











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Surface sarcomas are a rare entity that need correct diagnosis to differentiate parosteal (cPOS), periosteal and the high grade surface osteosarcomas (HGSO). HGSO has malignant behavior similarities with osteosarcomas and wide resection is the key to a successful treatment.1 The Capanna and Hemi-Capanna reconstruction techniques have being developed in order to avoid amputation after an oncological resection, allowing structural support from an allograft and biological advantages from a vascularised autograft.2,3
This case report presents a case of HGSO in the proximal tibia shaft. In order to achieve diagnosis various biopsies were performed, Finally, it was treated with an oncological resection followed by Hemi-Capanna reconstruction using the ipsilateral vascularised fibula with excellent results.
The patient was informed that data concerning his case would be submitted for publication and he provided consent.
Case report
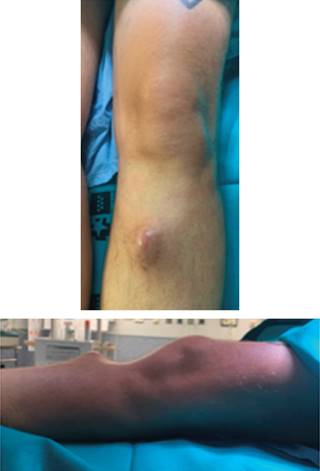
A 46-year-old man presented at the clinic with knee pain and a 4 × 3 cm soft tissue tumor on the right tibial. His medical history included sporadic tobacco and alcohol consumption and up to six pneumothorax episodes, needing surgery 13 years prior to consultation. He refers onset of tumoration the previous year without trauma, and sudden increase in size in the last month. Physical examination showed a 4 × 3 cm soft tissue tumor on the proximal aspect of the anterior left tibia, hard and painful to touch, attached to deep structures (Figure 1).
Initially a XR, CT and MR were performed showing a soft tissue tumor on the proximal aspect of the left tibia just inferior to the tibial tuberosity, size of 40 × 29 × 19 mm (coronal × sagittal × axial). Emerging from the anterior tibia periosteum and growing towards the subcutaneous tissue, hyperintense in T2 and hypointense in T1. Tumor presents with irregular and extensive internal calcifications (Figure 2). An initial biopsy was performed that was inconclusive, so an ultrasound guided biopsy was done afterwards with a 14G needle. The pathologist could not conclude between, hypertrophic fracture callus, osteoblastoma or osteosarcoma subtype osteoblastoma.
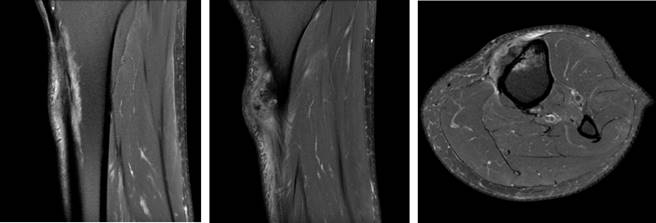
Figure 2: MR image of the tumor showing growth from the anterior periosteum and internal calcification. Soft tissue invasion can be seen.
Three months later MR was repeated showing increase in size 42 × 40 × 27 mm and small areas of necrosis. Large attachment to the anterior periosteum remains with exophytic growth contacting the skin (Figure 3). With new imaging a third biopsy was performed guided with ultrasound. It showed trabecular osteoid areas that converge and areas of spindle cells with moderate cellular atypia, that suggested cPOS or HGSO.
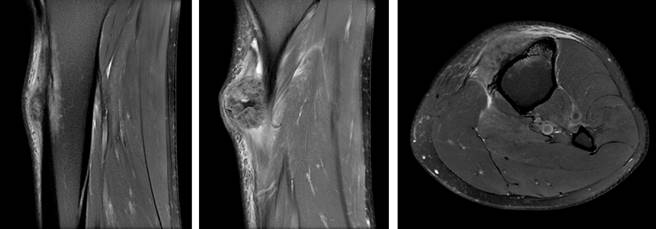
Figure 3: MR image of the tumor showing growth compared with previous image. Contact with the skin can be noted.
