










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.28 no.3 Ciudad de México jul./sep. 2024 Epub 01-Sep-2025
https://doi.org/10.22201/fo.1870199xp.2024.28.3.91108
Clinical case
Tomographic and periodontal clinical parameters two years after surgical exposition of maxillary impacted canines. Case series
1 Egresada, Especialidad de Periodoncia e Implantología, División de Estudios de Posgrado e Investigación, Facultad de Odontología, UNAM, México.
2 Docente, Especialidad Periodoncia e Implantología. División de Estudios de Posgrado e Investigación, Facultad de Odontología, UNAM, México.
3 Docente, Área Básicas Médicas, División de Estudios de Posgrado e Investigación, Facultad de Odontología, UNAM, México.
Introduction: This report on clinical cases presents the evaluation of periodontal parameters that should be assessed in patients with impacted maxillary canines as predictors of post-operative results. Objective: To evaluate the surgical follow-up after two years, analyzing the tomographic and clinical periodontal parameters of the impacted maxillary canines that underwent an orthodontic traction procedure after exposure by using apical and lateral reposition flaps from existing keratinized tissue. Case presentation: Clinical parameters were evaluated: plaque index, gingival index, pocket depth, keratinized tissue width, and Cairo esthetic score. Tomographic parameters were also evaluated: bone height, bone support, and bone thickness. After two years of post-operative follow-up, clinical parameters showed the absence of plaque in the gingival area, absence of inflammation, bleeding, color change, and absence of periodontal pockets. The width of keratinized tissue obtained was 4.3 mm and it always kept up with the tooth’s movement. Its aesthetics and quality are comparable to the adjacent tooth. Cone-beam computed tomography showed that the bone height was greater in the labial region and lesser in the palatal region and the percentage of bone support was related to the height of the alveolar crests. The thickness of the labial bone plate was smaller compared to the thickness of the palatal bone plate. Conclusion: The apical-positioned flap and the lateral-positioned flap have been demonstrated as periodontal plastic surgery techniques to maintain an appropriate width of keratinized tissue around natural teeth. In the literature, there are not sufficient reports showing the joint evaluation of clinical and tomographic periodontal parameters, so they must continue to be reported to create an evaluation protocol before canine exposure surgery in the future.
Keywords: impacted canines; apical and lateral positioned flap; periodontal health
Introducción: este reporte de casos clínicos presenta la evaluación de parámetros periodontales, que habitualmente deberán valorarse en pacientes con caninos maxilares impactados como predictores de los resultados posoperatorios. Objetivo: evaluar el seguimiento posquirúrgico a los dos años, analizando los parámetros periodontales clínicos y tomográficos de caninos maxilares impactados sometidos a tracción ortodóncica después de ser expuestos utilizando colgajos de reposición apical y lateral a partir de tejido queratinizado existente. Presentación de casos: se evaluaron parámetros clínicos: índice de placa, índice gingival, profundidad de bolsa, ancho de tejido queratinizado y puntuación estética de Cairo; además, parámetros tomográficos: altura ósea, soporte óseo y grosor óseo. Después de dos años de seguimiento postoperatorio, los parámetros clínicos mostraron ausencia total de placa en el área gingival, ausencia de inflamación, hemorragia y cambio de color y ausencia de bolsas periodontales. El ancho de tejido queratinizado obtenido fue de 4.3mm y siguió al diente en sus movimientos; su estética y calidad fue comparable al de los dientes vecinos. En la tomografía se observó que la altura ósea fue mayor en la región vestibular y menor en la región palatina, el porcentaje de soporte óseo estuvo relacionado con la altura de las crestas alveolares. El grosor de la cortical ósea vestibular fue menor en relación al grosor de la cortical ósea palatina. Conclusión: las técnicas de cirugía plástica periodontal mediante colgajos de reposición apical y lateral han mostrado ser eficaces en el mantenimiento de un adecuado tejido queratinizado alrededor de dientes naturales. Existen limitados reportes donde se presente la evaluación conjunta de parámetros periodontales clínicos y tomográficos. Este reporte de casos contribuye para crear en un futuro, un protocolo de evaluación previo a la cirugía de exposición de caninos.
Palabras clave: caninos impactados; colgajo reposición apical y lateral; salud periodontal
Introduction
An impacted tooth is defined as a tooth that has not erupted in its functional position and its follicular sac does not maintain a connection with the oral cavity within its normal growth period1,2. Maxillary canines occupy the second place in impaction, after the third molars1. According to Grisar et al, 42.5% of cases present labial impaction2. Its etiology is multifactorial and includes dental discrepancy, ectopic position of the tooth germ, absence of space and orientation, presence of hard or soft tissue pathologies, and genetic factors2,3. In addition, 90% of cases of impacted teeth are covered only by soft tissue3.
