











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Upgraded pain management can lead to rapid recovery, fewer postoperative complications and shorter duration of stay, which are the key features of the rapid recovery program.1,2,3 In addition, the side effects associated with opioid use, including nausea, vomiting, respiratory depression, hypotension, decreased bowel movements and urinary retention cannot be ignored and should be minimized.4
However, total knee arthroplasty (TKA) may be associated with severe postoperative pain, which often requires prolonged hospitalization to provide effective analgesia. This long stay in the hospital and the patient’s instability may cause unwanted medical problems such as nosocomial infection, deep vein thrombosis (DVT) and adverse side effects of surgery. Adequate management of postoperative pain following TKA poses a significant challenge, as most patients (up to 58%) experience moderate to severe pain on the first day of operation.5 Multiple options like peripheral nerve block, epidural infusion, as well as patient-controlled analgesia (PCA) are taken to control pain but regrettably all have limitations.
An innovative approach to pain management is to aim at controlling local pain pathways and receptors within the knee. This has been possible through local intraarticular or periarticular injection of analgesic combinations which has good efficacy, is cost-effective, and is easy to administer without causing motor blockade. Also, it does not require any special technical skill for administration.6
A multimodal pain program incorporating periarticular injection represents a significant advancement in perioperative pain management following total knee arthroplasty. Although the gold standard for the cocktail formula has not yet been set up, the components always contains local anaesthetics (ropivacaine and bupivacaine), epinephrine, steroids, opioids and nonsteroidal anti-inflammatory drugs (NSAIDs).6,7,8,9 However, whether those compositions are all necessary is still to be investigated considering the efficacy and safety. So we have conducted a retrospective study with a hypothesis that modified Ranawat Cocktail Regimen is safe and effective in decreasing postoperative pain and morbidity following Total Knee Arthroplasty.
Material and methods
Study design: this is a retrospective study of 116 patients of primary osteoarthritis undergoing total knee replacement at a tertiary Centre of North India were included in the study. All included patients signed an informed consent form, and the methods for this trial were approved by the local ethics committee (GGS/IEC/36).
Data collection: the data from August 2017 to December 2021 of patients with primary osteoarthritis knee who underwent TKA retrieved from the main operation theatre, record room (admission file) and radiodiagnosis department regarding all the in-patient details. Apart from this the follow-up details were collected from the discharge card, outpatient department slip, follow up X-Rays from radiodiagnosis department along-with the telephonic conversation on patient’s personal contact number. The two groups so formed in terms of LIA and normal saline infiltration as sham injection (control group) were compared.
Inclusion criteria includes patients of both the sex having grade III and grade IV primary osteoarthritis knee. Exclusion criteria consist of patients suffering from rheumatoid and other secondary arthritis, patients with connective tissue disorders, who are medically unfit for surgery, with previous history of cardiac disease, coagulopathies or hypersensitivity to any of the cocktail constituents and revision TKA patients.
Procedure: in this study, we used 35 ml of LIA for deep infiltration consisting of the modified ranawat regimen for TKA patients which contains (ropivacaine with adrenaline(10 + 1 ml), methylprednisolone (1 ml), morphine (1 ml), ketorolac (2 ml) and normal saline (20 ml) whereas 14 ml of superficial infiltration with 7ml each of ropivacaine and normal saline to manage postoperative pain in all 58 patients presenting to our institute for primary TKA.9 The differences from Ranawat cocktail were the inclusion of ropivacaine (it is less cardiotoxic than bupivacaine), lesser volume and antibiotic (already mixed with bone cement). The control group of 58 patients had the placebo control sham injection of normal saline.
The cocktail was injected 7 ml each at the following 7 zones which includes 5 deep and 2 superficial zones: zone 1: anteromedial zone, 2: posteromedial zone, 3: medial retinaculum, 4: anterolateral zone. 5: posterolateral zone, 6: patellar tendon and fat pad zone (superficial LIA). 7: cut ends of quadriceps muscle and tendon (superficial LIA). Deep LIA was given before implant and superficial after final implant insertion (as shown in Figures 1 to 6).10






Postoperative pain was assessed using numerical rating scale (NRS) with the aim to keep the postoperative NRS score below 5. All the patients received 1 g/100 ml paracetamol infusion 8 hourly as per institutional protocol, if the patient still complains of pain and has NRS score above 5 at 6 hours postoperatively then diclofenac 75 mg/2 ml intramuscular was given as rescue analgesic and NRS score 5 or above at 9 hours then the rescue analgesia started in the form of injection tramadol infusion 50 mg/2 ml in 100 ml of normal saline was kept as second rescue analgesic and if the NRS score still persist above 5 after 3 hours of tramadol infusion then morphine 1 mg infusion given as third rescue analgesic.