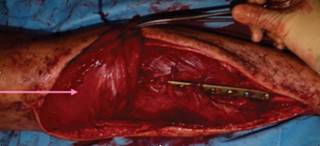
Surgery was performed by the orthopedic and plastic surgery team under general anesthesia. First a medial approach was performed accessing to the posterior compartment and identifying neuromuscular bundle. Extensive resection that included 15 cm of tibial shaft, surrounding soft tissue and 7 cm skin flap was performed securing intraoperative free edges. The tibial tuberosity and patellar tendon were left intact. Second a lateral approach over the fibula was performed, dissection of the peroneal artery and interosseous membrane, proximal and distal fibula osteotomy leaving 7 cm and 6 cm left correspondingly, followed by fibula tunneling to the anterior compartment (Figure 4).
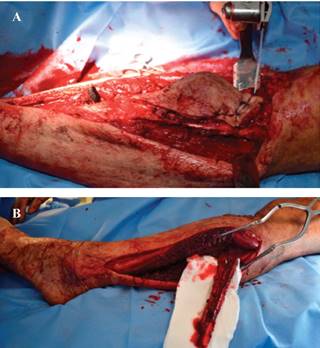
Figure 4: A) Medial approach with proximal tibial and skin resection. B) Lateral approach with fibula graft, peroneal artery can be identified.
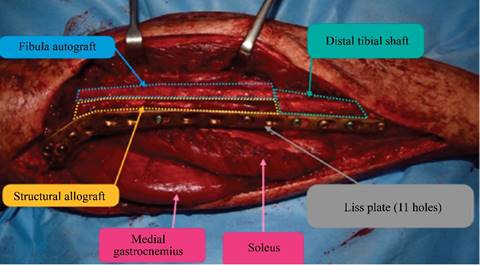
On an auxiliary Table allograft preparation was performed with diaphyseal and metaphyseal osteotomy. With a long LISS plate osteosynthesis was done over allo and autograft mounting. Two cortical screws were used to ensure fibula and allograft compression (Figure 5). Finally, a pedicled medial gastrocnemius flap and free skin flap was used to cover soft tissue defect (Figure 6).
After six weeks non weight bearing patient started partial weight bearing and physiotherapy. Surgical sample was analyzed and was diagnosed as HGSO. The pathology analysis confirmed a HGSO (Figure 7).
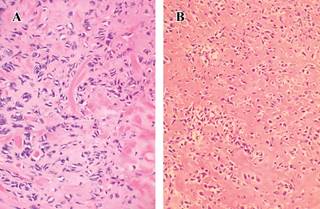
Figure 7: A) Tumor formed by cells with much nuclear pleomorphism (H&E, ×400). B) Cellular proliferation of diffuse growth pattern in which osteoid material is identified around the neoplastic cells (H&E, ×200).
The patient underwent four rounds of chemotherapy with Cisplatin and Adriamycin. During follow-up patient underwent genetics examination and was positive for the following biomarkers FGFR1, MYC, RICTOR, CUL4A, ZNF703, C17orf39, IRS2 and WHSC1L1, being diagnosed with Li-Fraumeni Syndrome.
After 15 months’ follow-up no evidence of recurrence or metastasis appeared on MR or PET-SCAN. He undergoes periodical colonoscopies and examination and no new tumors have been found. Patient is satisfied, walks with a cane and reports no pain.
The patient was informed that the data on his case would be submitted for publication, and he gave his consent.
Discussion
The vast majority of sarcomas arise intramedullary thus the Surface Osteosarcomas subtype are rare, representing 4-6% of all sarcomas.4,5 The main variants of surface osteosarcomas are the cPOS, periosteal and the HGSO, representing 5, 1.5 and 0.5% respectively.1 HGSO are highly malignant lesions that bear similarities to conventional intramedullary osteosarcoma, having the ability to metastasize and cause death. They occur more frequently in males than females (1.6:1),6,7 during the second and third decades of life7 with a mean age of 25 years old6 They most frequently involved the mid femur followed by distal femur and mid tibia6 and usually measures 5-22 cm at initial presentation.7 Pain and swelling are the usual presenting symptoms. Diagnosis needs to be performed with a biopsy or surgical piece, but it remains tricky due to superficial affection.
