











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
Social isolation represents a critical condition that, particularly during the pandemic period, affected children (Torres González et al., 2020). Furthermore, recent research suggests it may influence their mental health (Padilla-Bautista & Galindo-Aldana, 2022), emotional intelligence, and overall development (Pallotto et al., 2021). Nevertheless, specific details regarding its impact on the mental health of children in residential care homes (RCHs) during that period, as well as its developmental consequences remain unknown. The United Nations International Children’s Emergency Fund (UNICEF) indicates that, although considerable progress has been made globally during the last decade in improving the living conditions of children and adolescents, this advancement has been uneven. Factors such as poverty and inequality affect their lives, becoming barriers that prevent the complete realization of their rights and development (UNICEF, 2024).
Evidence indicates that people living in vulnerable conditions may experience social isolation more severely (Padilla-Bautista & Galindo-Aldana, 2022). In Mexico, the nearly 40 million children and adolescents represent a third of the country’s population and face diverse realities (Cookson et al., 2021). For instance, it is increasingly common to encounter children and adolescents working in public spaces to fulfill their daily needs. These problems and lifestyles are part of an expanding phenomenon rooted in economic adversity and domestic violence, among other factors, which compels families to incorporate minors into economic activity or can lead to abandonment (Selmani-Bakiu & Elezi, 2021). Children in vulnerable conditions are susceptible to living in the street, becoming victims of human trafficking, and/or working in conditions detrimental to their development and physical and mental well-being, among other risks (Rizzoli-Córdoba et al., 2017). The degree of vulnerability of children is defined by their exposure to risk factors and their capacity to face or resist problematic situations (Franchino-Olsen, 2021; Merikangas et al., 1999).
Governmental, civil, as well as religious organizations have devised strategies, through specific programs and social assistance initiatives, to address the needs of children facing these deprivations (Bautista-Otero & García-Ubaque, 2012). As a result, there are 703 institutions in Mexico focused on the attention and care of minors. These establishments serve as a source of support, and even a survival mechanism, for these young individuals. While approximately 412,456 children lack parental care, only 29, 310 reside in these social assistance institutions. There is no record of the remaining, so the number could be much higher (Curiel-Arévalo et al., 2010).
As mentioned before, placing children in institutions, such as RCHs, has been suggested as an exceptional and temporary protective measure with the purpose of removing them from a risky situation and safeguard their rights until their circumstances improve, facilitating their reintegration into their family of origin or, in more severe cases, adoption may be offered to them. Several studies (Hagaman et al., 2010; Yslado-Méndez et al., 2019) have demonstrated that the institutionalization of minors presents a wide variety of challenges for their development. Often, children in RCHs exhibit consequences stemming from the particular characteristics of their social environment, in addition to experiences of abandonment, separation, abuse and mistreatment-circumstances that are detrimental to their proper emotional development. Aspects depicting mental health risks in children living under vulnerable conditions have been identified by other studies (Rhodes, 2021), which state that these circumstances can result in a lack of security, affection, trust, aggressive behavior, low self-esteem, anxiety (Álvarez-Gallego, 2010; Levin & Liu, 2021), among other developmental, academic and behavioral issues. In other words, minors are affected both in personal and social development due to their low levels of self-esteem and poor management of emotions, which hinders their ability to solve problems and to adapt to the social environment (Rahmani & Ulu, 2021).
This pattern was not present in psychiatry services, which is interpreted as a greater ease of maintaining a more pragmatic type of care remotely. Nonetheless, further research is needed to demonstrate treatment-related effects, particularly considering designs based on clinical trials with control samples. For example, follow-up phases have demonstrated their value in assessing treatment efficacy for children living under vulnerable conditions across different types of treatments and training programs (Chapagain et al., 2023; Moiniafshari et al., 2022).
