










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.27 no.3 Ciudad de México jul./sep. 2023 Epub 16-Ene-2025
https://doi.org/10.22201/fo.1870199xp.2023.27.3.85102
Clinical cases
Decompression of Odontogenic Keratocyst with 3D-Printed Cannula. Case Report
1Residente Cirugía Oral y Maxilofacial, Universidad Nacional Autónoma de México, Escuela Nacional de Estudios Superiores-León, Guanajuato, México.
2Profesor adscrito de Cirugía Oral y Maxilofacial, Universidad Nacional Autónoma de México, Escuela Nacional de Estudios Superiores-León, Guanajuato, México
3Profesora del Laboratorio de Nanoestructuras y Biomateriales, Universidad Nacional Autónoma de México, Escuela Nacional de Estudios Superiores-León, Guanajuato, México
Introduction:
The odontogenic keratocyst is a developmental epithelial cyst that comes from the remains of the dental lamina, of relatively high prevalence and aggressive behavior. In large lesions, it is possible to decompress by installing a 3D-printed cannula, which facilitates the subsequent enucleation of the cystic lesion.
Case presentation:
A 26-year-old female patient presented an increase in volume in the right hemiface at the level of the middle and lower facial third after approximately one year of evolution. Imaging and histopathological studies were performed, and the diagnosis was odontogenic keratocyst. The treatment consisted of decompressing the lesion with the placement of a cannula designed in the Blender software and 3D-printed with BioMed Clear™ biocompatible resin. Then the enucleation and curettage of the remaining lesion were performed, plus the application of 5-fluorouracil as an adjuvant. In control studies, bone neoformation can be observed, with no data on recurrence.
Conclusions:
The 3D-printed cannula is a customized device that offers accuracy and precision in the treatment of decompression.
Keywords: Odontogenic keratocyst; decompression; 3D cannula; 5-fluorouracil
Introducción:
El queratoquiste odontogénico es un quiste epitelial del desarrollo que proviene de los restos de la lámina dental, de prevalencia relativamente alta y de comportamiento agresivo. En lesiones de gran tamaño es posible realizar una descompresión mediante la instalación de una cánula impresa en 3D, lo que facilita la posterior enucleación de la lesión quística.
Objetivo:
Presentar una alternativa en la descompresión para el tratamiento del queratoquiste odontogénico.
Presentación del caso:
Paciente femenina de 26 años, presenta aumento de volumen en la hemicara derecha a nivel de tercio medio e inferior facial de aproximadamente un año de evolución. Se realizaron estudios de imagen e histopatológicos cuyo diagnóstico fue queratoquiste odontogénico. El tratamiento consistió en realizar una descompresión de la lesión con la colocación de una cánula diseñada en el software Blender, la cual fue impresa en 3D con resina biocompatible BioMed Clear™. Luego se realizó la enucleación y curetaje de la lesión remanente, más la aplicación de 5-Fluoracilo como coadyuvante. En los estudios de control se puede observar neoformación ósea, sin datos de recidiva.
Conclusiones:
La cánula impresa en 3D es un dispositivo personalizado que ofrece exactitud y precisión en el tratamiento de la descompresión.
Palabras clave: queratoquiste odontogénico; descompresión; cánula 3D; 5-fluoracilo
Introduction
The odontogenic keratocyst (OKC) is a developmental epithelial cyst arising from the remains of the dental lamina. The term OK was first used by Philipsen in 19531; although other authors mention that the term was first used in 19562. In 2005, it was classified by the World Health Organization (WHO) as a keratocystic odontogenic tumor (KOT). In 2017, KOT was again classified as a developmental odontogenic cyst3. And in the current classification, it continues to be considered as a cyst4. Compared with other cysts of the jaw, OKC is unique due to its distinctive clinical features, including potentially aggressive behavior, high recurrence rate, and an association with the nevoid basal cell carcinoma syndrome (NBCCS)5.
