










Servicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista odontológica mexicana
versión impresa ISSN 1870-199X
Rev. Odont. Mex vol.26 no.3 Ciudad de México jul./sep. 2022 Epub 23-Jul-2025
https://doi.org/10.22201/fo.1870199xp.2022.26.3.80392
Clinical case
Treatment of a Bruxism Patient with Minimally Invasive Restorations: a Case Report
1 Egresado de la Especialidad en Prostodoncia. Centro Universitario de Ciencias de la Salud. Universidad de Guadalajara.
2 Estudiante de la Especialidad en Prostodoncia. Centro Universitario de Ciencias de la Salud. Universidad de Guadalajara.
3 Profesor de la Especialidad en Prostodoncia. Centro Universitario de Ciencias de la Salud. Universidad de Guadalajara.
Introduction:
Bruxism is an oral condition associated with numerous clinical problems. It is defined as “an oral habit consisting of rhythmic or spasmodic grinding or clenching of the teeth during non-masticatory movements, which can cause occlusal trauma”.
Objectives:
To describe the follow-up of a patient with awake and sleep bruxism, with generalised loss of dental substance.
Case presentation:
Generalised loss of tooth substance associated with bruxism was diagnosed, as well as decreased vertical dimension of occlusion. The treatment was divided into 4 phases. First phase: Diagnostic models, radiographs and photographs were taken. Second phase: The wax-up was evaluated by means of a diagnostic mock-up, observing the facial harmony and patient acceptance. Third phase: The pieces were prepared, the final impression was taken, and the provisional restorations were placed, which were kept in the mouth for 2 weeks to verify the patient’s adaptation. Fourth phase: The partial restorations were cemented, and an occlusal splint was placed. The patient had a correct adaptation to the new vertical dimension of occlusion, the aesthetic, biological and functional objectives were met, and the parafunction was treated.
Conclusions:
Minimally invasive restorations prove to be a comfortable, quick and painless option that meets aesthetic, biological and functional requirements.
Keywords: Tooth wear; Bruxism; Bonded Restorations; Minimally Invasive; Lithium Disilicate
Introducción:
El bruxismo es una condición oral asociada con numerosos problemas clínicos, se define como “hábito oral que consiste en rechinar o apretar en forma rítmica o espasmódica los dientes durante movimientos no masticatorios, lo cual puede ocasionar trauma oclusal”.
Objetivos:
Presentar el seguimiento de un paciente con bruxismo de vigilia y del sueño, con pérdida de sustancia dental generalizada.
Presentación del caso:
Se diagnosticó pérdida de sustancia dental generalizada asociada a bruxismo, así como dimensión vertical de oclusión disminuida. El tratamiento se dividió en 4 fases. Primera fase: Se tomaron modelos de diagnóstico, radiografías y fotografías. Segunda fase: Se evaluó el encerado mediante una maqueta de diagnóstico observando la armonía facial y aceptación del paciente. Tercera fase: Se prepararon las piezas, se tomó impresión final y se colocaron las restauraciones provisionales, las cuales se mantuvieron 2 semanas en boca para verificar la adaptación del paciente. Cuarta fase: Se cementaron las restauraciones finales y se colocó férula oclusal. El paciente tuvo una correcta adaptación a la nueva dimensión vertical de oclusión, se cumplieron los objetivos estéticos, biológicos y funcionales y se dio tratamiento a la parafunción.
Conclusiones:
Las restauraciones mínimamente invasivas resultan ser una opción cómoda, rápida e indolora la cual cumple con los requisitos estéticos, biológicos y funcionales.
Palabras clave: Pérdida de sustancia dental; Bruxismo; Restauraciones adheridas; Mínimamente Invasiva; Disilicato de Litio
Introduction
Bruxism is an oral condition associated with numerous clinical problems, including orofacial pain, loss of tooth substance, and failure of restorative treatments. In the eighth edition of the Glossary of Prosthodontic Terms, it is defined as “an oral habit consisting of rhythmic or spasmodic grinding or clenching of the teeth during non-masticatory movements, that may cause occlusal trauma”1-3. The international consensus of experts on bruxism, published in 20184, described it in two types:
Sleep or nocturnal bruxism is masticatory muscle activity during sleep that is characterised as rhythmic (phasic) or non-rhythmic (tonic) and is neither a movement disorder nor a sleep disorder in healthy people.
Awake or diurnal bruxism is an activity of the masticatory muscles while the individual is awake that is characterised by repetitive or sustained dental contact.