As a high grade tumor, it is highly proliferative and may present with satellite lesions and early metastases, 15% probability of pulmonary metastasis.6,7 The treatment of choice is a combination of wide surgical excision and adjuvant chemotherapy.5,6 H. Nouri et al, recommend the use of chemotherapy postoperative only, because of the amount of poor response and the high risk of progression during treatment.1
The prognosis for HGSO is worse than for the other two types of surface osteosarcoma. The following are described as risk factors for worst prognosis: proximal location in limbs, increased size, metastasis at diagnosis and poor outcome after chemotherapy.8 The latest is one of the most important prognosis factors, considering good response to chemotherapy more than 90% of necrosis/sclerosis.9 The second most important factor is surgical margins, being local recurrence associated with marginal excision.1 Extension to the medullary canal is rare and also associated with worse prognosis.6 The survival rates at five years is 62.4%-82%, and disease free survival is 70%.1,7
In order to achieve free surgical margins wide resections need to be performed. Historically, amputation or disarticulation was the treatment of choice but a limb salvage surgery is more desirable, as it has being published no statistically significant difference in local recurrence rates, duration of postoperative disease-free period, or survival rates between limb salvage procedures and amputation.10 Options for limb salvage include the use of large cortical allografts, distraction osteogenesis, endoprosthesis, and vascularized bone grafts.2,11
The Capanna Technique is an excellent option to reconstruct the large defects of the femur and tibia left after an oncologic resection. It is recommended for defects larger than 10 cm.12 It combines a vascularized fibula autograft with a conventional massive allograft.3 The combination of allograft and autograft complement each other; the immediate structural strength provided by the allograft and the biological profiles of a vascularized fibula, with osteogenic capabilities and the potential to achieve lower rates of infection, fracture, and nonunion.
The free vascularized fibula harvested most commonly from the contralateral leg is at least 4-6 cm longer than the defect.12,13,14 The allograft is cut the same length as the bone defects. The fibula’s vascular pedicle is based on the peroneal artery with its venae comitantes, providing an endosteal nutrient artery to the medullary canal and periosteal branches that supply the cortical surface.
The classical Capanna Technique consists of inserting the harvested fibula carefully into a previously prepared allograft groove. At the tibial level the autogenous fibula is inserted 2-3 cm into the medullary canal of the distal tibial stump and proximally, it is placed at the center of the metaphysis or epiphyseal. When fibula insertion into de allograft care is taken to prevent damage to the vessels.15
The classical Capanna Technique constrains the fibula within the medullary canal of the allograft and does not fully allow hypertrophy over time. Thus, the evolution to the «hemi-Capanna». In this technique the allograft is buried within the medullary canal and then it is split in half longitudinally to accommodate the vascularized fibula. Bisecting the allograft increases the space available for the fibula in favor of osseous hypertrophy to take effect, and simplifying pedicle positioning and microsurgical anastomosis.2,14
While the «Hemi-Capanna» might result in decreased structural strength of the construct, it provides the benefit of increased exposure of the fibula graft to loads during weight bearing, which stimulates graft hypertrophy.16
In both the Capanna and Hemi-Capanna the construct is secured with plates and screws or with screws alone, and the microvascular anastomoses are performed after bony fixation, usually in an end-to-side fashion.
The overall success rate of the reconstruction is 93.5%. Complications included infection (6-8.5%), nonunion (6-10.5%), and fracture (10.5-13.3%).13,15
In conclusion the Hemi-Capanna technique is an evolution of the Capanna that uses its fundamental idea of allograft and vascularised autograft combination, but simplifies surgical technique and allows more graft hypertrophy site it is less constrained. It has proven to have excellent results in wide bone resections such as the ones performed at sarcomas or HGSO surgery.
Conclusion
HGSO are highly malignant lesions that bear similarities to conventional intramedullary osteosarcoma. It´s treatment of choice is a combination of wide surgical excision and adjuvant chemotherapy. The Capanna Technique is an excellent option after a wide excision, it´s evolution into the Hemi-Capanna simplifies the surgical technique and allows more graft hypertrophy, with excellent results in wide bone resections.