Approximately half of all keratocysts occur at the angle of the mandible and extend for varying distances into the ascending ramus and forward into the body2,6. In many cases, patients are remarkably asymptomatic until the cysts reach a large size and involve the maxillary sinus, ascending ramus, condylar processes, and coronoids6. Symptoms related to pain, infection, or pathologic fracture may occur less frequently7. The most commonly used radiological imaging techniques in the study of OKCs are orthopantomography and computed tomography (CT)8,9. OKCs may exhibit imaging features almost indistinguishable from other osteolytic lesions of the jaws; therefore, to obtain a definitive diagnosis, histopathologic examination is required9. Several treatment modalities have been reported, including marsupialization, decompression, enucleation with or without adjuvants, cryotherapy, and resection. Lesion recurrence rates vary according to the treatment modality chosen, with the lowest rate associated with surgical resection10.
Although most recurrences occur in the first 5 years, they can also occur after 10 years or even more11. In large lesions, it is possible to perform decompression of the lesion by installing a cannula, for subsequent enucleation of the remaining OKC12. As a driving factor of the fourth industrial revolution, 3D printing has had a global impact on healthcare, with 3D printed and patient-customized tools replacing outdated methods13. Virtual surgical planning and computer-aided fabrication of 3D printed devices provide the surgeon with multiple advantages14. When comparing traditional manufacturing methods with additive manufacturing and 3D printing, they stand out in their ability to manufacture complex structures faster and with high precision13. The materials currently used are mainly based on the use of naturally occurring polymers or synthetic molecules15. Biomed Clear™ is a resin for ink light-curing 3D printing, with good physical and mechanical properties15,16, this makes it able to remain for a long time in a biological environment and is biocompatible17.
Clinical case presentation
A 26-year-old female patient presented at the clinic of the School of Dentistry of the National School of Higher Education, Leon, UNAM, who reported a tumor in the mandible with approximately one year of evolution. In the extraoral physical examination, an increase in volume was observed in the right hemiface at the level of the middle and lower third of the face (Figure 1. A). In the intraoral examination, a lesion was observed expanding vestibular and lingual cortices; palpation was of indurated consistency, and no other systemic or important disease was found.
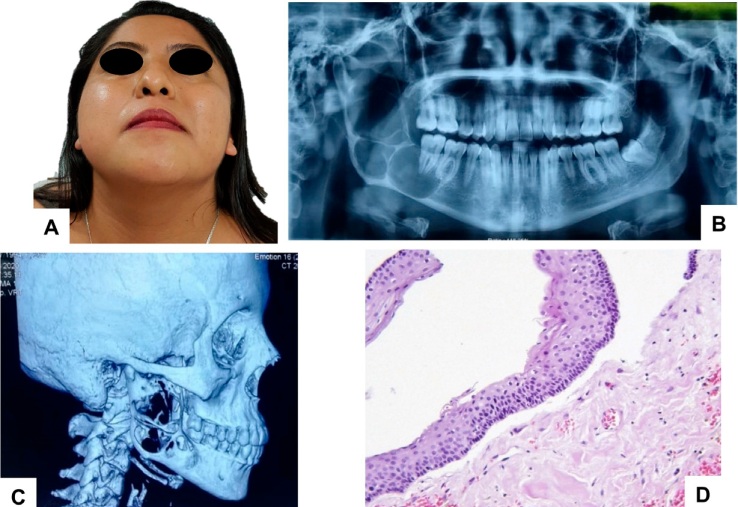
Figure 1 Initial photo. A. Antero-inferior view, volume increase in the right hemiface. Imaging studies. B. Orthopantomography shows multilocular areas at the level of the body, angle, and mandibular ascending branch. C. 3D reconstruction of computed tomography of the skull, showing osteolytic pattern with cortical expansion. D. Photomicrograph stained with hematoxylin and eosin at 100X, shows cystic cavity lined by parakeratinized stratified squamous epithelium with corrugated areas.