An important contribution that emerges from the international consensus is to consider bruxism as a risk factor rather than a disorder in healthy people and can be associated with other clinical conditions (sleep apnoea or other sleep disorders) or symptoms (xerostomia) without a cause-and-effect relationship.
Bruxism is also differentiated by two diagnostic approaches:
1. Without instruments
Clinical features of both diurnal and nocturnal bruxism include the presence of hypertrophy of the masticatory muscle, in addition to clefts in the tongue or lip and/or a linea alba on the inside of the cheek, damage to hard dental tissues (cracked teeth), repetitive failures of prosthetic restoration work, or mechanical wear of the teeth3,5.
2. With instruments
Electromyographic (EMG) recordings can provide key evidence of bruxism, despite their limited availability. On the other hand, polysomnography is the Gold Standard for diagnosing bruxism, but we are still far from the ideal assessment of bruxism. It is necessary to collect concurrent data on possible aetiological, comorbidity and risk factors that may contribute to the presence of bruxism since it is a condition with multifactorial aetiology, that is, it can be related to various conditions such as neurodiversity (including various types of autism), neurological diseases (including environmental and traumatic causes), and the use of different medications6.
Other treatment approaches involve addressing the psychosocial component including stress reduction, behavioural counselling, lifestyle changes, and therapy. However, they must be accompanied by occlusal splints that promote occlusal stability6.
One of the main signs of bruxism is the loss of tooth substance, which has become a fairly common pathology. Its aetiology is multifactorial. It can be caused by chemical processes, erosion, excessive attrition and abrasion, or even a combination of these7-9. Turner & Missirilian 198410 defined 3 categories in patients with loss of tooth substance: Category one: excessive loss of tooth substance with loss of vertical dimension of occlusion (VDO). For which a facial and phonetic analysis must be performed, and once the new dimension has been determined and placed, it must be tested for at least 2 weeks before the final restorations to see the patient’s adaptability. This increase will provide space and promote less invasive restorations11, Category two: loss of tooth substance, without loss of VDO with available space. Not all patients who present dental wear patterns present loss of vertical dimension due to compensatory eruption, and finally, Category three: loss of tooth substance without loss of VDO with limited space10.
Once diagnosed, it must be assessed whether the patient should be treated. First, the amount of lost dental tissue must be observed (<1/3 of the crown must be restored) and confirm whether it is localised or generalised. The development of new materials in combination with advances in adhesion has allowed clinicians to adopt a more conservative way, in which the dental remnant is worn in minimal amounts, avoiding traditional retentive preparations that required greater dental wear12. In minimally invasive dentistry, the selection of restorative material is of utmost importance. Over time, direct and indirect resins, metal alloys and different ceramics have been used, taking care of adhesive techniques since, if there is a great loss of tooth substance, the dentin tissue will be exposed13-16.
Below, the case of a 60-year-old male patient with awake and sleep bruxism, diagnosed by a questionnaire and clinical examination, is presented. It has generalised loss of tooth substance, it is placed in category one of Turner & Missirilian, due to the need to increase the VDO.
Clinical case presentation
A 60-year-old male patient with the next reason of consultation: “I need lots of fixes”, reported being a type II diabetic, on metformin treatment. Extraoral analysis showed a mesocephalic facial biotype. The interpupillary line coincides with the intercommissural line. The facial midline showed harmony. The upper facial third is diminished while the middle and lower third are equivalent. The lower facial third is 2 times larger than the upper third and is symmetrical, which complies with the standard aesthetic analysis values (Table 1, Figure 1A). The patient presents nocturnal and diurnal bruxism with multifactorial aetiology.
Table 1 Fradeani Aesthetic Analysis measurements
| Measurement | Value | Standard |
|---|---|---|
| Profile | 176º | 170º |
| Nasolabial angle | 108º | 90-95º |
| Line E | lips from behind | lips from behind |
| Upper lip length | 22 mm | 20-22 mm |
| Dental exposure at rest | -0.2 mm | -0.04 mm |
| Lower lip curvature | Does not coincide with dental curvature |
It must coincide with dental curvature |
| Facial and dental midline | Coincident | Coincident |
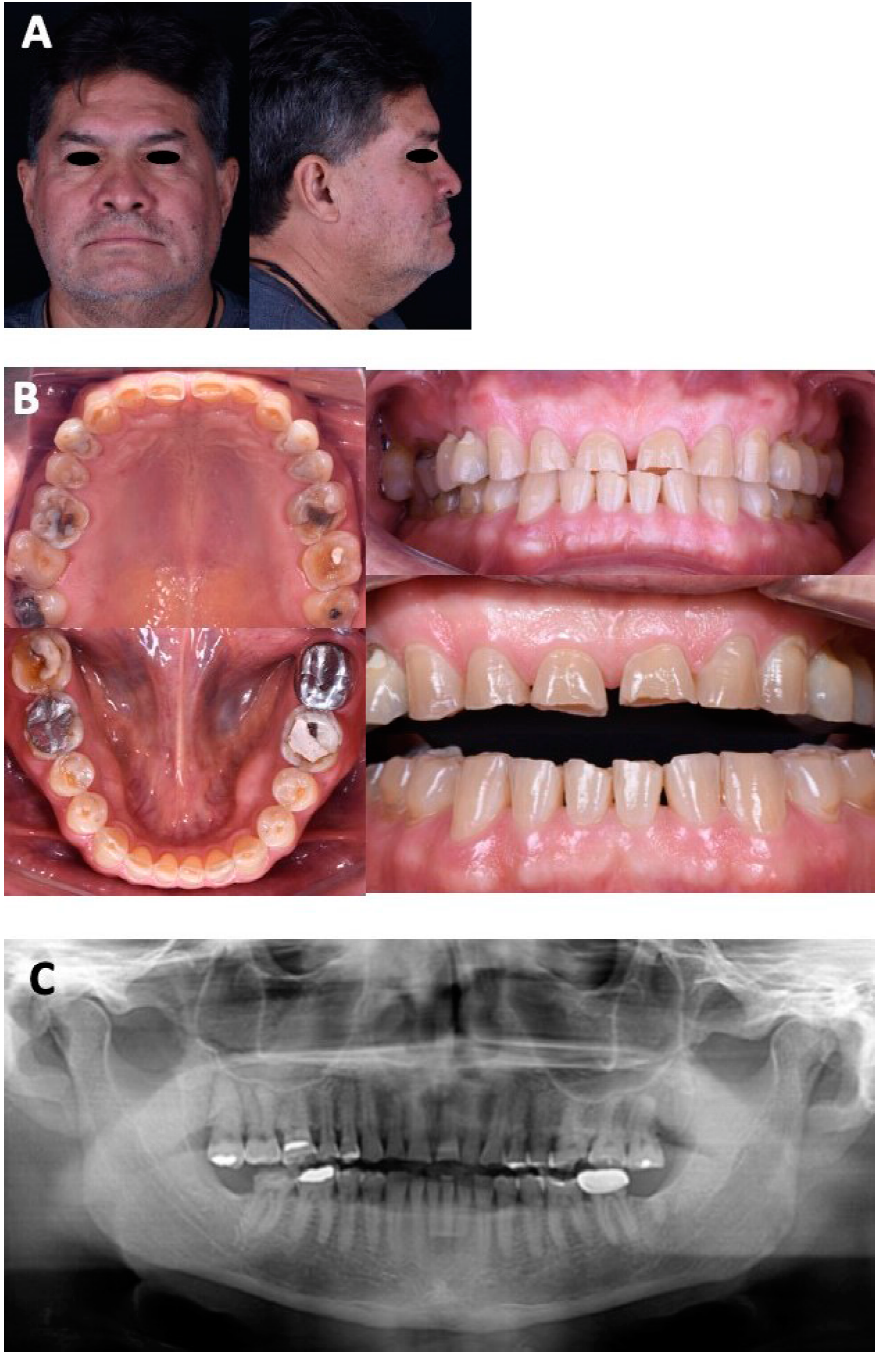
Figure 1 Initial studies. A. Initial facial photographs from the front and profile view. B. Initial intraoral photographs. C. Orthopantomography.
Intraoral analysis showed square arches in both arches and the presence of mandibular torus, a wide band of generalised keratinised gingiva in all sextants. In the maxillary arch, root exposure of teeth 17, 16, 15, 14, 26 and 27 was observed, besides defective restorations in teeth 14-18, and 24-28, loss of dental substance in all teeth including the anterior sector, emphasising abfractions on teeth 24 and 25.
Defective restorations were identified in teeth 35-37, 46 and 47, in addition, loss of dental substance in all teeth of the mandibular arch, highlighting the abfractions of the 4 premolars (Figure 1B). Orthopantomography showed patent maxillary sinuses and correct root parallelism, absence of teeth 38 and 48, and absence of bone ridges (Figure 1C).
In the occlusal analysis, were observed the canine relationship and Class I molar, 1 mm overbite and 1 mm overjet, VDO 61 and vertical dimension at rest (VDR) 66, the interocclusal free space is 5 mm and the discrepancy between maximum intercuspation and centric relationship is 0.5 mm (Figure 2A).

