Clinical cases
Renal mucosa-associated lymphoid tissue lymphoma: a case report and
literature review
Linfoma de tejido linfoide asociado a mucosa renal: reporte de un
caso y revisión de la literatura
Andrés Felipe Córdoba, Conception, design, Supervision, Data collection, Writing1
 http://orcid.org/0000-0003-1019-5473
http://orcid.org/0000-0003-1019-5473
Roberto Franco Villalba-Bachur, Data collection, Analysis and interpretation, Literature review1
*
http://orcid.org/0000-0002-4488-3568
Juan Camean, Analysis and interpretation, Literature review1
http://orcid.org/0000-0002-4100-5743
Joaquín Chemi, Analysis and interpretation, Literature review1
http://orcid.org/0000-0003-1826-5114
Jorge Jaunarena, Supervision, Writing1
http://orcid.org/0000-0003-3059-2097
Cecilia Foncuberta, Conception, design, Critical review1
http://orcid.org/0000-0003-0028-6558
Gustavo Villoldo, Conception, design, Critical review1
http://orcid.org/0000-0003-1119-5336
1Instituto Alexander Fleming, Buenos Aires,
Argentina.
Abstract
Background:
Renal MALT lymphoma is a rare entity with few reports in the literature.
These neoplasms arise at extranodal sites, usually related with chronic
inflammation due to infection or autoimmune disorder and share histologic
and immunophenotypic features. To date, 10 cases of renal MALT lymphoma have
been described.
Case presentation:
We present a case of a MALT renal lymphoma in a 69-year-old woman with
suspected preoperative diagnosis of renal cell carcinoma (papillary vs
chromophobe type), RENAL SCORE 9p. We performed a retroperitoneal
laparoscopic left partial nephrectomy guided by intraoperative
ultrasound.
Conclusion:
There are few reports in the literature regarding renal MALT lymphoma. We
consider that this might be considered as a differential diagnosis of renal
mass.
Keywords: Renal lymphoma; mucosa-associated lymphoid tissue (MALT); nephrectomy
Resumen
Antecedentes:
El linfoma MALT renal es una entidad rara con pocos reportes en la
literatura. Estas neoplasias surgen en sitios extraganglionares,
generalmente relacionadas con inflamación crónica debida a infección o
trastorno autoinmunitario, y comparten características histológicas e
inmunofenotípicas. Hasta la fecha se han descrito 10 casos de linfoma MALT
renal.
Presentación del caso:
Presentamos un caso de linfoma renal MALT en una mujer de 69 años con
sospecha de diagnóstico preoperatorio de carcinoma de células renales (tipo
papilar vs cromófobo), RENAL SCORE 9p. Se realizó nefrectomía parcial
izquierda laparoscópica retroperitoneal guiada por ecografía
intraoperatoria.
Conclusión:
Existen pocos informes en la literatura sobre el linfoma MALT renal.
Consideramos que esto podría plantearse como diagnóstico diferencial de masa
renal.
Palabras clave: Linfoma renal; tejido linfoide asociado a mucosas (MALT); nefrectomía
Background
Mucosa-associated lymphoid tissue low-grade B-cell lymphoma (MALT), first described
by Isaacson and Wright in 1983,1 is
recognized as a distinct subtype in the non-Hodgkin lymphoma classification and is a
different group from B-cell lymphomas specified in the World Health Organization
(WHO) classification.1,2 Renal involvement represents less than 1% of prevalence of
MALT lymphomas.3-6
Pelstring et al. reported the first case of renal MALT lymphoma in 1991 and Colovic
first described primary renal MALT lymphoma in 1999.7 They are one of the less aggressive lymphomas and often
present as an indolent, localized disease and the treatment of these cases was
heterogeneous, from surgical, chemotherapy, immunotherapy, to radiotherapy.7,8
Clinically, patients with renal lymphoma are usually asymptomatic or may refer
nonspecific symptoms such as low back pain and/or haematuria. Diverse radiographic
presentations have been reported, including single or multiple retroperitoneal
masses and, in some cases, hydronephrosis or diffuse nephromegaly.9
Case Presentation
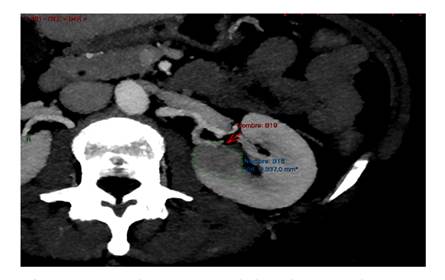
69-year-old woman with a history of IA endometrial cancer treated with
adnexa-hysterectomy in March 2021. In a follow up CT scan a completely endophytic
hypo-vascular tumor on the left kidney was evidenced, poorly delimited at the level
of the upper polar line, approximately 30 mm in the axial plane, suggesting a
papillary or chromophobe tumor. RENAL SCORE: 1+3+3+p+2=9p (Figure 1).
