











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
The COVID-19 disease caused by SARS-CoV-2 became a global pandemic, spreading to Mexico and leading to social isolation (Parmet & Sinha, 2020; World Health Organization, 2020a). This isolation brought with it potential psychological repercussions, elevating risks of depression, declines in well-being, and even mortality (Pollard et al., 2020; Yanai, 2020). The effects on the youth, however, remain under exploration, particularly when compounded with the stressors of transitioning to adulthood (Copeland et al., 2021).
Before the pandemic, the health of the youth population was affected by lifestyle modifications such as increased overeating and consumption of ultra-processed foods, alcohol, and tobacco, as well as the change in eating patterns (Akseer et al., 2017; De Mier et al., 2017, Concha et al., 2019). It’s notable that southern Mexico has a peculiar diet pattern, consuming more fruits yet fewer legumes, eggs, and dairy. Alarmingly, the region also has a higher consumption of sugary beverages, a recognized factor for obesity and metabolic syndromes across various age groups (Rodríguez-Ramírez et al., 2020; Hernández-Cordero et al., 2014).
In Mexico, the prevalence of obesity (34.1%) increased in people between 20 and 29 years of age, in addition to diabetes (10.3%) and hypertension (18.4%), according to the National Survey of Health and Nutrition (ENSANUT, 2018). These conditions, in combination, significantly amplify COVID-19 mortality rates (Correa et al., 2022). Moreover, the imposed isolation saw an 18.9% surge in depression among Mexican youths (Emigdio-Vargas et al., 2021).
On the other hand, the relationship between dietary patterns and health outcomes is well-established. Consuming non-recommended foods, which offer low nutritional value, alongside alcohol intake and a sedentary lifestyle, especially when combined with genetic predispositions, elevates the risk of chronic diseases and subsequent complications in adulthood (Begdache et al., 2017). Diets rich in saturated fats and sugars pave the way for metabolic disruptions, manifesting in conditions like obesity and neuroinflammation. Further, an elevated body mass index (BMI) poses risks, making one more susceptible to cardiovascular and renal diseases, diabetes, and various cancers (Chu et al., 2018; GBD 2015 Obesity Collaborators, 2017).
Ensuring physical and mental well-being is fundamental to enhancing the quality of life across all life stages. Physical activity is essential to prevent chronic degenerative diseases and is defined as any bodily movement that requires energy expenditure and includes daily activities such as work, play, household tasks and recreational activities (Akseer et al., 2017). Likewise, depression would increase due to coexisting metabolic deficiencies (Fulton et al., 2022). These disorders generate structural and functional changes in the brain, similar to depression, such as region-specific increases in cell density and neuronal connectivity (Fulton et al., 2022). Therefore, adopting a holistic approach to wellness encompassing a balanced diet that curbs the intake of foods rich in saturated fats, sugars, and salt, and encourages consumption of natural foods, paired with consistent physical activity becomes imperative. Such a lifestyle is particularly crucial for younger populations, safeguarding their physical and mental health against both intrinsic (genetic) and extrinsic (lifestyle-related) risk factors (Begdache et al., 2017, 2020; Bruins et al., 2019; Budreviciute et al., 2020).
The pandemic has particularly magnified pre-existing disparities in health, education, and income among southeastern Mexico’s population (García et al., 2020). Even before the pandemic, the population in this region showcased concerning dietary patterns, marked notably by a pronounced intake of sugar-sweetened beverages (Rodríguez-Ramírez et al., 2020). In addition, young individuals in this region have significant mental health challenges, predominantly anxiety and depression (Castillo et al., 2019). However, the impact of the pandemic, when viewed in tandem with factors like diet, physical activity, and familial health histories, on southeastern youth remains rather ambiguous. Therefore, the research assessed the dietary habits, physical activity, as well family history and examined the potential implications for the health of youths from southeastern Mexico within the context of the quarantine imposed due to the COVID-19 pandemic.