Outcome was assessed in terms of post-op NRS score, morbidity index (as shown in Table 1), analgesic consumption and functional milestones achieved.
Table 1: Morbidity index.
| Sr no. | Activities | Score 0 | Score 1 | Score 2 | Score 3 |
|---|---|---|---|---|---|
| 1 | Knee ROM | No extensor lag, flexion > 90 | Lag < 10 Flexion 60-90 |
Lag > 10 < 20 Flexion 30-60 |
Lag > 20 Flexion < 30 |
| 2 | Power | Can do active SLR | Can do active SLR but cannot sustain for more than 5s | Needs initial support for active SLR | Cannot do active SLR |
| 3 | Ambulation | Able to walk independently | Able to walk with stick | Able to walk with walker | Unable to stand |
| 4 | Pain | Mild or no pain | Pain tolerable with oral medications | Requires systemic medications to control pain | Severe pain despite of systemic medications |
| 5 | Wound status | Clean | Mild spotting | Minimal soakage or drain < 300 over 24 hours | Complete soakage or drain > 300 over 24 hours |
| 6 | Bladder | Can pass urine comfortably | Frequency but no retention | Less control and incomplete emptying | Require catheterization |
| 7 | Vital signs | Pulse and BP stable and input and output maintained | Needs mild support Not affecting mobilisation |
Needs more support severe enough to affect mobilisation | Needs continual support (ICU) |
| 8 | Attitude | Happy | Enthusiastic but anxious | Concerned | Unhappy |
| 9 | Sleep | Sleeping well | Sleep less than normal | Sleep with help of sedatives | Could not sleep even with sedatives |
| 10 | Appetite | Normal | Less | Loss of appetite with nausea and vomiting | Severe anorexia |
Sr no. = Serial number. ROM = Range Of Motion. SLR = Straight Leg Raise Test. ICU = Intensive Care Unit.
The analysis was performed using descriptive and inferential analysis (t-test for parametric and Mann-Whitney for non-parametric results). A p-value of < 0.05 was accepted as statistically significant. Morbidity index includes a total of ten components which are ROM, power, pain, ambulation, wound status, bladder functioning, vital signs, attitude, sleep and appetite.11
Results
Demographic and intraoperative data were comparable in both the groups (Table 2).
Table 2: Demographic and intraoperative profile.
| Sr no. | Local infiltrative anaesthesia group | Control group | |
|---|---|---|---|
| 1 | Male Female |
27 31 |
30 28 |
| 2 | Mean age, (years) | 62.5 | 59 |
| 3a | FFD (< 10) | 17 | 21 |
| 3b | FFD (10-20) | 31 | 32 |
| 3c | FFD (> 20) | 10 | 5 |
| 4a | Varus (< 10) > 20 | 14 | 17 |
| 4b | Varus (10-20) | 37 | 35 |
| 4c | Varus (> 20) | 7 | 6 |
| 5 | Average tourniquet time, (mins) | 81 | 84 |
| 6 | Diabetes Asthma Coronary artery disease Renal impairment |
7 1 11 2 |
5 0 9 3 |
Sr no. = Serial number. FFD = fixed flexion deformity.
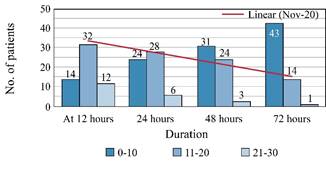
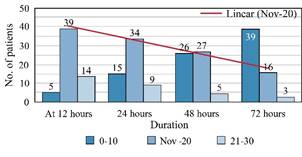
As per morbidity index the mean score on day one was 16.18 and 23.40 which decreased to 6.37 and 9.21 by day three in LIA (as shown in Figure 7 ) and control group (as shown in Figure 8 ) respectively indicating morbidity has decreased but more so in LIA group. On postoperative day three 71% (n = 43) patients had excellent result, 27% (n = 14) patients had good result and 2% (n = 1) patient had poor result in the LIA group.
The mean NRS score was significantly lower in LIA group (3.2) as compared to control group (3.9) in first 24 hours but after that results were non-significant (Table 3).
Table 3: Mean numerical rating scale score.
| Sr no. | Postoperative duration, (hours) | LIA group | Control group | p |
|---|---|---|---|---|
| 1 | 12 | 4.1 ± 1.9 | 4.9 ± 1.6 | 0.009 |
| 2 | 24 | 3.2 ± 1.1 | 3.9 ± 1.5 | 0.07 |
| 3 | 48 | 2.8 ± 1.2 | 3.2 ± 1.1 | 0.21 |
| 4 | 72 | 2.5 ± 1.7 | 2.8 ± 1.3 | 0.33 |
Sr no. = Serial number. LIA = local infiltrative anaesthesia.
Functional milestones were relatively achieved earlier in LIA group but the values were not significant. Total hospital stay was 4.6 days in LIA group as compared to 5.3 days in control group (Table 4).
