











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Conventional parosteal osteosarcoma is an uncommon malignant bone tumor, comprising 4% of all osteosarcomas. Although rare, parosteal osteosarcoma is the most common type of osteosarcoma of the bone Surface.1),(2 Conventional Parosteal osteosarcoma is a slowly progressive tumor that carries better prognosis than the classical, high-grade osteosarcoma. The treatment for this type of tumor is wide surgical resection and the adequacy of surgical margins appears to be the most important prognostic factor, since inadequate margins were reported to be associated with local recurrence, dedifferentiation and metastases.3 Parosteal osteosarcoma can be of two types: conventional or dedifferentiated. Histologically, conventional Parosteal Osteosarcoma is a low grade malignant tumor composed of parallel arrays of osseous trabeculae intermixed with fibroblast-like tumor cells with bland-looking nuclei.4 Dedifferentiated Parosteal Osteosarcoma is a variant of osteosarcoma in which a high-grade sarcoma coexists with a conventional parosteal osteosarcoma.5 Cartilage differentiation is present in parosteal osteosarcomas in about 25-55% of cases, usually is located at the peripheral portion of the tumor where it can simulate an osteochondroma, but it may also be present as isolated nodules in the tumor.6
Recently a rare histologic variant of parosteal osteosarcoma characterized by the presence of low grade liposarcoma component has been described.7),(8
Here we present a case of a parosteal osteosarcoma in which a low grade liposarcoma and also a low grade chondrosarcoma component are present.
Case report
Clinical History: a 36-year old woman began her condition one year prior to admission to the hospital with increased volume in the left knee and pain with a VAS of 4/10. In the last 3 months she mentioned pain exacerbation, with a VAS of 7/10, increased volume and difficulty to walk.
Image studies
Anteroposterior and lateral radiographs of the left knee showed an exophytic and lobulated bone tumor attached mainly to the posterior surface of the distal third of the diaphysis and distal femoral metaphysis. The tumor presented central dense ossification and a thin, radiolucent zone between the tumor and the underlying bone (Figure 1).

Figure 1: Anteroposterior radiography (A) and lateral (B) of the left knee. Lobulated and exophytic bone tumor with central dense ossification, adjacent mainly to the posterior surface of the distal third of the diaphysis and distal femoral metaphysis. Presence of radiolucent cleavage (arrows) that separates the tumor and the adjacent normal cortex (sign of the rope) which corresponds histologically to the periosteum interposed between the cortex and the tumor mass.
Computerized Tomography showed a juxtacortical and heterogeneous tumor on the posterior surface of the femur There were hypodense and hyperdense areas. The bone marrow was not involved (Figure 2).
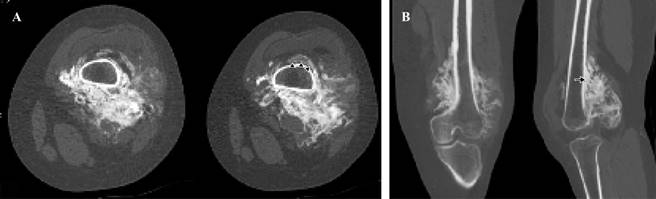
Figure 2: Computerized Tomography. Axial cut (A), Multiplanar reconstruction (B). Presence of juxtacortical tumor on the posterior surface of the metaphysis and distal third of femoral diaphysis, showing abundant ossification, which surrounds almost the entire circumference of the femur, identifying the sign of the rope (arrowheads) and cortical thickening (arrow). The bone marrow is respected.
Magnetic Resonance showed a heterogeneous tumor, with large areas of low signal strength in all the sequences, alternating with areas of fat behavior) and zones of intermediate intensity (Figure 3).
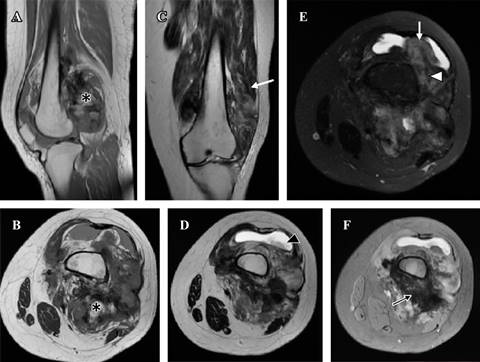
Figure 3: Magnetic Resonance. (A y B) T1 sagittal and axial, (C y D) T2 coronal and axial, (E) T2 with coronal fat saturation, (F) Gradient echo in axial plane. Heterogeneous tumor, with large areas of low signal strength in all the sequences, in relation to tumor ossification (black arrow), alternating with areas of greasy behavior (*) intermediate intensity zones (white arrowhead), infiltrating both vastus muscles, mainly the lateral and suprapatellar recesses (white arrow), conditioning joint effusion (black arrowhead).
