibiotics, and total parenteral nutrition were administrated. The patient continued to be monitored with clinical examination as well as laboratory and imaging tests, which revealed gradual improvement of her condition. On the 13th day of hospitalization a gastrografin esophagography did not reveal any extravagation of gastrografin but demonstrated a stenosis of the distal esophagus (Fig. 3). As the next days, the patient was not able to eat and drink normally it was decided to place an intra-esophageal self-expanding stent which was successfully placed on the 30th day of hospitalization and feeding began without problems (Fig. 4). She was discharged 3 days later.

Discussion
Boerhaave’s syndrome or spontaneous esophageal perforation was first reported by Dr Hermann Boerhaave in 1724. It is an uncommon but potentially fatal condition, as it may lead to severe mediastinitis, sepsis and multiple organ failure1. It has a significant high mortality rate that ranges between 20% and 75%6 and approaches 100% in untreated cases7. Since delayed diagnosis and therefore treatment increases morbidity and mortality5 (delay of 12 h - 36% and delay of 24 h - 64%)3, the suspected cases should be identified and further investigated immediately.
Boerhaave’s syndrome is usually manifested in adult (40-60 years old)2 alcoholic male patients3. Our 83-year-old female patient is an exception. Its etiology is the increased intra-luminal pressure in the esophagus, which mainly happens during vomiting (>95% of cases), as was in our case. Other rare causes are asthma, seizures, and childbirth, which also increase the intra-abdominal pressure. Esophagus lacks serosal layer that acts protectively, making it prone to rupture2,8. The location of rupture is mainly in the left lower third of the esophagus7, as was in our patient.
Boerhaave’s syndrome is misdiagnosed frequently. The clinical presentation of the syndrome varies from lack of symptoms to hemodynamic instability2 and may mimic other cardiothoracic or upper gastrointestinal diseases such as peptic ulcer perforation, myocardial infarction and pneumonia that are more common. Its presenting symptoms (vomiting and epigastric pain) are usually non typical1, while the Mackler triad with vomiting, chest pain, and subcutaneous emphysema is found in < 33% of the cases4. In late presentation (24 h) odynophagia, subcutaneous emphysema and Hamman sign (a “mediastinal crunch”)9 can be found7. It has also been claimed that pain worsens with swallowing10 and it may be accompanied by dysphagia or fever4. Our patient experienced many of the typical symptoms.
The diagnostic tools for Boerhaave’s syndrome are chest X-ray, contrast esophagography, esophagoscopy, and thoracic CT scan1. More specifically, chest X-ray may reveal hydropneumothorax, pneumothorax, pneumomediastinum, pleural effusion, subcutaneous emphysema, or widened mediastinum2,5, while contrast esophagography may show contrast media extravasation11 and is considered to be the gold standard12. Esophagoscopy is as sensitive as esophagography, but it needs to be carefully performed. Finally, CT scan may show pneumothorax, pneumomediastinum, and pleural effusion1.
Treatment of Boerhaave’s syndrome remains controversial. Many authors argue that immediate surgery is necessary, whereas others support that if certain criteria such as early detection and limited to the mediastinum esophageal rupture, well drained cavity into the esophagus and limited patient symptoms without signs of sepsis and patient’s stability, or pleural loculus esophageal ruptures are met, conservative treatment should be chosen1. It is most commonly believed that surgery should be the treatment of choice with a 2-layer primary buttressed repair and drainage of the pleural cavity1,13. Other suggests that the choice of surgical or conservative treatment should be based on the site and extent of the rupture, the patient’s symptoms, signs, and radiographic findings5. Conservative treatment includes parenteral nutrition, broad-spectrum antibiotics coverage, thoracostomy, and percutaneous drainage of fluid collections and has been proved to be efficient1,3. A 92% survival rate has been reported using these measures3. Endoprostheses, endoscopic management, clipping, and gluing have been also suggested4. The use of esophageal stents and percutaneous thoracic drainage in the treatment of Boerhaave’s syndrome has not been well reported14,15. However, esophageal self-expanding stents have been used and encouraging results have been reported, such as in a 2010 report, in which 10/15 patients were successfully treated with stent16. Over time new stents with improved properties, such as easier removal, have been invented. For instance, the recently invented Polyflex stent is suitable for temporary placement in benign conditions, can be easily removed and causes minimal tissue hyperplasia. In a few cases stents have caused complications, such as fistulas and strictures15.
A complication of conservative treatment that has been seldom reported in the literature is esophageal stenosis17. Stenosis can be successfully treated with endoscopic placement of an esophageal self-expanding stent17. In our case, spontaneous esophageal perforation was successfully treated in an octogenarian with conservative management (intravenous fluids and parenteral nutrition, broad-spectrum antibiotics coverage, and drainage) and after patient stabilization an esophageal stent was placed to treat the stenosis that has developed.
In conclusion, although Boerhaave’s syndrome is a rare condition, doctors should be alerted to diagnose and treat it in time, so the patient could have increased chances of survival. Conservative treatment is an option for stable patients.