Labial impactions are usually difficult to manage without causing periodontal complications. It is estimated that the surgical technique used to expose the canine is critical in the final periodontal result because it can affect the amount of gingiva adhered to the crown of the tooth once it has reached its functional position3. The modification of the Ericson and Kurol analysis proposed by Lindauer et al. in 1992, allows for determining the position of the impacted canines in the maxilla, taking the lateral incisor as a reference4. Sector I is located distal to the tangent that touches the distal surface of the lateral incisor, sector II includes the area from the tangent on the distal surface to the midline bisector of the lateral incisor, sector III extends from the midline bisector to the tangent that crosses the mesial surface of the lateral incisor and sector IV includes all areas mesial to sector III4.
Before the surgery, clinical periodontal parameters such as plaque index (PI) and gingival index (GI), pocket depth (PD), keratinized tissue width (KT), Cairo’s root coverage esthetic score (RES), as well as tomographic parameters such as bone height (BH), bone support (BS) and bone thickness (BT), should be evaluated to determine the surgical technique to treat impacted or included teeth, as it involves the use of periodontal plastic surgery techniques such as gingivectomy, labial repositioning flap, apical repositioning flap, and lateral repositioning flap1. The purposes of surgical treatment are to obtain direct access to the clinical crown and sufficient bone and mucogingival release for orthodontic button placement3,5,6.
Orthodontic treatment of impacted maxillary canines is usually a challenge because several factors must be taken into account such as proper selection of the surgical technique where the labio-palatal position, vertical position of the tooth regarding the mucogingival line, mesiodistal position of the canine crown and amount of keratinized tissue are considered; the orthodontic traction modality to achieve satisfactory esthetic and periodontal health results; sufficient space in the dental arch to allow proper alignment of the canine, accurate anchorage preparation, careful biomechanical planning and a magnitude of force used within a physiological range (which should not exceed 0.6 N)7.
These two clinical cases aimed to evaluate the two-year postsurgical follow-up by analyzing the clinical and tomographic periodontal parameters of impacted maxillary canines subjected to orthodontic traction after exposure using apical and lateral repositioning flaps from existing keratinized tissue.
Presentation of clinical cases
Case 1
A 13-year-old female patient attended the Periodontics and Implantology Clinic of the Division of Postgraduate Studies and Research of the Universidad Nacional Autónoma de México (DEPeI-UNAM), referred by the Department of Orthodontics with a diagnosis of impacted maxillary canine, tooth #13, sector III4 for surgical exposure.
Periodontally, her diagnosis was mild, generalized gingivitis induced by dental biofilm. After performing periodontal phase I, the tissue was in gingival health. Apical repositioning flap surgery was performed because, within the clinical periodontal parameters, a keratinized tissue width of 3mm was recorded in tooth 13. The tomography showed the impacted tooth #13, with the absence of cortical tissue in the labial region and at the level of the cementoenamel junction of tooth #11. These findings allowed us to determine the position of tooth 13 in sector III according to Lindauer’s diagnosis 4 and helped us in the selection of the surgical technique.
An apical repositioning flap was chosen to preserve as much keratinized tissue as possible8, and because of the apical position of the canine regarding the mucogingival line. In the surgical procedure, a partial thickness flap was designed, two-thirds of the coronal crown was exposed and the orthodontic button (Borgatta®) was attached as close as possible to the incisal edge using the 3M adhesive system®. The flap was then repositioned apically and sutured to the periosteum with single stitches and 6-0 polyglycolic acid suture so that it covered 2 to 3 mm of the crown (Figure 1. A-D).