A retroperitoneal laparoscopic left partial nephrectomy with intraoperative
ultrasound guidance was performed.
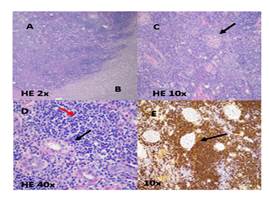
Pathological report showed microscopically alteration of the histoarchitecture, whith
lymphoid proliferation that infiltrates adipose tissue and whose intraparenchymal
borders are delimited from the preserved renal parenchyma. This lymphoid
proliferation replaces some glomerular and ductal structures, leaving others
preserved. Morphologically, no clear epithelial infiltration was observed. The cell
population was predominantly made up of small lymphoid cells, some plasma cells, and
very few and isolated large cells. There were few and isolated lymphoid follicles
with reactive-appearing germinal centers.
Immunohistochemistry (IHC) was positive for: (Figure 2:
A, B, C, D, E). CD20, CD3, CD5, CD23; cytokeratin’s: bcl-2, MIB-1. and
negative for: CD10, bcl-6. Labeling CD138, Kappa light chains and Lambda light
chains was also observed: indicating of isolated plasma cells remains. The final
diagnosis was renal MALT type lymphoma.
The staging with PET CT, bone marrow biopsy and flow cytometry did not show distant
disease.
Considered as primary renal MALT type lymphoma stage IE, no further treatment was
indicated and the patient remains disease free in the follow up.
Discussion
In 2020 the French LyKID study published the largest non-autopsy lymphoma series with
renal involvement, out of 87 cases only five were MALT type.10
MALT lymphomas can affect several anatomical sites and the appearance is usually
preceded by an inflammatory process, mainly observed in the gastrointestinal tract,
respiratory system, salivary glands, head and neck, thyroid, breast, gallbladder,
cervix, and ocular adnexa.3-5,7-9,11,12
The etiology of renal MALT lymphoma is not well established. However, repetitive
injury to renal lymphatics due to a chronic inflammatory process, such as chronic
pyelonephritis, usually precedes the onset of the disease. Usually debut as a
localized disease with slow clinical progression. However, transformation to
high-grade in the late course of the disease was reported in 8% of the
patients.5,13
Radiographic presentations may vary, as well as their clinical presentation.14 There are no differences in terms
of imaging diagnosis since it debuts as a renal mass. The role of PET- FDG
(18F-fluorodeoxyglucose positron emission tomography computed tomography) in this
scenario remains debatable due to the low avidity of MALT lymphoma extranodal
lesions, and their tendency to be located in tissues with physiologic
[18F]FDG-uptake can make image interpretation difficult.15
In case of nodal and extranodal involvement, a diagnostic percutaneous biopsy can be
considered to carry out systemic treatment. In our case it was not necessary since
it was a single presentation in the kidney.
The prognosis for patients with renal MALT lymphoma is good with chemotherapy,
surgical intervention, or radiation. The 5-year overall survival for MALT lymphoma
in the genitourinary tract is 75.6 %, even though for those with different
anatomical origins ranges from 69.1 to 87.9 % .10
Chemotherapy takes place when there is a multicentric or systemic involvement. In the
literature, most patients diagnosed with B-cell lymphoma underwent cytotoxic
chemotherapy with rituximab and intratecal methotrexate. Patients with MALT
lymphomas have better prognosis compared with those with high grade lymphomas.12
In most cases, the diagnosis is made after nephrectomy, generally due to suspicion of
another oncological lineage, and most of these patients do not require additional
treatment.
Conclusions
This is a rare disease and should be considered as a differential diagnosis in the
case of an atypical renal mass. Early diagnosis and timely treatment have positive
results.
References
1 Isaacson P, Wright DH. Malignant lymphoma of
mucosa-associated lymphoid tissue. A distinctive type of B-cell lymphoma.