Nuclear Medicine: Gamagraphy with 99mTc-MIBI reported a bone lesion, with extension to adjacent soft tissues, with an abnormal increase in the radiopharmaceutical. The greater uptake of the lesion was towards the lateral región. The SPECT/CT reported an exophytic bone lesion, located in the metaphysis, with heterogeneous appearance, and abnormal increase in the radiopharmaceutical. The lesion showed multiple positive focal zones (Figure 4).
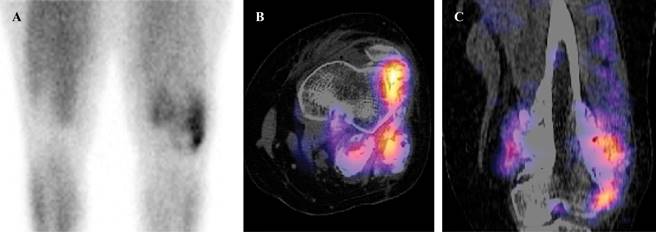
Figure 4: Gammagraphy (A) There is abnormal increase in the radiopharmaceutical in soft tissues. The greater uptake of the lesion was towards the lateral region. SPECT/CT axial (B) and sagittal (C). Presence of multiple focal zones of abnormal increase in the radiopharmaceutical.
An incisional biopsy was performed, and the histology showed well differentiated osseous trabeculae and spindle-cell stroma without nuclear atypia or mitotic Figures. With the pathology diagnosis of a Parosteal Osteosarcoma a wide surgical resection was undertaken.
The surgical piece showed a well delimited and superficial tumor, that didn’t affect the bone marrow but with apparently intraarticular extension. The tumor was about 18 × 9 × 7 cm3 with major tumoral volume in the femoral posterior surface but also with lateral, medial and anterior surface affection and articular extension. The tumor had a heterogeneous aspect. In the periphery of the tumor there were present bland and yellow zones that alternate with white and hard zones. The interior portion of the tumor consisted in very hard white-gray tissue. Also in different zones there were bluish-white and rubbery cartilaginous-looking areas (Figure 5).
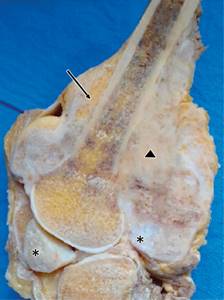
Figure 5: Surgical piece sagittal cut. A juxtacortical tumor that surrounds almost the entire circumference of the femur and does not invade the medullary cavity. The tumor is heterogenous with yellow adipose zones (black arrow) alternating with white-hard zones () and multiple bluish-white cartilaginous looking areas (*).
Microscopically in the yellow zones of the tumor there were observed adipocytes of different sizes. These adipocytes were present in two growing patterns: pushing borders that rejected the bone trabeculae and also infiltrative pattern between the fusiform cells and the parallel bone trabeculae. There was heterogeneity in the size and shape of adipocytes and also there were lipoblast focally. These zones were interpreted as low grade well differentiated liposarcoma (Figure 6).
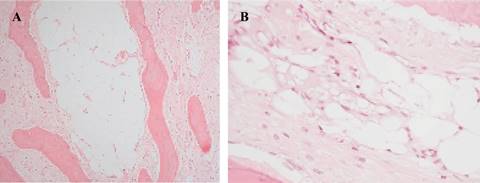
Figure 6: Photomicrography of the adipose component. (A) 20×. There is adipose tissue between bone trabeculae. (B) 40× Adipocytes of different sizes and shapes are observed, as well as small multivacuolate cells whose nuclei are rejected towards the periphery. These correspond to lipoblasts.
The cartilaginous component was hyaline, hypocellular, without chondrocyte atypia and arranged in two ways: one consisted of well delimited nodules (Figure 6A), and the other consisted on cartilage zones with endochondral ossification on their periphery (Figure 6B). In these endochondral ossification areas, focal infiltration by myxoid matrix into the intertrabecular space was found and interpreted as low grade chondrosarcoma (Figure 7).