Methods
Study population
A cross-sectional study using a simple random sample, included 277 participants between 15 and 35 years (20.7±2.4) who confirmed that they lived in the southeast of Mexico, in the states of Yucatan, Campeche, and Quintana Roo. For this study, we define the youth population as between 15 and 35. The rationale for the age range is that individuals have not yet commonly experienced the effects of hormonal decline, immune response, or organ dysfunction associated with chronic degenerative health conditions (Fidler et al., 2017).
Instruments
An online questionnaire designed to collect general data using the Microsoft Forms application. The questionnaire was distributed by e-mail, with the support of the School Control Department of the Faculty of Chemical Engineering of the Autonomous University of Yucatan, from December 2020 to October 2021. The questionnaire considered the following: age, gender, weight, height, waist, dietary patterns (considered the types of food consumed; they were classified into recommended [RF] and non-recommended [NRF] foods); (Rodríguez-Ramírez et al., 2020). Also, as the frequency of weekly consumption at each mealtime (breakfast, lunch, dinner, and snack), physical activity, hereditary-family history, and health status (included an item on the feeling of depression). The BMI was calculated as weight in kilograms divided by the square of his height in meters (kg/m2), and the results were classified into four categories according to the World Health Organization (2021). Undernutrition <18.5; normo-weight 18.6-24.9; overweight 25.0-29.9; obesity class I 30-34.9; obesity class II ≥35. Participants who gave informed consent completed the online survey, which followed the principles outlined in the Declaration of Helsinki. They were also offered the possibility of revoking this consent at any time. They were informed that participation in the study was voluntary and that their data’s anonymity and confidentiality would always be guaranteed.
Data analysis
Statistical analysis was performed on media, standard deviation for continuous variables and percentage for discrete variables. Multivariate analysis for obesity was presented using the odds ratio [OR (confidence interval) p value] to clinical and heredo-familial characteristics, alimentary groups, and symptoms of depression, adjusted for gender, age, and BMI by Pearson coefficient, using STATA 13-SE statistical package with a 95% confidence interval and a significance level of p < .05 (StataCorp, 2013).
Results
Anthropometry, health status and familiar history
In the cohort comprising 277 participants for the research study, 153 were females, constituting 55.2% of the sample, whereas 124 were males, representing 44.7%. A higher participation was observed among 15- to 24-year-olds (266 respondents) compared to the 26- to 35-year-old group (11 respondents). Due to the age range of the participants, an analysis of the continuous variables between the age mentioned above groups was performed. The average waist of the participants was 80.3±15 cm. The weight range varied between 50 to 82 kg (women) and 58 to 87 kg (men). The mean BMI was 24.7±4.1 and 41.9% of the total population had a BMI ≥ 25. It is important to note that the students provided their measurements after following the instructions on the correct way to measure.
In the health of the youth population, symptoms of depression (24.2%) were reported to be the second most frequent negative health effects after obesity (41.9%). The 9.3% of participants reported having been infected with COVID-19 before or during questionnaire application. Chronic diseases such as hypertension (1.1%) were reported to a lesser extent, and no cases of diabetes were reported. Ninety-one percent reported at least one person with chronic degenerative diseases in their family. Family history of diabetes was the most frequently reported disease with 77%, followed by hypertension (66.38%) and obesity (62.5%).
Diet and physical activity in the youth population in Southeastern Mexico
Concerning eating habits in the young population of southeastern Mexico, the lunch (99%) was most frequently eaten, as well as breakfast and dinner to a lesser extent in more the respondents. Snacking (55%) was the feeding time with the lowest frequency. During breakfast, fruits and vegetables (82.5%), as well as legumes and animal foods (98.2%), were consumed most frequently during lunch, and cereals (76.9%). At dinner, fruits and vegetables were consumed less frequently (46.7%), and at lunch, it was cereals (60%). The perception of breakfast (64%), lunch (68%), and snack (58%) were “regular” (neither adequate nor inadequate). However, the perception of food at dinner (56%) was inadequate (Table 1).
Table 1 Food consumption patterns and perceptions among southeastern Mexican youth during COVID-19 quarantine
| Mealtimes | Breakfast (%) | Lunch (%) | Dinner (%) | Snack (%) |
| 86 | 99 | 88 | 55 | |
| Food group included in the meal Fruits and vegetables | 58 | 82.5 | 46.7 | ND |
| Cereals | 76.9 | 60 | 76.2 | ND |
| Legumes and foods of animal origin | 80.3 | 98.2 | 63.5 | ND |
| Perception of the quality of the food consumed | ||||
| Adequate | 23 | 25 | 14 | 15 |
| Regular | 64 | 68 | 30 | 58 |
| Inadequate | 13 | 8 | 56 | 27 |
Figure 1 shows the RF and NRF consumed mainly by the youth during different mealtimes. In all mealtimes, water was the most consumed RF (> 1 day), mainly during snacks (97.4%). Additionally, the most consumed RF (> 1 day) during breakfast were home-cooked food (95.4%) and fruits (92%); at lunch, home-cooked food (98.9%) and legumes (98.2%); home-cooked food (84%) and dairy (79.1%) at dinner; and snack, fruits (90.1%) and dairy (45.7%). At breakfast, sandwiches (79%) and cookies (75.6%); sauces/dressings (73.8%) and fast food (61.1%) at lunch; at dinner, fast food (84.4%) and sandwiches (78.7%); and, at snack sweets/desserts (68.9%), and cookies (63.9%) were the most consumed NRF (> 1 day).
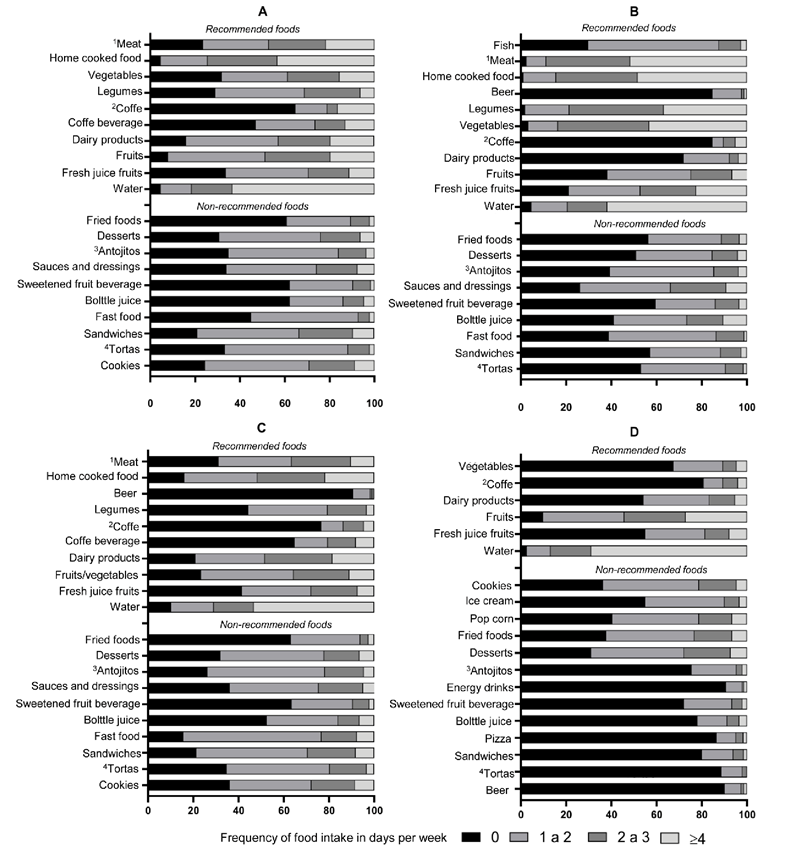
Figure 1 Foods consumed by youth in southeastern Mexico in days per week during the COVID-19 quarantine. A: breakfast; B: lunch; C: dinner; D: snack.
The home-cooked food was consumed > 4 times per week during breakfast (43.3%), lunch (48.8%), and dinner (21.7%). During breakfast, it was sandwiches/ bagels (9.7%), at lunch bottled soft drinks (10.5%), and cookies (8.5%) at dinner, the most consumed NRF > 4 days. At snack, fruits (27.1%) and sweets/desserts (7.3%) were the most consumed RF and NRF (> 4 days), respectively. Juice and soft drinks (62.2%) at breakfast and beer at lunch (84.7%) and dinner (90.6%) were the NRF most mentioned not to consume. Most respondents did not prefer coffee (RF) at any mealtime.
Physical activity was reported by 65.64% of the respondents. The 29.22% indicated doing it 1-2 times per week; only 13.31% indicated practicing physical activity > 4 times per week. 34.36% of the respondents did not engage in physical activity. The highest percentage (30.36%) engaged in physical activity between 30 and 60 min. The main reason was health (35%), followed by physical appearance (16.91%).
Risk factors associated with major chronic diseases
The main risk factors associated with the respondents’ health during the COVID-19 pandemic are presented below. Table 2 shows the association analysis shows that BMI would increase the risk of obesity up to 8.0 (4.51 - 14.47) times (p < .0001). This risk would increase mainly in men up to 2.1 (1.02 - 4.60) times (p < .05). Another important factor for obesity is the consumption of food during dinner [OR 1.2 (.35 - 4.46) .01]. Table 3 shows that obesity would be associated mainly with NRF consumption during dinner [OR 2.4 (1.48 - 12.70) .02], as well as at lunch [OR 2.7 (1.72 - 10.60) .01] and snack [OR 1.7 (1.65 - 4.79) .02]. Thus, NRF, mainly during dinner and snacks, is strongly associated with symptoms of depression [OR 7.6 (1.19-43.03) .06] and [OR 2.6 (0.42-16.91) .02].
Table 2 Association between obesity and clinical characteristics of youth during quarantine
| Obesity | OR (IC) p | p -value |
| Age | .9 (.78 - 1.08) | .3 |
| Sex | 2.1 (1.02 - 4.60) | .04* |
| BMI | 8.0 (4.51 - 14.47) | .0001* |
| Breakfast | 1.4 (.49 - 4.13) | .5 |
| Lunch | .2 (.003 - 21.70) | .5 |
| Dinner | 1.2 (.35 - 4.46) | .01* |
| Snack | 1.3 (.68 - 2.55) | .03* |
| Physical activity | .9 (0.44 - 1.99) | .8 |
| Time of physical activity | .7 (0.49 - 1.25) | .3 |
Note: Data are presented as odds ratio (95% CI). Statistical significance was calculated using Pearson Chi2 analysis Adjusted for sex, BMI, waist, and physical activity with a value of * p < .05; CI-95%. OR: odds ratio.
Table 3 Association between obesity and symptoms of depression with food groups
| Food group | Obesity | Symptoms of depression | ||
| OR (IC) p | p- value | OR (IC) p | p- value | |
| Recommended foods Breakfast | .42 (.11-1.62) | .2 | .3 (.087-1.74) | .2 |
| Lunch | .16 (.02-1.06) | .5 | 1.4 (.14-15.81) | .7 |
| Dinner | .95 (.19-4.53) | .9 | 1.6 (.02-0.99) | .04 |
| Snack | .60 (.11-3.08) | .5 | .9 (.28-3.37) | .9 |
| Non recommended foods Breakfast | 1.4 (1.28-7.97) | .06 | 0.9 (.10-9.15) | .9 |
| Lunch | 2.7 (1.72-10.60) | .01* | 1.3 (.13-12.96) | .8 |
| Dinner | 2.4 (1.48-12.70) | .02* | 7.6 (1.19-43.03) | .06 |
| Snack | 1.7 (1.65-4.79) | .02* | 2.6 (.42-16.91) | .02* |
Note: Data are presented as odds ratio (95% CI). Statistical significance was calculated using Pearson Chi2 analysis Adjusted for sex, BMI, waist, and physical activity with a value of * p < .05; CI-95%. OR: odds ratio.
Obesity would increase up to 11.1 (3.7-33) times if a times (p < .0001). In contrast, a history of hypertenfamily member had the same condition, a significant sion was not shown to be associated with the disease. risk (p < .0001); (Table 4). Meanwhile, a family history On the other hand, obesity would increase up to 2.3 of diabetes would increase the risk up to 3.3 (2.4-4.5) (1.05-5.01) symptoms of depression (p < .05).
Table 4 Association between obesity and familial history of southeastern Mexican youth
| Obesity | OR (IC) p | p- value | Adjusted OR (IC) p | p- value |
| FH obesity | 11.1 (3.7-33.0) | .0001* | 17.0 (4.4-64.7) | .001* |
| FH diabetes | 3.3 (2.4-4.5) | .0001* | 1.4 (1.0-5.1) | .0001* |
| FH hypertension | 1.1 (0.62-2.2) | .6 | 2.2 (1.01-5.12) | .04* |
| FH symptoms of Depression | 1.8 (0.95-3.52) | .06 | 2.3 (1.05-5.01) | .03* |
Note: Data are presented as odds ratio (95% CI). Statistical significance was calculated using Pearson Chi2 analysis Adjusted for sex, BMI, waist, and physical activity with a value of * p < .05; CI-95%. OR: odds ratio.
Discussion
In the population of southeastern Mexico, pre-existing inequalities in health, education, and economic income have been observed and increased during the COVID-19 pandemic (García et al., 2020). For this reason, local governments have been urged to take action to stabilize human development indices, including health and well-being (García et al., 2020). Before the pandemic, obesity (34.1%) was high in Mexicans between 20 and 29 years of age. In this study, a larger population with obesity (41.9%) was reported, similar to the prevalence reported in the adult population of the southern region of Mexico (41.5%) (Barquera et al., 2020). The obesity is a disease that precedes the development of other more severe diseases, such as diabetes and hypertension. The latter, together with obesity, are comorbidities that increase the risk of death from COVID-19 by up to 54.1% (Correa et al., 2022).
In the country’s south, the indicators of interest have focused on mental health, specifically depression. In the last decade, attention has been paid to mental health, mainly in the young population, due to the increase in cases of attempted suicide, which has become a severe public health problem that demands timely intervention from other government sectors, in addition to the health sector (ENSANUT, 2018). One of the most affected groups is the youth population in the southeastern of Mexico, where prevalence reaches up to 20.2% (Castillo et al., 2019). The youth group (19-30 years old) presented six symptoms, the highest being: scared easily (34.9%), feeling nervous, tense, or worried (30.2%) and difficulty thinking clearly and feeling depressed (28.6%) (Castillo et al., 2019). In this study we found similar prevalence of feeling depressed (24.2%). Also, during isolation, Emigdio-Vargas et al. (2021) found a prevalence of 18.9% on depression symptoms measured using a scale in people < 40 years old in southeastern of Mexico. In the face of this health problem (physical and mental), diet and physical activity could influence health when they are included in a healthy lifestyle (Begdache & Patrissy, 2021).
The youth population commonly assumes responsibility for their diet. Several aspects could influence the schedules and eating patterns, which play a role in establishing new dietary habits. Before the pandemic, the diet of the youth population was unhealthy, and mealtimes were consistently irregular (Akseer et al., 2017; De Mier et al., 2017). In this regard, lunch was the mealtime (99%) most performed, followed by breakfast (84.6%) and dinner (80%) in a youth population of both genders aged 18 to 30 years (Concha et al., 2019). In contrast to the results of this work, a similarity was found with the frequency of performing lunch (99%) and breakfast (86%). However, the frequency of eating dinner was higher (88%).
Eating breakfast and lunch before 5:00 pm could reduce the development of overweight and obesity. On the contrary, consuming more than 33% of the daily food intake at dinner could increase the risk of overweight and obesity (Wang et al., 2014). Additionally, meal composition is associated with a better nutritional status, mainly during breakfast. Higher consumption of carbohydrates and proteins at breakfast is related to a lower BMI (Sievert et al., 2019). Conversely, a higher intake of fat and lower amounts of fiber at breakfast may increase BMI. Regardless of caloric intake, late-night dining could increase the risk of developing obesity and diabetes (Nimitphong et al., 2018). In this study, it was observed that young people of southeastern chose to dine on inadequate foods, representing a high intake of calories, mainly during dinner. This fact would be contributing to a higher risk of developing obesity.