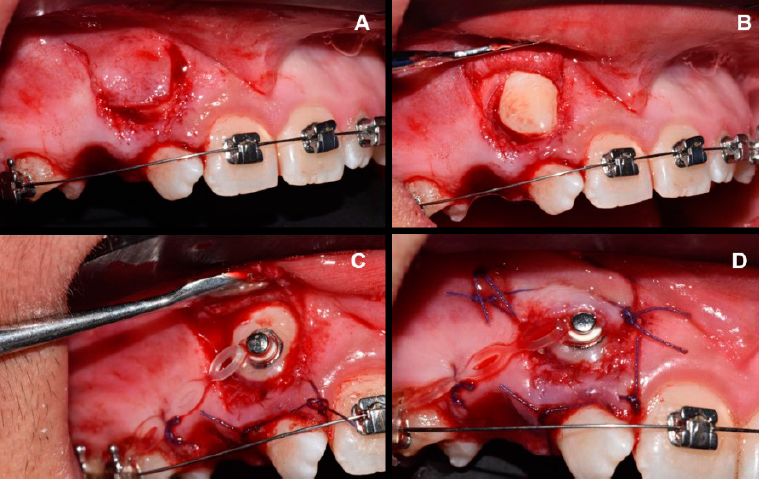
Figure 1 Periodontal plastic surgery technique for the exposure of tooth #13. Case 1. A. Design of a partial thickness flap to be repositioned apically. B. Exposure of tooth #13. C. Placement of the orthodontic button. D. Apical repositioning of the flap using simple stitches and 6-0 polyglycolic acid suture.
Traction of tooth #13 was activated at the time of orthodontic button placement with a second-generation Ormco closed elastic chain®, in the direction of tooth #14 to guide eruption (Figure 1. C-D). Traction was performed intermittently from tooth exposure until the ninth month of orthodontic follow-up where tooth positioning was achieved with light and continuous forces at one-year post-surgery.
Case 2
Female patient, 13 years old, attended the Periodontics and Implantology clinic of the DEPeI UNAM, referred by the Department of Orthodontics with a diagnosis of impacted maxillary canine teeth #13 and #23, sector IV4, for surgical exposure by apical repositioning flap for both teeth and a second flap surgery with lateral repositioning for tooth #13. Future extractions of teeth #11 and 21 were planned due to severe root resorption.
Periodontally, mild, generalized dental biofilm-induced gingivitis was diagnosed. After performing periodontal phase I the tissue was in gingival health. At the time of surgery, the width of keratinized tissue in teeth #13 and 23 was 3mm. The tomography allowed us to determine the position of teeth #13 and 23 in sector IV according to Lindauer’s diagnosis4 and it was observed that tooth #13 was in an apical position to tooth #23 and covered by labial cortical bone. These findings helped us to determine the surgical technique and we chose to perform an apical repositioning flap in both canines to preserve as much keratinized tissue as possible8, because of the apical position of the canines regarding the mucogingival line.
The surgical procedure was performed using the apical repositioning flap technique previously described in case 1, both for tooth 13 and tooth 23; with the only difference being that in tooth #13 cortical bone was removed before the removal of the connective tissue follicle (Figure 2. A-B). The traction of tooth #23 was activated at two weeks post-surgery from a closed metal ligature (TD) fixed from the orthodontic button (Borgatta®), attached by 3M adhesive system®, in the direction of tooth #21 to guide the eruption. Traction was performed intermittently for six months.
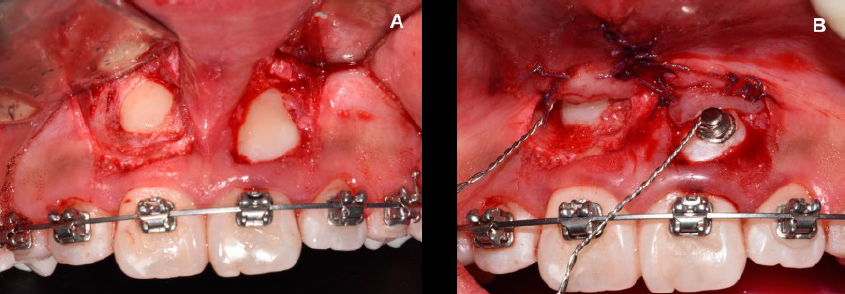
Figure 2 Periodontal plastic surgery techniques for exposure of teeth #13 and 23. A. Design of a partial thickness flap to be repositioned apically over both teeth. B. Placement of orthodontic buttons and apical repositioning of the flaps from simple stitches and 6-0 polyglycolic acid suture.
Six months after surgery, it was observed that the keratinized tissue adjacent to the orthodontic button of tooth #13 was covering it and would not facilitate the placement of the bracket for future tooth traction, so it was decided to perform a second surgery with a lateral repositioning flap, after removing the orthodontic button (Figure 3. A-D).
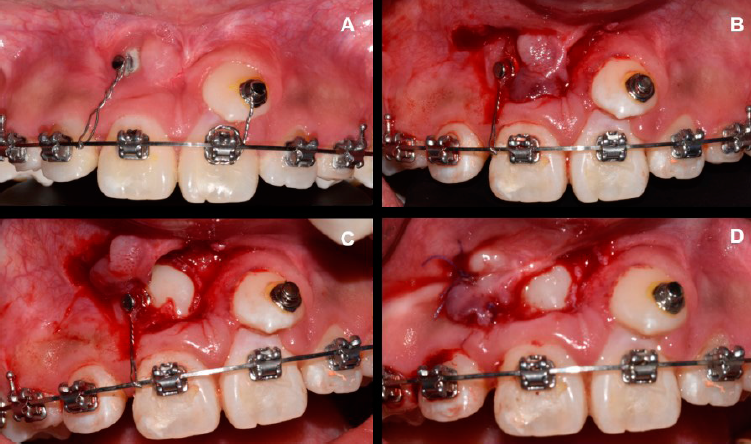
Figure 3 Periodontal plastic surgery technique for exposure of tooth #13, 6 months after the previous surgery. A. Presence of keratinized tissue lateral to tooth #13. B. Design of a partial-thickness flap to be repositioned laterally. C. Exposure of tooth #13 and placement of the orthodontic button. D. Lateral repositioning of the flap using simple stitches and 6-0 polyglycolic acid suture.
Seven months after the second surgery, the canines reached occlusion and the corresponding alveolar area of teeth #11 and 21, which were extracted because they had a hopeless prognosis due to complete root resorption and severe mobility.
At two years post-surgery, once the teeth reached occlusion and their position in the corresponding alveolar area, the clinical parameters were assessed in sequential order: PI, GI, PB, KT, RES, and same order with the tomographic parameters BH, BS, and BT (Figure 4 A-B).
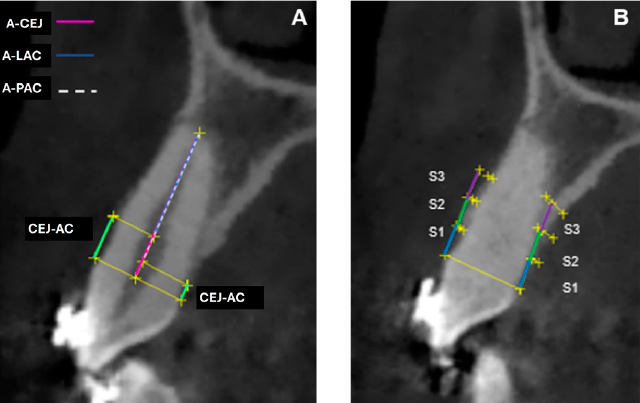
Figure 4 Tomographic analysis. Schematic drawing to calculate the labial and palatal bone height (BH) and bone support (BS) of the exposed canines at two years post-surgery. The green lines identify the cementoenamel junction-alveolar crest (CEJ-AC) distance in both the labial and palatal regions, the pink line identifies the apex-cementoenamel junction (A-CEJ) distance, the blue line marks the apex-labial alveolar crest (A-LAC) distance, and the dashed white line identifies the apex-palatal alveolar crest (A-PAC) distance. The bone percentage was calculated by dividing the apex-alveolar crest distance by the apex-enamel cementoenamel junction distance. Schematic drawing for calculating the labial and palatal bone thickness (BT) of exposed canines at two years post-surgery. Taking as reference the distance between the root surface and the cortex, perpendicular to the long axis of the tooth, at 3 mm S1), 6 mm (S2), and 9 mm (S3) (blue, green, and purple lines respectively) from the cementoenamel junction.
Follow-up
Case 1
Tooth #13: In the clinical parameters, PI=0 showed the absence of plaque in the gingival area; GI=0, showed gingiva with the absence of inflammation, hemorrhage, and alteration of color change, PD<4mm, with the absence of periodontal pockets (Table 1), KT of 5mm (Figure 5 A-C).
Table 1 Clinical and tomographic periodontal parameters obtained two years after surgery for cases 1 and 2. The percentage of bone support was obtained by dividing the apex-to-alveolar crest distance by the apex-cementoenamel junction distance.