Several life conditions of children living in RCH pose a challenge for improving and optimizing well-being, mental health, and EI skills. Data suggest that the risk of mental health problems increases with the length of stay in the institution (Andreopoulou et al., 2020; Baptista et al., 2014; Chinn et al., 2021; Ginige et al., 2020; Holmes et al., 2018; Lionetti et al., 2015). Our results showed that delivery of EI intervention during critical periods of development can help to maintain EI skills and empathy. Institutionalized children face numerous challenges that can directly influence the outcomes of EI interventions. Among these factors, frequent caregiver turnover stands out, which generates a lack of continuity in affective relationships and hinders the establishment of a secure attachment (Sánchez-Reyes et al., 2019). The absence of a stable caregiver can lead to feelings of insecurity and distrust, which in turn impacts the development of skills such as empathy and emotional self-regulation. The absence of adequate social, emotional and cognitive stimuli, which are essential for the healthy development of children, is a recurrent problem in institutions where individualized attention is limited due to the high ratio of children per caregiver and the lack of adequate resources (Dorado Primo, 1990; UNICEF, 2024). Research such as Condor-Vela and Shuguli-Zambrano (2024)), and Yslado-Mendez et al. (2019) have shown that the quality of institutional care has a significant impact on EI levels in children and adolescents. These factors also affect the effectiveness of the programs designed to improve EI.
Despite these challenges, children can cultivate strategies enabling them to adapt effectively to demanding circumstances. They can foster protective factors, including practical management and life skills, independence, and the capacity to manage stress (Pacione et al., 2013). To enhance children's coexistence across their various environments, both inside and outside the home, it is essential to nurture their emotional capacities and skills (Guil et al., 2018), alongside other cognitive processes like attention, memory, and language, which are integral to social interaction. Moreover, socio-cognitive competencies such as problem-solving and behavioral planning, all of which are vital for integral child development (Saiz Manzanares & Roman Sánchez, 1996). The greater or lesser effectiveness in the use of cognitive-affective and behavioral resources that a child uses to resolve everyday situations of social interaction will depend on the perception of their own abilities to generate alternative solutions, regulate their emotions, consider the ramifications of each action, and finally, to make better decisions in everyday life. To put it differently, a child's capacity to generate solutions, control their emotions, and think about the consequences of their actions is crucial for success in social interactions.
The ability to properly manage emotions is fundamental, especially in conflict situations, as it enables children to respond more adaptively and avoid impulsive reactions. Considering that these skills develop in specific contexts, the question arises as to whether children who have experienced abandonment, abuse, and those with disruptive behaviors, coming from challenging developmental environments, use different strategies to resolve conflicts (Ison-Zintilini & Morelato-Giménez, 2008). Given this evidence, it is essential to develop intervention programs that strengthen emotional intelligence (EI) in these children. In this regard, intervention programs based on EI methods have shown good results in reducing adverse mental health outcomes. According to previous research, emotional intelligence in children's lives encompasses elementary aspects that intervene in a child's life, improving the way a child addresses and resolves problems, whether at school, at home, or in the social environment (Domínguez, 2013; Mesa Jacobo, 2015; Peralta Bazán & Sandoval Chimoy, 2016).
The significant role of EI lies in allowing children to acquire strategies and skills that permit them to recognize and express their own emotions and those of others, and to maintain satisfactory interpersonal relationships (Arias-Chávez et al., 2020; Peralta Bazán & Sandoval Chimoy, 2016; Peres Arenas, 2008; Pérez, 2007). Among the components mentioned by Bar-On’s mixed model to describe EI are benefits including successful adaptation to the environment, and prevention of negative behaviors such as aggressiveness or disruptive behaviors, stress, antisocial behaviors, depression, harmful behaviors, as well as negative emotions that can affect the integrity of children (Espinosa Gallardo, 2018; Pacheco y Fernández-Berrocal, 2013). Developing emotional skills in early stages of life works as a strategy that optimizes a child’s resources when dealing with adverse situations (Bisquerra Alzina, 2005).
On the other hand, social distancing measures implemented as prevention for the COVID-19 pandemic have transformed the dynamics of childhood, and it has been pointed out that one of its consequences is the increased vulnerability of this population to experiencing serious mental health problems (Gurwitch et al., 2020). Findings during the pandemic suggested that children and adolescents with anxiety, mood, or stress-related disorders experienced an intensification of symptoms, while those diagnosed with neurodevelopmental disorders showed increased symptomatology, both of which have been associated with changes in routines and household structure, as well as fear of contagion or the death of a close person (Joint Task Force for the Development of Telepsychology Guidelines for Psychologists, 2013).