In the imaging studies, in the orthopantomography of the right side in the mandibular region, a multilocular radiolucent area was observed, from the first molar to the ascending branch, with well-defined and sclerotic borders. In the three-dimensional reconstruction of the simple cranial computed tomography, an image of the lytic aspect was observed, with fine septa in its interior of multilocular aspect with an expansion of bony cortices (Figure 1. B-C).
As a diagnostic impression OKC was suspected due to the location of the lesion, the multilocular radiolucency with well-defined borders, and the age of the patient. Conventional ameloblastoma and odontogenic myxoma were suspected as differential diagnoses. As part of the diagnostic protocol, an exploratory puncture was performed and the material was yellowish-white liquid, then an incisional biopsy of the lesion was performed, both at the same surgical time.
The histopathological study identified fragments of the capsule made up of lax fibrous tissue, which is mostly lined by stratified squamous epithelium of more or less uniform thickness of six to eight layers thick, with a parakeratinized wavy surface and a cuboidal to columnar basal layer that in multiple areas is detached from the capsule (Figure 1. D). The result of the histopathological study was: Odontogenic Keratocyst.
The design of the digital cannula was performed, first the DICOM format file of the patient’s CT scan was obtained, then in Blender software, the decompression cannula with a diameter of 0.5cm and a length of 2.5cm was designed, and then the 3D model was extracted in the form of STL data on the Formlabs Form 2™ 3D printer (Formlabs Ohio Inc., Millbury, OH, USA). Medical grade resin with the trade name Biomed Clear™ (Product Code: FLBMCL01) from Formlabs (Formlabs Ohio Inc., Millbury, OH, USA) was used for the cannula impression (Figure 2).
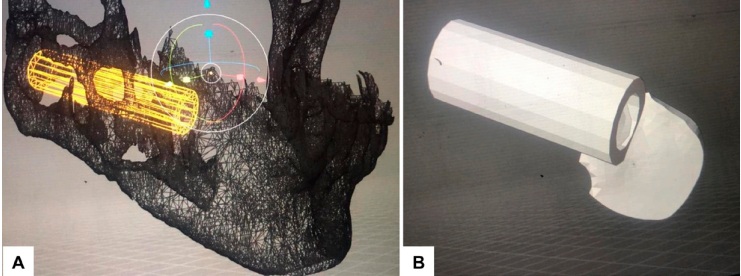
Figure 2 Virtual planning. A. Three-dimensional reconstruction of the mandible with custom-designed cannula. B. Cannula for keratocyst decompression
The treatment consisted of decompressing the cystic lesion with a custom-printed cannula for subsequent enucleation. An incision was made in the anterior border of the mandibular ramus and extended to the first molar, subsequently the second permanent molar was extracted, since it presented grade III dental mobility, due to bone loss. The cyst lumen was accessed and the 3D-printed cannula was placed and fixed with two 1.5 system screws to the remaining corticals. The lumen of the cannula was irrigated with 0.9% sodium chloride solution (NaCL) (Figure 3).
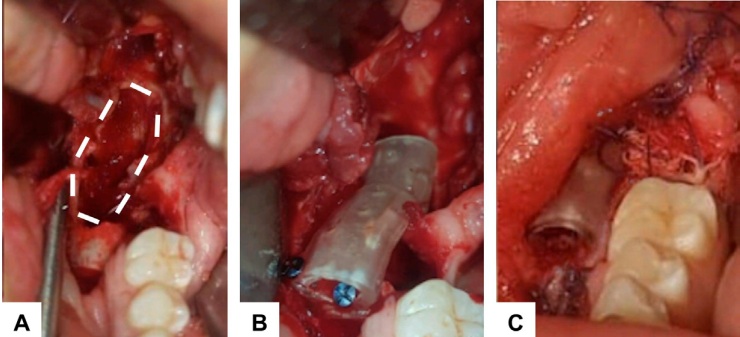
Figure 3 Transsurgical photographs. A. Lines show the limits of the cystic cavity. B. Cannula placement in the cyst lumen and screw fixation to the remaining bone cortex. C. Placement of 4.0 x 4.0 cm gauze embedded with 5-Fluorouracil
The patient attended follow-up appointments; in the control orthopantomograms at three months the lesion decreased in size (Figure 4. A), at nine months an increase in radiopacity was observed, with a residual radiolucent area in the mandibular body of less than three cm. At this time enucleation and curettage of the residual lesion plus peripheral ostectomy of one cm was performed, a gauze soaked with 5-fluorouracil solution was placed for 24 hours, then it was removed. It is important to mention that after decompression, a small radiolucent lesion was still observed at the level of the right coronoid process, which did not decrease in size, so coronoidectomy was also performed with a five mm margin in the same surgical time, thus eliminating the entire lesion (Figure 4. B). The final histopathological result of both samples was an odontogenic keratocyst. A control computed tomography was performed one year and eight months after the procedure, bone neoformation was observed in the mandibular body and ascending mandibular branch (Figure 4. C).