Cancer. 1983;52(8):1410-6. doi:
https://doi.org/10.1002/1097-0142(19831015)52:8<1410::AID-CNCR2820520813>3.0.CO;2-3
[ Links ]
2 Thun EM, Linet MS, Cerhan JR, Haiman CA, Schottenfeld and D,
editors. Cancer Epidemiology and Prevention. 4th ed. Oxford, New
York: Oxford University Press; 2017. 1330p.
[ Links ]
3 Okuno SH, Hoyer JD, Ristow K, Witzig TE. Primary
renal non-Hodgkin’s lymphoma. An unusual extranodal site. Cancer.
1995;75(9):2258-61. doi:
https://doi.org/10.1002/1097-0142(19950501)75:9<2258::AID-CNCR2820750911>3.0.CO;2-
[ Links ]
4 Makino T, Miwa S, Koshida K, Kawashima A.
Mucosa-associated lymphoid tissue lymphoma involving the kidney: a case report
and review of the literature. Int Cancer Conf J. 2015;5(2):82-9. doi:
https://doi.org/10.1007/s13691-015-0234-6
[ Links ]
5 Gromicho A, Araújo D, Oliveira V, Ribeiro A, Ferraz
L. Mucosa-Associated Lymphoid Tissue Lymphoma Involving the Kidney
and Renal Pelvis. Cureus. 2021;13(5):e15172. doi:
https://doi.org/10.7759/cureus.15172
[ Links ]
6 Cavalli F, Isaacson PG, Gascoyne RD, Zucca E. MALT
Lymphomas. Hematology. 2001;2001(1):241-58. doi:
https://doi.org/10.1182/asheducation-2001.1.241
[ Links ]
7 Otsuki H, Ito K, Sato K, Kosaka T, Shimazaki H, Kaji T, et
al. Malignant lymphoma of mucosa-associated lymphoid tissue involving
the renal pelvis and the entire ureter: A case report. Oncol Lett. 2013
May;5(5):1625-8. doi: https://doi.org/10.3892/ol.2013.1221
[ Links ]
8 Polani FS, Zaidi F, Polani FS, Zaidi F. Renal
Mucosa-Associated Lymphoid Tissue (MALT) Associated End-Stage Renal Disease in a
Patient Presenting With Diarrhea. Cureus. 2021;13(7). Doi:
https://doi.org/10.7759/cureus.16158
[ Links ]
9 Olszewski AJ, Castillo JJ. Survival of patients with
marginal zone lymphoma: analysis of the Surveillance, Epidemiology, and End
Results database. Cancer. 2013;119(3):629-38. doi:
https://doi.org/10.1002/cncr.27773
[ Links ]
10 Garcia M, Konoplev S, Morosan C, Abruzzo LV, Bueso-Ramos
CE, Medeiros LJ. MALT lymphoma involving the kidney: a report of 10
cases and review of the literature. Am J Clin Pathol. 2007;128(3):464-73. doi:
https://doi.org/10.1309/0t2ukukv91w3qr6w
[ Links ]
11 Kohn M, Karras A, Zaidan M, Bénière C, de Fréminville J-B,
Laribi K, et al. Lymphomas with kidney involvement: the French
multicenter retrospective LyKID study. Leuk Lymphoma. 2020;61(4):887-95. doi:
https://doi.org/10.1080/10428194.2019.1697811
[ Links ]
12 Vannata B, Stathis A, Zucca E. Management of the
marginal zone lymphomas. Cancer Treat Res. 2015;165:227-49. doi:
https://doi.org/10.1007/978-3-319-13150-4_9
[ Links ]
13 Urban BA, Fishman EK. Renal lymphoma: CT patterns
with emphasis on helical CT. Radiographics. 2000;20(1):197-212. doi:
https://doi.org/10.1148/radiographics.20.1.g00ja09197
[ Links ]
14 Cohen D, Perry C, Hazut-Krauthammer S, Kesler M, Herishanu
Y, Luttwak E, et al. Is There a Role for [18F]FDG PET-CT in Staging
MALT Lymphoma? Cancers(Basel). 2022;14(3):750. doi:
https://doi.org/10.3390/cancers14030750
[ Links ]
15 Asgari SA, Aval HB, Asgari SA, Kheradmand K. A
unique case of kidney’s collecting system MALT lymphoma. Can Urol Assoc J.
2014;8(3-4):E172-175. doi: https://doi.org/10.5489/cuaj.1452
[ Links ]












 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink