











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Children with acute lymphoblastic leukemia (ALL) may present with musculoskeletal symptoms, including functional limitations, limping, and joint effusion.1 These symptoms are often described as intermittent, sudden, and migratory, which can lead to a misdiagnosis.2,3 Besides osseous pain, clinicians should also consider the possibility of septic arthritis and osteomyelitis in ALL patients.4Candida albicans is the species most frequently associated with fungal osteomyelitis; however, there has been a significant increase in non-albicans Candida infections.5 Despite being clearly associated with leukemia patients, bone involvement by fungal infections is rare.
We present a case of a 4-year-old girl with a history of medium-risk ALL in complete remission, who developed a chronic osteoarticular infection of the elbow due to Candida tropicalis during the second week of rest post-consolidation.
Case presentation
A 4-year-old female patient, diagnosed five months ago with medium-risk acute lymphoblastic leukemia type B with central nervous system involvement, was admitted to the emergency department of our center for a single subfebrile episode (37.5 oC) along with right elbow pain that had developed over the past 24 hours. She was in the second week of rest post-consolidation block of Argentine Group for the Treatment of Acute Leukemias (GATLA) 2010 pediatric protocol. It is important to mention that the patient had a porth-a-cat placed 1 month prior and was receiving antibiotic prophylaxis with Trimethoprim and Sulfamethoxazole 100 mg/day, three times per week.
At the time of admission, the patient was hemodynamically stable and febrile. She presented with right elbow pain and limited flexion-extension range of motion (90o-160o) without evidence of edema, erythema, or elevated local temperature. Initial laboratory tests revealed leukocytes at 5,600/mm³ (with neutrophils at 2,747/mm³), hematocrit at 27%, hemoglobin at 9.6 g/dl, platelets at 60,000/mm³, erythrocyte sedimentation rate at 9 mm, and C-reactive protein at 57 mg/l. Anteroposterior and lateral radiographs of the right elbow revealed a radiolucent image on the external aspect of the humeral metaphysis (Figure 1).

Figure 1: Anteroposterior and lateral radiographs of the right elbow show a radiolucent image in the medial region of the humeral trochlea.
The patient was admitted for further evaluation, and a magnetic resonance imaging (MRI) of the elbow was performed. The results showed joint effusion alongside an osteolytic lesion at the medial aspect of the humeral trochlea, as well as edema of the trapezius muscle (Figure 2). Urine, peripheral blood, and central venous catheter retro cultures were obtained and results negative. Despite negative initial cultures, surgical debridement was performed 24 hours after admission via a Kaplan lateral elbow approach, along with a needle bone biopsy for bacteriologic and histologic analysis. During capsulotomy, a significant amount of purulent fluid was observed and collected for analysis. Postoperatively, the elbow was immobilized with a long upper limb cast.
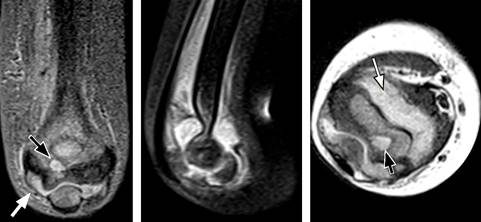
Figure 2: The magnetic resonance imaging image revealed abundant joint fluid (white arrow) and a lytic aspect at the level of the distal humerus (black arrow).
Osteomyelitis was considered, and an intravenous antibiotic treatment with Vancomycin (40 mg/kg/day) and Ceftazidime (50 mg/kg/day), was promptly initiated. Forty-eight hours later, a yeast growth in the blood agar and thioglycollate broth culture media. Therefore, Caspofungin (50 mg/m2/day) was also added to the treatment. On day 8, Candida tropicalis was isolated using the Vitek MS mass spectrometry method and pathological anatomy results showed an active chronic inflammatory process.
The patient showed signs of clinical improvement without fever for 12 days. However, experienced later on, a new febrile episode associated to mild pain and limited function in the right elbow joint, without any signs of inflammation or redness around the wound. A follow-up MRI revealed a new organized collection, mainly in the posterior region of the trochlea and humeral metaphysis (Figure 3). Consequently, a second surgical toilette and debridement had to be performed using a new trans-tricipital approach. Abundant purulent material and friable whitish tissue were obtained, which tested positive for C. tropicalis as well. After the second surgery, the patient had a favorable outcome, remained free of fever and pain, and showed progressive improvement in elbow mobility. She was discharged 15 days after the second surgery with an oral antifungal treatment: fluconazole (10 mg/kg/day) orally for six months, and continued to received her antibiotic prophylaxis with trimethoprim-sulfamethoxazole (10 mg/kg/day) orally for eight weeks.
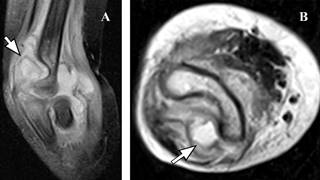
Figure 3: Sagittal and axial images of the new magnetic resonance imaging show evidence of an organized collection in the posterior region of the trochlea and humeral metaphysis (white arrow).
After three years of follow up, the patient did not develop episodes of infection recurrence and no joint sequelae were observed (Figure 4).