These conditions prompted mental health professionals to adopt novel strategies to continue providing their services, leading to an increased prevalence of remote psychological intervention. The application of remote interventions is framed within the concept of "telehealth", which refers to the remote delivery of services related to mental health or physical health for assessment, prevention, and intervention (Krach et al., 2020). Concerning this, both the APA and the National Association of School Psychologist (NASP) have published some recommendations for the provision of distance psychological care services, noting that it is important to maintain the validity and reliability of procedures when adapting them to the virtual modality (Banks & Butcher, 2020; NASP, 2017). Corresponding to the increase in the implementation of remote psychological services, there is growing body of research aimed at verifying their efficacy; however, studies exploring childcare services are less common. Understanding the reliability, effectiveness, and self-reported aspects of childhood intervention is essential to evaluate and optimize the use of remote mental health services (Hoffnung et al., 2021).
Recent findings identify advantages associated with accessibility, given that a significant part of the population has electronic communication devices, reduced transportation times (especially in rural regions), and the inclusion of psychoeducation in treatments. Particularly within the young population, digital technologies have been highlighted as an attractive, inexpensive, accessible and clinically significant way to address mental health problems in children and adolescents (Markowitz et al., 2021; Reynard et al., 2022). Benefits achieved through the incorporation of programs involving EI training include increased the social skills and satisfactory interpersonal relationships, a reduction of self-destructive thoughts, and better self-esteem. Furthermore, the integration of such programs may lead to a decrease in rates of violence and aggression, less antisocial behavior, as well as enhanced academic performance. Other benefits described include a decrease in the initiation of alcohol, tobacco, and drug use, and a reduction in sadness and depressive symptoms (Garaigordobil Landazabal et al., 2018), alongside other issues such as anxiety and stress. However, currently there are only a few programs based on EI training, and the number is even more limited for home care populations.
The aforementioned highlights the importance of fostering strategies in children’s development and the creation and implementation of intervention programs, considering available resources under critical conditions and social isolation, as well as the lack of access or availability to mental health services. The objective of this study was to evaluate the effectiveness of a remotely administered intervention program based on emotional intelligence in children residing in RCHs under social isolation during the pandemic lockdown. The hypothesis considered was that EI skills may improve after the administration of a remotely administered intervention program in a group of children living in RCHs.
Methodology
Materials and Methods
Participants
Participants in this study were children aged between 7 and 11 years (four females, three males), with a mean age of 9 years old (SD = 1.41). All participants resided in a RCH located in a rural region of Mexico (Table 1). Due to ethical regulations from RCH services and institutions in Mexico, no further clinical background or family history details were provided.
Instruments and Materials
Evaluation of Neurological Soft Signs - ENSS - (Rosselli Cock et al., 2004). This instrument was administered to rule out the presence of neurological or sensory conditions that could impede basic psychological or sensory processes required for access to the assessment and intervention activities designed in the program. The evaluation consisted in delivering instructions to the child. Tasks consisted: gait (walking along a line on the floor), pencil grip, articulation (words repeating), visual acuity, right-left discrimination, dysdiadochokinesis (coordination of hand movements), and digital opposition movements. Auditory discrimination was not evaluated because of sensitivity problems associated with distance assessment; nevertheless, deficiencies in this sensory modality were ruled out by response to sound stimuli and the opinion of the caregiver.
To measure emotional intelligence, the Emotional Intelligence Questionnaire EQ-i by Reuven Bar-On (as cited in Davis & Wigelsworth, 2018) was used. It was translated into Spanish by Dolores Prieto and considers five components of emotional intelligence: intrapersonal component, interpersonal component, stress management component, adaptability and general mood (Prieto et al., 2008).
After each intervention, a Likert scale feedback questionnaire on the general well-being of the participants was conducted. It consisted of 5 questions related to subjective sensation of achievement of the session’s objective, sensation of wellbeing and mood, follow-up to the administered tasks, and attention.