Figure 2 Analysis of the models and occlusal splint. A. Analysis of the models, overbite (molar and canine classification). B. Manufacturing procedure for a 3.5 mm occlusal splint to determine adaptation to the new vertical dimension of occlusion.
The treatment objectives were to place 28 lithium disilicate restorations in all teeth to replace the decreased VDO, complying with aesthetic, biological and functional principles, along with treatment for parafunction.
By means of diagnostic waxing, it was decided to increase the VDO by 3.5 in the articulator stem, providing adequate space for the restorative material and leaving an interocclusal clearance of 1.5 mm. Subsequently, an occlusal splint with a height of 3.5 mm was made (Figure 2B), and the patient used it for 3 months. We began by removing defective restorations and carious lesions (Figure 3A) in which resin coating was placed, for which selective etching, self-conditioning adhesive (3MTM Single Bond Universal Adhesive, 3M ESPE Deutschland GmbH, Germany) and fluid resin A1 shade (3MTM FiltekTM Z350 XT Universal Restorative, 3M ESPE Deutschland GmbH, Germany) were used (Figure 3B). Once the patient confirmed the adaptation to the new VDO, the waxing was tested in the mouth using a mock up (3MTM ProtempTM Plus Temporization Material, 3M ESPE Deutschland GmbH, Germany), where the following were evaluated: aesthetics, phonetics, occlusal plane, buccal corridors, occlusion, anterior disocclusions and patient acceptance (Figure 4A). Finally, the teeth were prepared using the prognostic model based on wax-up to avoid further wear of the pieces and preserving space for the restorative material. The preparations consisted of a complete crown of tooth 37 with a knife-edge finish, occlusal veneers with long bevels on teeth 17, 16, 15, 25, 26, 27, 36, 46 and 47, vonlays on 14, 24, 35, 34, 44 and 45 together with vestibular veneers on mandibular anterior teeth and vertical full crown preparation on maxillary anterior teeth. All restorations were made with the “Cut Back” technique on vestibular veneers and vonlays (IPS e.max Press HT, Ivoclar Vivadent AG, Principality of Liechtenstein) while the rest of the restorations were made up. At the time of cementation, occlusal veneers were conditioned with 9.5% weak hydrofluoric acid gel (Porcelain Etchant, BISCO, Inc., Schaumburg, Illinois, USA) for 20 seconds, washed, 35% phosphoric acid (K-ETCHANT Syringe, Kuraray Noritake Dental Inc., Niigata, Japan) was applied with 60 seconds of friction to remove residues, followed by a 20-second wash. They were dried and silane (Porcelain Primer/Bis-SilaneTM, BISCO, Inc., Schaumburg, Illinois, USA) was placed and allowed to dry for 60 seconds. Subsequently, Universal adhesive (ClearfilTM Ceramic Primer Plus, Kuraray Noritake Dental Inc., Niigata, Japan) and dual cement (PanaviaTM V5, Kuraray Noritake Dental Inc., Niigata, Japan) were applied.

Figure 3 Removal of carious and defective lesions. A. Maxillary and mandibular arch with caries and defective restorations. B. Maxillary and mandibular arch after removal of caries and defective restorations.