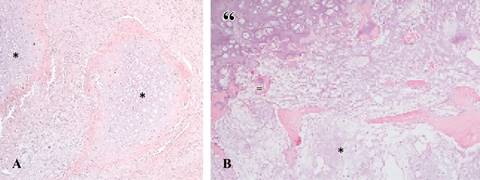
Figure 7: Photomicrography of the cartilaginous component. (A) 20× There are two nodules of hyaline cartilage. The nodules are well limited and there is no atypia (*). (B) 40×: Another area of the tumor that shows hyaline cartilage (“), endochondral ossification (=) and bone trabeculae between which there is abundant myxochondroid matrix with moderate cellularity (*).
The conventional parosteal osteosarcoma was also present and was characterized by well differentiated osseous trabeculae and spindle-cell stroma without nuclear atypia or mitotic Figures. Trabeculae were long and disposed in parallel or irregular shaped array (Figure 8).
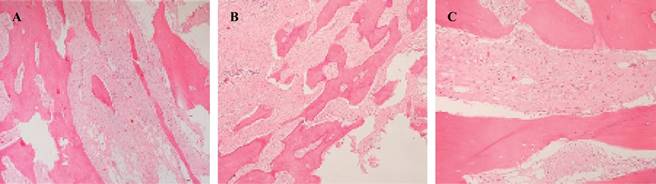
Figure 8: Photomicrography of the osseous component. (A, B) 20× Bone trabeculae disposed in parallel and fusiform cells between them. (C) 40×. The cells in the spindle cell stroma are fusiform and have no nuclear atypia.
Immunohistochemistry was positive for MDM2 and CDK4 in the nuclei of fusiform cells present between bone trabeculae and that alternate with adipocytes. IDH1 was focally positive in the nuclei of some chondrocytes.
The surgical piece pathology diagnosis was: Parosteal Osteosarcoma with low grade chondrosarcoma and liposarcoma components.
Discussion
In retrospective, the adipose and the cartilaginous components were present in the image studies. However, these components were not present in the initial biopsy. Only in the surgical piece the low grade liposarcoma histology was evident: adipocytes of different sizes and shapes and lipoblast. On the other hand, the chondroid component of the tumor, which was also not present in the initial biopsy, was mostly composed of well-defined nodules of hypocellular hyaline cartilage without atypia. Only focally there were zones with abundant myxochondroid matrix between bone trabeculae.
The knowledge of this rare parosteal osteosarcoma variant can lead the orthopedic oncologists to avoid overlooking the adipose component and provide adequate surgical margins. For pathologists the knowledge of this variant may lead to request a biopsy from multiple sites in order to not misdiagnose the tumor or to mention in the description that the other components observed in the image studies are not present in the biopsy.
There are only two previously reported cases of parosteal osteosarcoma with a low-grade liposarcoma component. One of these cases was present in a 34-year-old woman, with a slowly growing mass in upper humerus.7 The other case was present in a 37-year-old female with a long -standing juxtacortical mass of the proximal tibia.8 In both cases, as well as in our case, imaging studies revealed a heterogeneous parosteal mass and there was no medullar cavity involvement. However, none of the previous reported cases also had a cartilaginous component, like our case.
In parosteal osteosarcomas the low grade liposarcoma and the low grade chondrosarcoma components may be scarce and focal. This may be one reason why they may be overlooked.
Considering only the histology, the differential diagnoses will depend on what component is present and predominant in the biopsy: well differentiated liposarcoma of soft tissues or low grade chondrosarcoma. However, these differential diagnoses are ruled out when doing correlation with imaging studies. That is why in cases like this one that we present, the clinical-radiological correlation, as well as obtaining a representative biopsy for histopathological study, is of utmost importance.
The presence of the lipomatous and cartilaginous components in parosteal osteosarcomas could be explained by the fact that periosteum contains mesenchymal stem cells with proliferative capacity that have osteogenic, chondrogenic, and adipogenic potential, so called tripotency.9),(10),(11
This proliferative capacity allows periosteal cells to differentiate into adipose tissue, cartilage tissue or bone tissue.
Further case reports and studies of this rare parosteal osteosarcoma variant are necessary to establish the prognosis of patients.