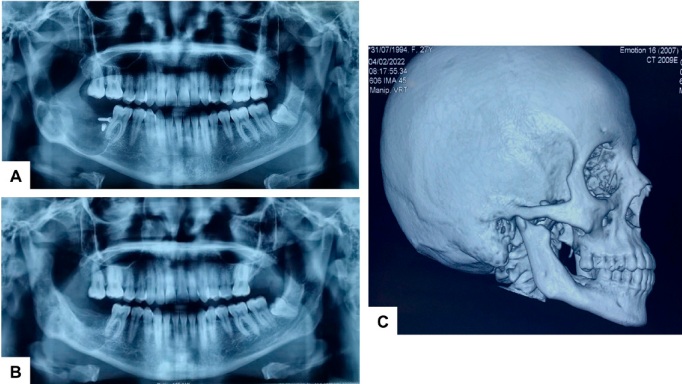
Figure 4 Control imaging studies. A. Orthopantomography at 3 months, lesion size decreases, and screws fixing the cannula to the bone are observed. B. Post-surgical orthopantomography at 9 months, there is increased radiopacity in the body, angle, and ascending mandibular branch. C. 3D reconstruction of skull computed tomography at one year and eight months, bone neoformation is observed with no data of relapse
Discussion
According to the World Health Organization (WHO) classification for odontogenic cysts and tumors, the OKC may represent a true cyst, but it is not a common cystic lesion. The lesion is distinct and requires special consideration because of its aggressive clinical behavior and high recurrence rate18. Although there is a predilection for men, in the case hereby presented it was a woman; it has been shown that when OKCs are associated with nevoid basal cell carcinoma syndrome (NBCCS) their ratio is 1:1, i.e. there is equal involvement for both men and women8. Regarding the age of the patient, it can be considered that she is within the age range most predisposed to present the lesion, which is between the second and third decade of life19, the patient was 26 years old. As for the location, it is generally located in the body and mandibular ramus, this location is the most frequently reported in the literature18,19. The characteristics related to bucco-lingual expansion, disruption of the cortical bone, and presence of septa within the lesion, in addition to the multilocular pattern8, were confirmed with orthopantomography and computed tomography.
After confirming the diagnosis of OKC by histopathological result of the incisional biopsy, the treatment was performed in two surgical stages. The first stage consisted of decompression of the lesion using a custom-designed 3D-printed cannula and odontectomy of the second molar. Although technically marsupialization and decompression are different treatments, both aim to communicate the cyst lumen with the outside to reduce its pressure, induce a change in the cyst epithelium and thus decrease the size of the lesion, decompression followed by surgical enucleation is attributed as a first line of treatment of OKC2,19.