| Case 1 | Case 2 | |||
|---|---|---|---|---|
| Variables | Region | Tooth #13 | Tooth #13 | Tooth #23 |
| Plaque index | 0 | 0 | 0 | |
| Gingival index | 0 | 0 | 0 | |
| Pocket Depth | Mesio-labial | 3 | 2 | 2 |
| Labial | 1 | 1 | 1 | |
| Disto-labial | 3 | 3 | 3 | |
| Mesio-lingual | 3 | 2 | 2 | |
| Lingual | 3 | 2 | 3 | |
| Disto-lingual | 3 | 2 | 3 | |
| Width of keratinized tissue | Labial | 5 mm | 5 mm | 3 mm |
| Bone height (CEJ- alveolar crest) | Labial | 3.96 mm | 4.80 mm | 2.26 mm |
| Palatal | 1.42 mm | 1.33 mm | 1.31 mm | |
| Apex-Alveolar crest | Labial | 9.86 mm | 5.01 mm | 3.77 mm |
| Palatal | 12.28 mm | 8.89 mm | 4.84 mm | |
| Apex-cementoenamel junction | 13.87 mm | 10.16 mm | 6.16 mm | |
| Bone support | Vestibular | 71% | 49% | 61% |
| Palatine | 88% | 87% | 78% | |
| Labial bone thickness | S1 | 0.53 mm | 0.48 mm | 0.42 mm |
| S2 | 0.49 mm | 0.74 mm | 0.60 mm | |
| S3 | 0.58 mm | 0.71 mm | - | |
| Palatal bone thickness | S1 | 0.83 mm | 2.49 mm | 1.70 mm |
| S2 | 1.87 mm | 4.00 mm | 3.93 mm | |
| S3 | 2.49 mm | 2.67 mm | - | |
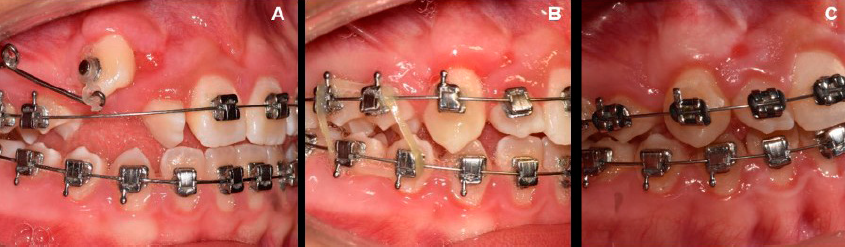
Figure 5 Assessment of keratinized tissue obtained around tooth #13 after surgery. The tissue followed the tooth during its movements and is comparable to that of the adjacent teeth. A. 6 months post-surgery. B. One-year post-surgery. C. Two years after surgery.
Table 2 shows the RES, where the score for the gingival margin level was 6, i.e., absence of gingival recession; for the marginal tissue contour the result was 1, showing a scalloped marginal contour; the variable of texture with a score of 0 showed the presence of a scar; for color, the score was 1, showing adequate integration with the adjacent soft tissues; for its part, the MGL was shown to be aligned with the adjacent teeth, obtaining a score of 1. A total score of 9 was obtained.
Table 2 Cairo’s esthetic scores obtained two years after surgery for cases 1 and 2.
| Case 1 | Case 2 | ||
|---|---|---|---|
| Variables | Tooth #13 | Tooth #13 | Tooth #23 |
| Gingival margin level | 6 | 6 | 6 |
| Marginal tissue contour | 1 | 1 | 1 |
| Texture | 0 | 0 | 0 |
| Color | 1 | 0 | 1 |
| MGL lineup | 1 | 1 | 1 |
| TOTAL | 9 | 8 | 9 |
Table caption: Gingival margin level. 0=presence of gingival recession, 6=absence of gingival recession. Marginal tissue contour. 0=irregular gingival margin (does not follow CEJ), 1=adequate marginal contour/scalloped gingival margin. Texture. 0=scar formation and/or keloid appearance; 1=absence of scar or keloid formation. Color. 0=tissue color varies from the gingival color of adjacent teeth; 1=normal color and integration with adjacent soft tissues. MGL alignment. 0=MGL misaligned with MGL of adjacent teeth; 1=MGL aligned with MGL of adjacent teeth.