Procedure
All procedures of the RA-EIBI were sequenced in three phases:
Phase I: Initial Diagnosis
A telephone link was made with one of the caregivers of the children’s home 15 minutes prior to the application to prepare the space and work materials for the child. Subsequently, a digital link was made with the child, and the applicator introduced himself briefly. A computer was provided to the RCH for communication with the participants. Following this, a digital link was stablished with the child, and the application of the EQ-i was given through Google Form. The application time was approximately 40 minutes. Throughout the assessment, the instructor requested the support of a caregiver to be available for any questions the child might have and to ensure attentiveness to the instructions.
Based on this first evaluation, the intervention program was designed with a greater focus on the intrapersonal, interpersonal, and stress management components of the Bar-On’s mixed model, where the lowest scores were obtained. This decision also took into account the breadth of the components and subcomponents that encompass emotional intelligence and the limited time available in the home for the application of the program.
The RA-EIBI program was designed considering the following EI domains based on Bar-On’s model:
-Intrapersonal component (IPC) - Area that brings together the following components:
Emotional self-understanding (CM): The ability to notice and understand our feelings and emotions differentiate them and know the reason for them.
Assertiveness (AS): The ability to express feelings, beliefs and thoughts without hurting the feelings of others and to defend our rights in a non-destructive manner.
Self-concept (SC): The ability to understand, accept, and respect oneself, accepting our positive and negative aspects, as well as our limitations and possibilities.
Self-Realization (SR): The ability to do what we can, what we really want, enjoying what we do.
Independence (IN): The ability to be self-directed, feeling self-confident in thought, actions, and being emotionally independent to make decisions.
- Interpersonal component (IC) - Area that brings together the following components:
Empathy (EM): The ability to notice, understand and appreciate the feelings of others.
Interpersonal relations (IR): The ability to establish and maintain mutually satisfying relationships that are characterized by emotional closeness and intimacy.
Social responsibility (SR): The ability to demonstrate oneself as a cooperative, contributing, and constructive member of the social group.
- Adaptability component (AC) - An area that brings together the following components:
Problem solving (PS): The ability to identify and define problems as well as to generate and implement effective solutions.
Reality testing (RT): The ability to evaluate the correspondence between what we experience (the subjective) and what exists in reality (the objective).
Flexibility (FL): The ability to make an appropriate adjustment of our emotions, thoughts and behaviors to changing situations and conditions.
- Stress management component (SMC) - An area that brings together the following components:
Stress tolerance (ET): The ability to withstand adverse events, stressful situations and strong emotions without "falling apart," actively and positively coping with stress.
Impulse control (IC): The ability to resist or delay an impulse or temptations to act and control our emotions.
- General mood component (GMC) - An area that brings together the following components:
Happiness (HA): The ability to feel satisfied with our life, to enjoy ourselves and others, and to have fun and express positive feelings.
Optimism (OP): The ability to see the brighter side of life and maintain a positive attitude, despite adversity and negative feelings.
Phase II. Intervention (see Appendix A for further details)
In this phase, the intervention program was applied remotely, with a total of 10 sessions per child over the course of three months, from March 19th to May 21st. Each individual session lasted approximately 40 minutes. The RCH designated a caregiver to help monitor the child during the session to verify and assist if necessary. Additionally, a quiet space, away from the rest of the children and free of distractions, was provided within the home. Prior to the sessions in this phase, resources and didactic materials were provided to the children, in order to enhance the efficiency of the program. Sessions were scheduled as shown in Table 2.
Table 2 Intervention Schedule
| Intervention session and objective | Date |
| Session 1. Introduction to intervention | March 19th-20th |
| Session 2. Emotional Identification | March 26th-27th |
| Session 3. Assertiveness | April 9-10th |
| Session 4. Self-concept (team-work session) | April 17th |
| Interpersonal Component | |
| Session 5. Empathy | April 23rd |
| Session 6. Interpersonal relations (team-work session) | May 7th-8th |
| Stress Management Component | |
| Session 7. Commend | May 14th-15th |
| Session 8-10. Impulse control | May 21th-22nd |
Phase III. Final Diagnosis
In this phase, a final evaluation of the EQ-i was conducted. This second administration allowed a comparison with the results of the initial and final diagnosis to determine if there was a favorable change in the emotional intelligence of the children at the children’s home once the intervention ended. A telephone call was made to one of the caregivers at the home minutes before the application. Then, a digital link was stablished with the child. The estimated time for this session was approximately 40 minutes per participant. The instructor also requested the support of a caregiver available for any questions the child might have and to ensure that the child remained attentive to the instructions.