Before the pandemic, the diet of the youth population was characterized by an increase in fast food and other foods prepared outside the home, immersed in an “obesogenic food environment” (Allman-Farinelli, 2015). The results of this study show an increase in home-cooked meals. In addition, at least once a week, lower consumption of alcohol (9.4%) at dinner and fruit (90.1%) at snack was observed. According to reports from ENSANUT (2018), 35.5% of those over 20 years of age are excessive alcohol consumers, Yucatan, with the population with the highest consumption (45.8%) annually between 12 and 65 years of age (Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco, 2017). In addition, the southern region has the lowest consumption of fruits and vegetables. Thus, the changes observed in the diet of the study population were positive due to social isolation. López-Moreno et al. (2023) reported that 50% of the adolescents during the pandemic mentioned that they improved their diet, possibly because most of them ate at home. Therefore, it is possible that the positive changes observed in this study are also related to eating food prepared at home due to social isolation.
Physical activity is part of a healthy lifestyle and can produce long-term benefits. It is advisable to perform at least 60 minutes of moderate to vigorous physical activity daily; more time is needed in young people (WHO, 2020b). In this context, only 11.52% of respondents complied with this recommendation during the pandemic. Before the pandemic, 14.32% of the population in Mexico between 20 and 29 years of age was considered inactive, and 74.4% performed physical activity ≤ 150 minutes (ENSANUT, 2018). The data indicated a decrease in physical activity in the population, compared to the national average during the pre-pandemic period, since 34.36% did not perform physical activity during the week. This trend indicates a need to implement strategies that promote increased physical activity in the youth population because a sedentary lifestyle would generate health consequences in the short and long term (Akseer et al., 2017)
A therapeutic alternative to treat obesity and symptoms of depression could be implementing a calorie-restricted diet (low sugar and/or low fat). This dietary intervention could reduce depression by 0.2 to 0.6-fold (Patsalos et al., 2021). Likewise, a dietary therapeutic strategy should include a physical activity program; it has been demonstrated that mental health in obesity improves self-efficacy and autonomous motivation (Carraça et al., 2021).
Identifying the risk factors associated with the health of the southeastern Mexico youth population would help design pro-health and wellness strategies. The results of this work contribute to the importance of preventing obesity; symptoms of depression rates could decrease. Thus, promoting healthy foods, mainly during dinner and snacks, as well as physical activity, would improve the quality of life of the population between 15 and 35 years of age in southeastern Mexico.
Among the study’s limitations is the use of an online questionnaire, which could mean a bias in the participation of people who need access to the internet or digital devices. Those above could limit the study’s representation of the broader youth population in southeastern Mexico. Moreover, participants’ self-measurement data may need to be more reliable due to measurement errors or the tendency of some respondents to give socially desirable answers. Despite the limitations, this work provides detailed knowledge of the consumption of RF and NRF of a specific population in the country.
The findings of this research have substantial implications for health policies and interventions aimed at improving the well-being of the young population, especially in southeastern Mexico and potentially in similar contexts. It is clear from this study that dietary and lifestyle habits that emerged during the COVID-19 pandemic, including increased consumption of non-recommended foods and lack of physical activity, have direct implications for young people’s health. Specifically, these factors are associated with an increased risk of obesity and symptoms of depression, highlighting the need for effective public health strategies that promote healthier eating and physical activities, especially in circumstances of social isolation.
Conclusion
In this study, high rates of obesity and symptoms of depression were found during the COVID-19 pandemic. The high prevalence of obesity, symptoms of depression, and diabetes among the youth surveyed suggests the urgency of addressing these health problems. Likewise, high consumption of homemade food at mealtimes and fruit at snack time was observed. In contrast, bottled soft drinks were consumed more during lunch. Although most of the surveyed population indicated physical activity, the inactive population was high. NRF consumption during dinner and snacking were identified as the main risk factors for obesity and symptoms of depression during social isolation. The results contribute significantly to our understanding of the broader health consequences of the pandemic and the measures needed to address them. In these sense, targeted dietary and therapeutic strategies are needed, as well as a healthy lifestyle in the youth population of the southeast, to improve their quality of life in the post-COVID-19 pandemic stage.