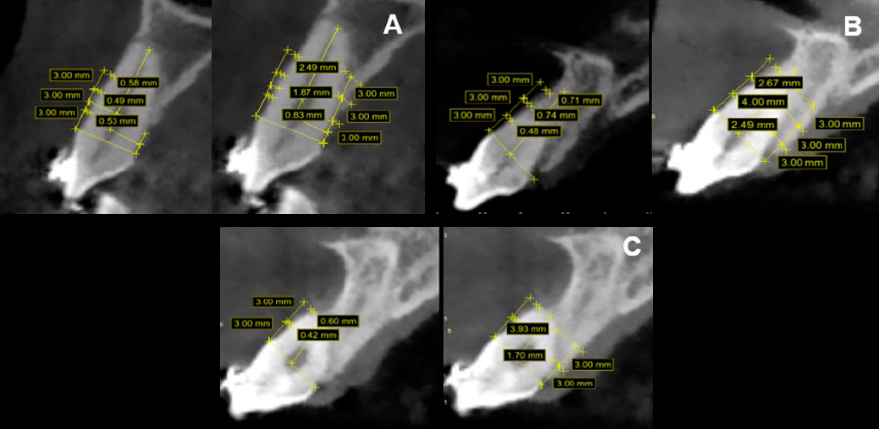
In the tomographic parameters the BH in the vestibular region was higher (3.96 mm) relative to the BH in the palatal region (1.42 mm); the percentage of labial BS was lower (71%) relative to the percentage of palatal BS (88%) (Table 1) (Figure 6 A). BT was lower at all three labial cortical sites (S1=0.53 mm) (S2=0.49 mm) (S3=0.58 mm) relative to BT at all three palatal cortical sites (S1=0.83 mm) (S2=1.87 mm) (S3=2.49 mm) (Table 1) (Figure 7A).
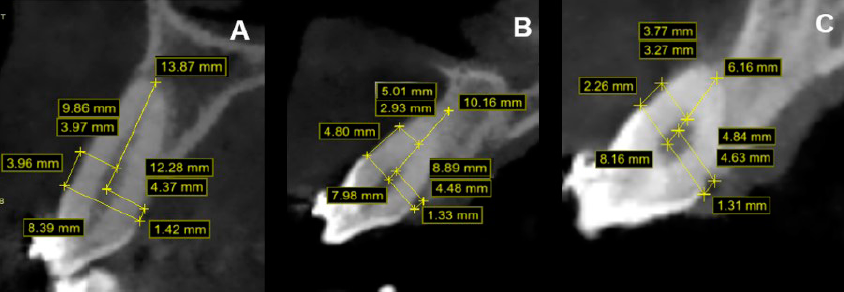
Figure 6 Tomographic image showing the measurements of the labial and palatal bone height (BH) and bone support (BS) of the exposed canines at two years post-surgery. A. Tooth #13, case 1. B. Tooth #13, case 2. C. Tooth #23, case 2.
Case 2
Teeth #13 and 23. In the clinical parameters, PI=0 presented an absence of plaque in the gingival area, GI=0, showed gingiva with absence of inflammation, bleeding, and color change, PD<4mm with absence of periodontal pockets (Table 1), KT of 5mm and 3mm for teeth 13 and 23 respectively (Figure 8 A-C). The RES showed a score of 6 for the level of the gingival margin in the two canines, i.e., absence of gingival recession; for marginal tissue contour the score was 1 for both teeth, evidencing a scalloped marginal contour; the texture variable with a score of 0, showed the presence of a scar around the two canines; For color, the score was 0 for tooth #13, showing a color variation with the adjacent teeth, and 1 for tooth #23, showing an adequate integration with the adjacent soft tissues; for its part, the MGL was aligned with the adjacent teeth, obtaining a score of 1 for both teeth. A total score of 8 was obtained for tooth #13, and 9 for tooth #23 (Table 2).

Figure 8 Assessment of keratinized tissue obtained around teeth #13 and 23 after surgery. The tissue followed the tooth during its movements and is comparable to that of the adjacent teeth. A. 6 months post-surgery. B. One-year post-surgery. C. At two years post-surgery
In the tomographic parameters for tooth #13, BH in the labial region was higher (4.80 mm) relative to the palatal AO (1.33 mm); the percentage of labial BS was lower (49%) relative to the percentage of palatal BS (87%). For tooth #23, BH in the labial region was higher (2.26 mm) relative to the palatal BH (1.31 mm); the labial BS percentage was lower (61%) relative to the palatal BS percentage (78%) (Table 1) (Figure 6 B-C).
It was observed that the BT for the labial cortex of tooth #13 was lower at the three points (S1=0.48 mm) (S2=0.74 mm) (S3=0.71 mm) relative to the BT at the three points of the palatal cortex (S1=2.49 mm) (S2=4.00 mm) (S3=2.67 mm). For tooth #23 the BT of the labial cortex was lower at the two points (S1=0.42 mm) (S2=0.60 mm) relative to the BT at the two points of the palatal cortex (S1=1.70 mm) (S2=3.93 mm), the third point (S3) could not be evaluated due to the decreased height of the labial and palatal cortices (Table 1) (Figure 7 B-C).