Ethical considerations
Integral Family Development (DIF, due to its initials in Spanish) properly analyzed and approved the implemented protocol in children. Also, the assessment procedures and intervention project were sent to be evaluated by the Graduate Research and Ethics Committee of the faculty, which resolved to ethically validate the intervention project under registration number POSG/020-2-01. Preprint available at https://www.preprints.org/manuscript/202210.0033/v1
Data analysis
Descriptive statistics were performed to summarize the empathy coefficient measures. The Shapiro Wilk test for normality was utilized due to the sample size and measurement levels. The Wilcoxon nonparametric test for related samples was then employed, using the empathy coefficient measures as the dependent variable and pre and post treatment as the independent variable.
Results
Throughout the sessions, the children demonstrated good adaptability to the activities. Sessions were primarily delivered using Google Meets, and the caregiver regularly assisted the child if they encountered difficulties with the computer. The administration of the ENSS indicated adequate performance of soft neurological functions in children, ensuring appropriate access to the interaction necessary for the EQ-i evaluation and the RA-EIBI administration.
Thereafter, data gathered from Google Forms was captured and verified to ensure that the database values fell within the minimum and maximum parameters established for each indicator and that there were no data outside the predicted ranges. Afterwards, the normality of the variables was assessed using the Shapiro-Wilk test. The results of the normality test proved to be significant, indicating non-normal data; Therefore, non-parametric statistics were used, and the Wilcoxon signed-rank test for paired samples was chosen as the appropriate test to determine if the RA-EIBI demonstrated significant differences in emotional intelligence before and after its administration to children living in an RCH. The results of the Wilcoxon signed-rank test are presented in Table 3.
Table 3 Comparisons of EQI Scores Before and After Emotional Intelligence Treatment
| EI Domain | Pre Treatment | Post Treatment | |||
| Mean | SD | Mean | SD | p | |
| Intrapersonal | 2.38 | 0.525 | 2.43 | 0.659 | 0.833 |
| Interpersonal | 2.11 | 0.675 | 2.32 | 0.450 | 0.339 |
| Stress Management | 2.29 | 0.970 | 2.62 | 0.651 | 0.553 |
| Adaptability | 2.71 | 0.668 | 2.86 | 0.556 | 0.672 |
| Mood | 3.19 | 0.813 | 2.76 | 0.787 | 0.203 |
| EQ | 116.8 | 5.01 | 117.85 | 4.14 | 0.351 |
The results of the test showed no statistically significant differences in any of the emotional intelligence components between the pre- and post-intervention evaluations. Following this, we aimed to describe the overall level of emotional intelligence among children living in the RCH during the social isolation period. The overall average score on the EQ-i was 2.53 in the pre-test and 2.59 in the post-test, as detailed in Table 3. Given that the maximum response score is 4, these average scores suggest a moderate level of overall emotional intelligence at both time points.
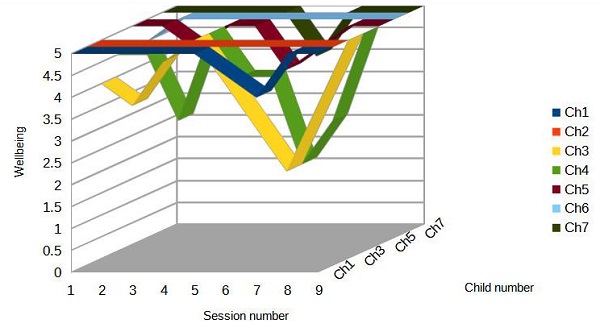
Self-reported well-being after each session follow-up revealed a particular decrease for five children in session number 7 (Figure 1), which took place on May 14th during a critical period of social isolation carried out in the institution. However, for all children, subjective well-being improved by the end of the program.