Discussion
Acute lymphoblastic leukemia (ALL) stands as the most common oncologic pathology in children and adolescents, with an estimated incidence of 26% among patients aged 0 to 14 years.6 Children with ALL may experience musculoskeletal symptoms such as bone pain and joint effusion, which are often unresponsive to painkillers but gradually improve with chemotherapy.1 Riccio et al.4 evaluated the incidence of osteoarticular complications arising from pediatric acute leukemia treatment. They described an incidence of 78.5% of bone/joint pain in the group with symptoms of the appendicular skeleton (n = 56). However, 12.5% presented septic arthritis-type symptoms (including pain, tumefaction, heat, reduced mobility, and fever), and 8.9% had osteomyelitis-type symptoms (such as fever, shivering, and intense localized pain). All the patients included in their study had negative culture tests, consistent with our case. In our case, the osteolytic lesion at the level of the humeral epiphysis evident in the X-ray led to osteomyelitis suspicion. Therefore, antibiotics to cover both gram-positive and gram-negative bacteria were initiated after obtaining the sample.
Fungal infections can have an incidence of up to 19.2% in ALL pediatric patients, representing one of the main causes of morbidity and mortality.7 Despite being associated with leukemia patients, bone infections by fungal microorganisms is rare. In a multicenter study including 123 pediatric patients with ALL and an associated fungal infection, only 2 exhibited osteoarticular involvement.8Candida infection is indeed one of the most common fungal infections, and C. albicans remains as the most prevalent Candida species, accounting for 56.6% of cases. Non-albicans species such as C. parapsilosis, C. glabrata, and C. tropicalis show lower incidences (18.9, 9.4 and 9.4%, respectively).9
C. tropicalis is strongly associated with ICU patients, especially in oncology patients who require prolonged intravenous devices, and/or broad-spectrum antibiotics.10-12 The infection can be acquired endogenously, where a colonized individual spreads the microorganism through the gastrointestinal tract to different anatomical sites, or exogenously, through catheters, implantable prosthesis, or parenteral solutions that were previously contaminated, causing several invasive infections, most commonly candiduria and candidemia.13 Its high virulence is notably attributed for its biofilm formation ability as well as adhesion to host surfaces (epithelial cells and medical devices).14,15
Early diagnostic suspicion is crucial for successful therapy. The combination of appropriate surgical debridement and antifungal therapy is critical for clinical resolution of the infection.16 Neofytos et al.9 reported that 52.8% (n = 28) of their cases underwent a surgical intervention for osteomyelitis management, with 100% of C. tropicalis cases requiring debridement. In our case, initial surgical debridement may have been insufficient. Hence, it is important to highlight the need of an aggressive approach when addressing osteoarticular infections surgically.
Regarding pharmacologic therapy, there is no strong consensus in the literature regarding the appropriate management of these infections. The guidelines from the Infectious Diseases Society of America (IDSA)17 suggests the use of echinocandins (caspofungin, micafungin); however, they particularly emphasize fluconazole for C. tropicalis infections, recommending a treatment duration of 6 to 12 months. In our case, a 6-month course of fluconazole, combined with 2 surgical debridement, was effective in controlling the infection and yielded favorable postoperative results without bone sequelae.
In conclusion, osteomyelitis by Candida tropicalis represents a severe condition that should be included in the differential diagnosis of osteoarticular complications in immunocompromised patients with ALL. The insidious and oligosymptomatic presentation demands a high index of suspicion for timely diagnosis and appropriate treatment. We suggest aggressive surgical debridement in cases of C. tropicalis osteomyelitis due to the high virulence of these fungal species.