Table 4: Showing functional milestones.
| Sr no. | Milestones | Duration, (days) | p | |
|---|---|---|---|---|
| LIA group | Control group | |||
| 1 | Sitting bedside | 1.2 ± 0.8 | 1.5 ± 0.4 | 0.33 |
| 2 | 90 degree range of motion | 1.4 ± 0.4 | 1.3 ± 0.6 | 0.88 |
| 3 | Standing with walker | 2.5 ± 0.7 | 2.9 ± 0.7 | 0.71 |
| 4 | Walking with walker | 2.9 ± 0.7 | 3.1 ± 0.8 | 0.82 |
| 5 | Total hospital stay | 4.6 ± 1.2 | 5.3 ± 1.1 | 0.12 |
Sr no. = Serial number. LIA = local infiltrative anaesthesia.
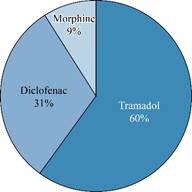
Tramadol (58%) and diclofenac (23%) were the most commonly drugs used for rescue analgesia (as shown in Figure 9 ). Tramadol consumption was remarkably higher in control group as compared to LIA group (34:13).
Discussion
The primary aim of performing total knee arthroplasty (TKA) in patients is to provide pain free knee and increase the quality of life among patients by facilitating early mobilization. But due to insufficient postoperative pain management there is a delay in the rehabilitation process among patients and a high rate of disappointment with the procedure.12 Therefore, an adequate and efficient post-operative analgesia protocol is the absolute necessity and one of the most workable methods is found to be multimodal approach using local infiltration analgesia (LIA).13 The use of LIA has also been associated with better patient satisfaction and decreased opioid consumption.13,14,15 The main disadvantages of LIA is usually seen due to the high doses of local anaesthetic used in the cocktail and is associated with cardiotoxicity and CNS toxicity in some elderly patients which may be fatal, consequently are relative contraindications in such patients.13
Literature about periarticular injection have reported good results from various medications and combinations but the ideal dose and combination are yet to derive.13,14,15 In our cocktail, Ropivacaine was used instead of bupivacaine because it is less cardiotoxic and most of the knee arthroplasty patients are elderly with a variable degree of compromised cardiac status, antibiotic was withheld as we use antibiotic mix cements and lesser volume of infiltration was used to decrease the overstuffing of knee joint.
To assess the postoperative patient condition, morbidity index is one of the most comprehensive scoring system designed for early postoperative period in total knee arthroplasty. The WOMAC (Western Ontario and McMaster Universities Index) and the Oxford Scores include only the functional abilities to carry out certain activities of the operated knee but does not include other parameters of recovery such as wound status, bladder activity, sleep, appetite, mental status and so on. Furthermore, these scores are not applicable on early postoperative day. On postoperative day three in LIA group, 71% (n = 43) patients had excellent results because of less pain, better sleep and enthusiastic attitude. 27% (n = 14) patients had good result and 2% (n = 1) patient had poor result with overall declining morbidity and better results than control group which is in concordance with Shah et al.11
Average NRS score in LIA group on day 1, 2 and 3 was 3.2, 2.8 and 2.5 respectively showing promising trend towards minimal pain and was significantly lower on day 1 than control group and consequently shorter hospital stay. Lisi et al. had similar results with scores below 3 after 3rd postoperative day.16
LIA cohort patients were able to sit with 90° ROM at an average time of 1.4 days. The mean time required to attain the standing position was 2.6 days favouring Issac et al. and Crawford et al. studies which had parallel functional outcome Figures. The similar milestones were slightly delayed in control group but the difference was non-significant which could be attributed to more multifactorial dependence of functional milestones.17,18
Berger et al proposed for TKA patients a protocol with ambulation starting in few hours after surgery and following discharge on the same day of surgery; however, this protocol may lead to a surge in readmission rates.19,20 In our study, the majority of the patients could walk with support within three days and similar results were obtained by multiple studies.21,22
Use of tramadol infusion as rescue analgesia was significantly more in control group on day 1 and 2. 60-65% of the analgesia had to be given on day 1, followed by 28% on day 2 and 9% on day three which are in line with the Tarun et al.23
So our study inferred that use of modified cocktail regimen in the knee effectively decreased morbidity with excellent to good results, declining NRS score, minimal rescue analgesia requirement, early ambulation with better safety. A good preoperative counselling regarding the whole procedure, proper surgical technique and adequate postoperative pain management along-with defined physiotherapy protocols are the key to a painless total knee arthroplasty. Despite several limitations our study will add valuable addition to the previous literature.
As we have observed that effect of LIA fades after 48 hours and results in both the groups are comparable on day three so we suggest that a future research directed towards patient matched ropivacaine dose and sustained release anaesthetic drug can be used to obtain long lasting pain relief.
Limitations: retrospective study, small sample size.