Discussion
This case report coincides with the study by Cercadillo-Ibarguren et al.9 in which it was observed that GI, bleeding on probing (BP) and PD did not show significant differences in surgically exposed teeth, and teeth subjected to orthodontic traction. From these results, it could be concluded that the apically repositioned flap technique proved to be a predictable procedure that maintains periodontal health in the long term. The results of this case report showed that the average KT obtained around the exposed teeth was 4.3 mm, similar to that of the adjacent teeth. These results are similar to those reported by Lee et al.10 where the group of teeth exposed by apically repositioned flaps showed pocket depth and keratinized tissue width values comparable to those of adjacent teeth.
This clinical case report included the RES11 which, despite being oriented to evaluate esthetic results after root coverage surgical techniques, is very practical for the evaluation of the state of the soft tissues at six months post-surgery. In the case of texture, the exposed canines obtained a value of 0 because they showed the formation of a scar; this same situation was reported in the study by Cercadillo-Ibarguren et al.9 in which 86.7% of the teeth exposed by an apical repositioning flap showed signs of scarring and 46.7% showed the presence of a bilateral scar in the soft tissues of the intervened teeth. In the color variable, tooth #13 exposed in case 2, obtained a score of 0 since a reddish color incompatible with gingivitis, varied to that of the adjacent tissues. The study by Cercadillo-Ibarguren et al.9 reported the same situation and attributed it to the fact that the alveolar mucosa accumulates from an apical position together with the sutured flap in its final position.
Regarding post-surgical bone assessment, the results showed that the group of surgically exposed teeth presented a higher BH in the labial region compared to the palatal region where the CEJ-AC distance was lower. Guo et al.12 in their systematic review and meta-analysis suggest that during orthodontic movements bone remodeling mainly involves bone resorption in the palatal region and limited bone apposition in the labial region. Castro et al.13 reported that maxillary canines reported a high risk of vertical alveolar bone loss during orthodontic movements. A greater CEJ-AC distance was reported in the vestibular region of tooth #13 exposed in case 2 as compared to case 1. Kohavi et al.14 recommend the use of light forces during tilting and extrusion movements to avoid less bone loss during traction of impacted teeth. The BT of the exposed canines, assessed at 3 mm, 6 mm, and 9 mm from the CEJ, was lower in the labial cortex than in the palatal cortex at the same points. The systematic review by Mandelaris et al.15 reports a higher incidence of bone dehiscence in teeth subjected to orthodontic forces aimed at moving the dentition out of the socket.
The literature reports other possibilities regarding techniques for canine exposure, such as a closed surgical approach. However, this technique has disadvantages such as ankylosis, lack of direct control of movement, and the need for an additional surgical procedure if the orthodontic button is debonded; in addition, mucogingival problems can be created by inadequate orthodontic mechanics causing the tooth to erupt through the mucosa8.
Conclusions
Both the apical repositioning flap used on teeth #13 in case one and #13 and #23 in case two -as well as the lateral repositioning flap used on tooth #13 in case two- have proven to be effective periodontal plastic surgery techniques for maintaining an adequate width of keratinized tissue around natural teeth. These techniques contribute significantly to the preservation of periodontal health and successful interdisciplinary treatment.
It is important to note that there are limited reports in the literature that jointly evaluate clinical and tomographic periodontal parameters. Therefore, clinical case reports should continue to be made, with the aim of developing in the future an evaluation protocol prior to canine exposure surgery. This will allow the establishment of criteria with more clinical evidence for planning these surgical procedures.
Acknowledgments
To the Department of Orthodontics of the DEPeI of the UNAM, to resident Andrés Heredia Montiel and his advisor, Dr. Francisco Marichi Rodríguez; and to resident Fernanda López Ortega and her advisor, Dr. Fabiola Hernández Girón.