Discussion
Contrary to findings suggesting a potential decline in emotional intelligence during social isolation and in vulnerable populations (Rahmani & Ulu, 2021; Zhang et al., 2022), the results obtained from the statistical tests in our study with children living in residential care showed no significant differences between the pre- and post-intervention measures, suggesting that emotional intelligence remained relatively stable during the period of social isolation due to COVID-19. Hoffnung et al. (2021) also reported challenges in the delivery and impact of remote psychological services with children during the pandemic. Their analysis of data from 43, 294 services provided during the first six months of 2020 in New York found a significant decrease in child psychotherapy services and a rapid increase in face-to-face services when they resumed, suggesting that the distance modality is less preferred by children compared to adults. In this study, we were not able to compare the effectiveness of the online administered treatment with a face-to-face group, but we identified that the children had adequate access to interact in the assessment and intervention processes of this study.
This access is a relevant element, especially considering the institutional vulnerability conditions that usually limit the use of technological tools. The fact that children were able to consistently participate suggests that this type of remote intervention may be a viable option in contexts where in-person services are unavailable or limited. Online- administered programs have proven to be effective, safe, and low-cost (Boettcher et al., 2021; Bulik et al., 2012). Regarding the effectiveness in child populations, previous research suggests online interventions are promising in early stages of treatments, for example, in conditions where anxiety is present (Green et al., 2023). However, it must be considered that emotional intelligence is a complex and multidimensional skill that depends on sustained affective bonds and emotionally safe environments- factors that may be limited in institutional settings with high caregiver turnover.
From this perspective, the absence of statistically significant differences may not necessarily indicate a failure of the program but rather a potential sign of emotional stability in the midst of an adverse context. Moreover, maintaining emotional intelligence levels during a crisis period such as lockdown may represent a meaningful achievement, considering that several studies have documented setbacks in developmental areas during that time. Future research should explore in greater depth the influence if institutional factors that may be moderating intervention outcomes, such as caregiver involvement, emotional bond quality, or organizational structure of the residential care home.
Conclusions
The implementation of this remotely administered emotional intelligence intervention for children in RCH during pandemic-related social isolation presented several challenges, as noted in previous sections. While interventions based on emotional intelligence hold promise for the development and mental health of children in residential care, our study, which aimed to evaluate the effectiveness of such a program delivered remotely, found no significant improvement in emotional intelligence skills. This suggests that a general emotional intelligence intervention, particularly when administered remotely and during a period of significant stress, may not be sufficient to equip children with the specific coping mechanisms that are necessary to address their complex needs arising from their family backgrounds and experiences of abuse or neglect.
Future research should consider a more integrated approach, evaluating not only EI, but also cognitive aspects in this population, recognizing that children in RCH may present unique developmental conditions due to their experiences. And it is vital to incorporate control groups to assess the true effectiveness of interventions in this context. It would also be pertinent to analyze the differential effect of each EI component targeted in the program to determine which areas show greater sensitivity to change.
Taking into account the central role of caregivers, subsequent research could explore the inclusion of caregivers in the program to enhance modeling and support for the development of emotional intelligence skills. Regardless of the aforementioned challenges, there is a clear need for interventions or actions that promote the development of emotional intelligence.
Addressing the challenges of institutionalized care is crucial. Initiatives focused on empowering caregivers and raising the quality of care can maximize their benefits and support children's emotional development. The literature consistently highlights their fundamental role in the emotional and psychological development of the children under their care. Through a systematic review, Hermenau et al. (2017) evidenced that structured interventions and caregiver training positively affect emotional, social, and cognitive development and improve the child-caregiver relationship.
Due to the difficulties of confinement, studies based on larger samples or control groups, especially in highly vulnerable populations, are extremely complicated. Therefore, one of the limitations of this study was the lack of a control group to strengthen the possible attributions of treatment effect expressed. In addition, research in children is considered of high risk, due to the protection of their rights, the regulations to study the effects of interventions in this population have robust ethical and legal considerations, which are very good to protect them, but at the same time limits the access to enhance sample size in conditions such as those of this study.
Finally, it is essential to tailor interventions to the specific and complex needs of children in institutionalized settings. This implies designing strategies that consider not only emotional intelligence, but also factors related to trauma, attachment and behavioral regulation, and psychological processing, such as attention, memory, executive functioning, and verbal reasoning. Based in this comprehensive perspective, a promising line of research can emerge, contributing to improving the quality of life and emotional well-being of an especially vulnerable population.