The 3D-printed cannula was designed to be placed deep into the lesion without the risk of the lumen collapsing. Several devices have been used for decompression, including a bladder catheter fragment, Penrose tube, and intravenous or pediatric feeding catheters, all of which have shown favorable results for decompression1,19. However, the 3D printed cannula has unique advantages in that its design is precise and customized for each patient, raw material costs are low and production speed is fast16,17. However, it can be considered a disadvantage that not all surgeons are familiar with 3D technology. Biomaterials used for 3D printing can be natural or synthetic, such as polymers, as they have good physical and mechanical properties17. An example of this is Biomed Clear™, it is a biocompatible resin used for applications requiring prolonged contact with skin and mucous membranes16. It is also compatible with hospital disinfection and sterilization methods. More generally, the integration of 3D printing into different facets of contemporary dentistry has enabled the production of complex surgical devices20. Other important advantages include improved design software, marked cost reduction, and simplicity of production13.
The second molar associated with the lesion was removed due to its high degree of mobility, which conditioned a poor functional prognosis. Although there is no consensus as to whether the tooth involved in the odontogenic keratocyst should be extracted or preserved, there are studies that report that when the roots are in contact with the margins of the lesion and are preserved, they have a recurrence rate of 32.4% compared to those in which extraction is performed, whose recurrence is 3.6%21. Although these data are not conclusive as to whether or not the tooth involved in the lesion should be removed, they are important data to consider when making a decision.
In the second surgical stage, enucleation and curettage of the remaining cyst were performed along with peripheral ostectomy, plus the application of 5-fluorouracil as an adjuvant method. 5-fluorouracil is an antineoplastic drug that has been shown to induce apoptosis by inhibiting the Sonic Hedgehog (SHH) signaling pathway in the cells of the OKC22. In addition, it inhibits the enzyme thymidylate synthetase, essential for DNA synthesis; it is used as an adjuvant to enucleation, curettage, and peripheral ostectomy23,24. However, its use has not been ruled out in the early stages of OKC, or those lesions of large size. There is no standard treatment protocol for OKC treatment; with a wide spectrum of modalities, treatment is chosen according to the clinical judgment of physicians on a patient-specific basis23,25.
The coronoidectomy was also performed on the right side when it was observed that the lesion persisted in the coronoid process even after several months of treatment with decompression. In cases that do not respond to conservative management, i.e., when the size of the lesion does not regress after 6 months of decompression, these signs should be considered indicators of aggressiveness, therefore, such lesions should be treated by radical resection with margins of at least 5 mm from the radiographic edge of the lesion26.
During the follow-up of this case, there was a notable clinical improvement of the patient as the lesion volume decreased. In the imaging studies, control orthopantomograms showed increased radiopacity at the site of the lesion, and the CT scan showed clear bone neoformation with no evidence of recurrence (Figure 4. B-C). This protocol has worked favorably in multiple reports, demonstrating the efficacy of decompression by decreasing the size of the lesion and minimizing damage to neighboring tissues, thus inducing bone neoformation progressively7,19. Nevertheless, the high recurrence rate of odontogenic keratocyst should always be considered, so it is essential to follow it up periodically utilizing imaging tests9,19.
Conclusions
Several treatment modalities are available for OKC. Clinical judgment plays a key role to choose the most appropriate one. It is important to consider the size of the lesion, growth rate, and degree of tissue invasion. Initial decompression with a customized 3D-printed cannula offers accuracy and precision in the initial treatment. In lesions refractory to conservative treatment, aggressive therapies should be used because of the high recurrence rate of OKC.