REFERENCES
1. Incerti-Parenti S, Checchi V, Ippolito DR, Gracco A, Alessandri-Bonetti G. Periodontal status after surgical- orthodontic treatment of labially impacted canines with different surgical techniques: A systematic review. Am J Orthod Dentofacial Orthop. 2016; 149(4): 463-472. DOI: 10.1016/j.ajodo.2015.10.019 [ Links ]
2. Grisar K, Fransen J, Smeets M, Hoppenreijs T, Ghaeminia H, Politis C, et al. Surgically assisted orthodontic alignment of impacted maxillary canines: A retrospective analysis of functional and esthetic outcomes and risk factors for failure. Am J Orthod Dentofacial Orthop. 2021; 159(6): e461-e471. DOI: 10.1016/j.ajodo.2020.12.019 [ Links ]
3. Henner N, Pignoly M, Antezack A, Monnet-Corti V. Periodontal approach of impacted and retained maxillary anterior teeth. J Dentofacial Anom Orthod. 2018; 21(2): 204. DOI: 10.1051/odfen/2018053 [ Links ]
4. Lindauer SJ, Rubenstein LK, Hang WM, Andersen WC, Isaacson RJ. Canine impaction identified early with panoramic radiographs. J Am Dent Assoc. 1992; 123(3): 91-97. DOI: 10.14219/jada.archive.1992.0069 [ Links ]
5. Tatakis DN, Chambrone L, Allen EP, Langer B, McGuire MK, Richardson CR, et al. Periodontal soft tissue root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015; 86(2S): S52-S55. DOI: 10.1902/jop.2015.140376 [ Links ]
6. Scheyer ET, Sanz M, Dibart S, Greenwell H, John V, Kim DM, et al. Periodontal soft tissue non-root coverage procedures: a consensus report from the AAP Regeneration Workshop. J Periodontol. 2015; 86(2S):S73-S76. DOI: 10.1902/jop.2015.140377 [ Links ]
7. Potrubacz MI, Chimenti C, Marchione L, Tepedino M. Retrospective evaluation of treatment time and efficiency of a predictable cantilever system for orthodontic extrusion of impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2018; 154(1): 55-64. DOI: 10.1016/j.ajodo.2017.10.027 [ Links ]
8. Cooke J, Wang HL. Canine impactions: incidence and management. Int J Periodontics Restorative Dent. 2006; 26(5): 483-91. PMID: 17073358 [ Links ]
9. Cercadillo-Ibarguren I, Gargallo-Albiol J, Abad-Sánchez D, Echeverría-García JJ, Berini-Aytés L, Gay-Escoda C. Periodontal health and esthetic results in impacted teeth exposed by apically positioned flap technique. Med Oral Patol Oral Cir Bucal. 2011; 16(1): e89-95. DOI: 10.4317/medoral.16.e89 [ Links ]
10. Lee JY, Choi YJ, Choi SH, Chung CJ, Yu HS, Kim KH. Labially impacted maxillary canines after the closed eruption technique and orthodontic traction: A split-mouth comparison of periodontal recession. J Periodontol. 2019; 90(1): 35-43: 10.1002/JPER.18-0034 [ Links ]
11. Cairo F, Rotundo R, Miller PD, Pini Prato GP. Root coverage esthetic score: a system to evaluate the esthetic outcome of the treatment of gingival recession through evaluation of clinical cases. J Periodontol. 2009; 80(4): 705-710. DOI: 10.1902/jop.2009.080565 [ Links ]
12. Guo R, Zhang L, Hu M, Huang Y, Li W. Alveolar bone changes in maxillary and mandibular anterior teeth during orthodontic treatment: A systematic review and meta-analysis. Orthod Craniofac Res. 2021; 24(2): 165-179. DOI: 10.1111/ocr.12421 [ Links ]
13. Castro LO, Castro IO, de Alencar AHG, Valladares-Neto J, Estrela C. Cone beam computed tomography evaluation of distance from cemento-enamel junction to alveolar crest before and after nonextraction orthodontic treatment. Angle Orthod. 2016; 86(4): 543-549. DOI: 10.2319/040815-235.1 [ Links ]
14. Kohavi D, Becker A, Zilberman Y. Surgical exposure, orthodontic movement, and final tooth position as factors in periodontal breakdown of treated palatally impacted canines. Am J Orthod. 1984; 85(1): 72-77. DOI: 10.1016/0002-9416(84)90124-6 [ Links ]
15. Mandelaris GA, Neiva R, Chambrone L. Cone-beam computed tomography and interdisciplinary dentofacial therapy: An American Academy of Periodontology best evidence review focusing on risk assessment of the dentoalveolar bone changes influenced by tooth movement. J Periodontol. 2017; 88(10): 960-977. DOI: 10.1902/jop.2017.160781 [ Links ]
Cite as:
Mier-Ortiz MJ, López-Reynoso PA, Yáñez BR, Esquivel-Chirino C. Parámetros periodontales clínicos y tomográficos dos años después de la exposición quirúrgica de caninos maxilares. Reporte de casos. [Tomographic and Periodontal Clinical Parameters Two Years after Surgical Exposure of Maxillary Impacted Canines. Case Series]. Rev Odont Mex. 2024; 28(3): 45-56. DOI: 10.22201/fo.1870199xp.2024.28.3.91108
Received: August 29, 2023; Accepted: August 23, 2024
 Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