Referencias bibliográficas
1. Alonso Moctezuma A, Santos Jaimes E, Zeta Castañeda E, González Alva P, Portilla Robertson J. Tratamiento con descompresión de un queratoquiste odontogénico. Rev Odont Mex. 2020; 24(2): 124-133. DOI: 10.22201/fo.1870199xp.2020.24.2.79494 [ Links ]
2. Polak K, Jedrusik-Pawlowska M, Drozdzowska B, Morawiec T. Odontogenic keratocyst of the mandible: A case report and literature review. Dent Med Probl. 2019; 56(4): 433-436. PMID: 31689015 [ Links ]
3. Forteza-López A, Sáez-Alcaide LM, Molinero-Mourelle P, Helm A, Paz-Hermoso V, Blanco-Jerez L, et al. Tratamiento del tumor odontogénico queratoquístico: revisión sistemática. Rev Esp Cir Oral y Maxilofac. 2019; 41(1): 26-32. DOI: 10.20986/recom.2019.1026/2019 [ Links ]
4. Soluk-Tekkesin M, Wright JM. The World Health Organization Classification of odontogenic lesions: A summary of the changes of the 2022 (5th) edition. Turk Patoloji Derg. 2022; 38(2): 168-184. DOI: 10.5146/tjpath.2022.01573 [ Links ]
5. Kshirsagar RA, Bhende RC, Raut PH, Mahajan V, Tapadiya VJ, Singh V. Odontogenic keratocyst: Developing a protocol for surgical intervention. Ann Maxillofac Surg. 2019; 9(1): 152-157. DOI: 10.4103/ams.ams_137_18 [ Links ]
6. Khan AA, Qahtani SA, Dawasaz AA, Saquib SA, Asif SM, Ishfaq M, et al. Management of an extensive odontogenic keratocyst: A rare case report with 10-year follow-up. Medicine. 2019; 98: 51 e17987. DOI: 10.1097/MD.0000000000017987. [ Links ]
7. Jung HD, Lim JH, Kim HJ, Nam W, Cha IH. Appropriate follow-up period for odontogenic keratocyst: a retrospective study. Maxillofac Plast Reconstr Surg. 2021; 43: 16. DOI: 10.1186/s40902-021-00301-x [ Links ]
8. Alves DBM, Tuji FM, Alves FA, Rocha AC, dos Santos-Silva AR, Vargas PA, et al. Evaluation of mandibular odontogenic keratocyst and ameloblastoma by panoramic radiograph and computed tomography. Dentomaxillofac Radiol. 2018; 47(1): 20170288. DOI: 10.1259/dmfr.20170288 [ Links ]
9. Borghesi A, Nardi C, Giannitto C, Tironi A, Maroldi R, Bartolomeo FD, et al. Odontogenic keratocyst: imaging features of a benign lesion with an aggressive behaviour. Insights Imaging. 2018; 9: 883-897. DOI: 10.1007/s13244-018-0644-z [ Links ]
10. Milani CM, Mauricio CM, Francio L, Mattos NHR. 14-Year evolution odontogenic keratocyst: Case report. Rev port estomatol med dent cir maxilofac. 2021; 62(1): 50-55. DOI: 10.24873/j.rpemd.2021.03.824 [ Links ]
11. Stoelinga PJW. The odontogenic keratocyst revisited. Int J Oral Maxillofac Surg. 2022; 51(11): 1420-1423. DOI: 10.1016/j.ijom.2022.02.005 [ Links ]
12. Ramirez Skinner H, Lai Guerrero S, Foncea Riquelme C, Solar González A, Goni Espíldora I, Vargas Díaz A. Correlación entre los hallazgos de la biopsia intraoperatoria y el estudio histopatológico definitivo en el tratamiento quirúrgico de los queratoquistes. Rev Esp Cir Oral Maxilofac. 2021; 43(4): 149-155. https://scielo.isciii.es/scielo.php?pid=S1130-05582021000400005&script=sci_arttext [ Links ]
13. Zoabi A, Redensky I, Oren D, Kasem A, Zingron A, Daoud S, et al. 3D printing and virtual surgical planning in oral and maxillofacial surgery. J Clin Med. 2022; 11(9) :2385. DOI: 10.3390/jcm11092385 [ Links ]
14. Barreda Hale M, Romero-Araya P, Cea Herrera M, Espinoza D, Castro N, Castro J, et al. Computer-assisted planning with 3D printing for mandibular reconstruction caused by a mandibular fracture with secondary osteomyelitis: A case report. Clin Case Rep. 2021; 9(7): e04410. DOI: 10.1002/ccr3.4410 [ Links ]
15. César-Juárez AA, Olivos-Meza A, Landa-Solís C, Cárdenas-Soria VH, Silva-Bermúdez PS, Suárez-Ahedo C, et al. Uso y aplicación de la tecnología de impresión y bioimpresión 3D en medicina. Rev Fac Med (Méx.) 2018; 61(6): 43-51. https://www.scielo.org.mx/pdf/facmed/v61n6/2448-4865-facmed-61-06-43.pdf [ Links ]
16. Vidakis N, Petousis M, Michailidis N, Papadakis V, Korlos A, Mountakis N, et al. Multi-functional 3D-printed vat photopolymerization biomedical-grade resin reinforced with binary nano inclusions: The effect of cellulose nanofibers and antimicrobial nanoparticle agents. Polymers (Basel). 2022; 14(9): 1903. DOI: 10.3390/polym14091903 [ Links ]
17. Wang Z, Yang Y. Application of 3D printing in implantable medical devices. Biomed Res Int. 2021: 6653967 DOI: 10.1155/2021/6653967 [ Links ]
18. Chaves FN, Fernandes JDL, França SR, Oliveira DHIP, Sampieri MBS, Carvalho FSR, et al. Conservative management of an extensive odontogenic keratocyst in the anterior region of a pediatric patient's jaw. Res Society Devel. 2021; 10(4): 14303. DOI: 10.33448/rsd-v10i4.14303 [ Links ]
19. Sánchez Sánchez J, Aguilar Maldonado J, Barreño Haro K, Jinez Zuñiga P. Odontogenic keratocyst: diagnostic characteristics and conservative surgical treatment. Int J Med Surg Sci. 2021; 8(4): 1-12. DOI: 10.32457/ijmss.v8i4.1655 [ Links ]
20. Khorsandi D, Fahimipour A, Abasian P, Saber SS, Seyedi M, Ghanavati S, et al. 3D and 4D printing in dentistry and maxillofacial surgery: Printing techniques, materials, and applications. Acta Biomater. 2021; 122: 26-49. DOI: 10.1016/j.actbio.2020.12.044 [ Links ]
21. Zhao Y, Liu B, Zhao YF. Controversies regarding the management of teeth associated with cystic lesions of the jaws. Chin J Dent Res. 2019; 22(2): 81-92. DOI: 10.3290/j.cjdr.a42512 [ Links ]
22. Hernández-Ortega OR, Malanche-Abdalá G, Salgado-Chavarría F. Terapia adyuvante con 5-fluorouracilo tópico para queratoquiste odontogénico, presentación de caso y revisión de la literatura. Rev Odont Mex. 2021; 25(3): 224-232. DOI: 10.22201/fo.1870199xp.2021.25.3.83093 [ Links ]
23. Wanve SA, Andrade NN, Venkatakrishnan L, Duro D. Comparison of the effectiveness of 5-Fluorouracil and modified Carnoy's solution in reducing the recurrence of odontogenic keratocyst. J Oral Biol Craniofac Res. 2023; 13(3): 436-441. DOI: 10.1016/j.jobcr.2023.03.007 [ Links ]
24. Caminiti M, El-Rabbany M, Jeon J, Bradlel G. 5-Fluorouracil is associated with a decreased recurrence risk in odontogenic keratocyst management: A retrospective cohort study. J Oral Maxillofac Surg. 2021; 79(4): 814-821. DOI: 10.1016/j.joms.2020.07.215 [ Links ]
25. Winters R, Garip M, Meeus J, Coropciuc R, Politis C. Safety and efficacy of adjunctive therapy in the treatment of odontogenic keratocyst: a systematic review. Br J Oral Maxillofac Surg. 2023; 61(5): 331-336. DOI: 10.1016/j.bjoms.2023.04.006 [ Links ]
26. Oginni FO, Alasseri N, Ogundana OM, Famurewa BA, Pogrel A, Al-Moraissi EA. An evidence-based surgical algorithm for management of odontogenic keratocyst. Oral Maxillofac Surg. 2023; 27(2): 201-12. DOI: 10.1007/s10006-022-01064-z [ Links ]
Received: March 01, 2023; Accepted: September 01, 2023
 Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia
Creative Commons