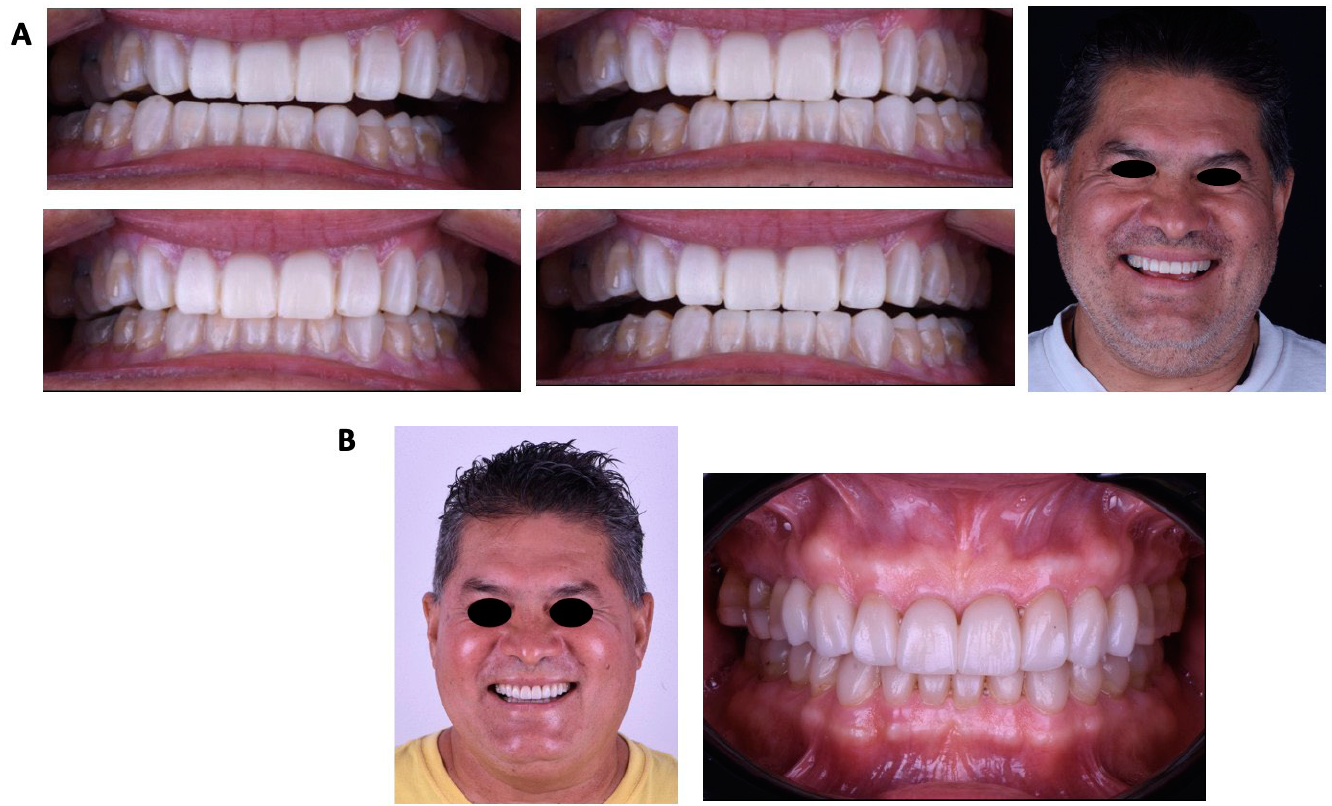
Figure 4 Diagnostic model test and final photographs. A. Test of the wax-up using a diagnostic model to corroborate the organic occlusion and assess aesthetics. B. Final photographs: extraoral smile and intraoral front view.
Regarding the conditioning of the teeth, they were sandblasted with 30-micron aluminium oxide, the surface was cleaned, the enamel was etched with 37% phosphoric acid for 15 seconds, it was washed and adhesive was applied (ClearfilTM Universal Bond Quick, Kuraray Noritake Dental Inc., Niigata, Japan). As for the restorations of vestibular veneers and vonlays, fluid resin was used for cementation due to their thickness, improving colour stability and longer working time. The protocol for conditioning the restorations was the same: only the dual cement was replaced by fluid resin A1 shade, the restoration was brought to the mouth, light photopolymerization began, excess was removed and each surface was subsequently photocured for 20 seconds (Figure 4B).
Finally, the occlusion was verified with articular paper, premature contacts were eliminated, and the occlusal splint was delivered. As a result, the objectives were achieved by placing 28 restorations that returned the decreased VDO with characteristics of organic occlusion and facial harmony, as well as parafunction treatment using an occlusal splint.
Discussion
Due to diet, intake of carbonated drinks and acidic substances, it is increasingly common to find dentures with loss of tooth substance and even more so in combination with parafunctions such as bruxism. Previously, teeth were usually restored by means of complete crowns, which implied the loss of additional structure, coupled with the biological implications; for example, loss of pulp vitality or the need to perform crown lengthening17. A patient who receives complete rehabilitation at an early age will need several restorations throughout their life, each of which leads to loss of tooth structure18. For this reason, it is imperative to delay the restorative cycle until older ages. Once the piece has been prepared for a complete crown, the only re-treatment will be to continue placing the crown until it no longer works. Thanks to current adhesive techniques, it is possible to offer patients less invasive alternatives for the treatment of exposed dentin. Many authors19-23 have published about treatments performed with occlusal veneers, vonlays or different types of partial restorations adhered with thicknesses of up to 1 mm made of different ceramics, including resins. That is, when a tooth is treated with partial adhesion restorations and these fail, most of the time a similar restoration can be performed again with minimal wear on the remaining structure and postpone the complete crown until the end. These treatments have been successful for 20 years, which are reduced when root canal treatment is presented. It is an option that cannot be ruled out, and at the same time, should not be the first choice in a young patient.
As for the material, although direct resins have had a correct biomechanical development, as shown in a retrospective study by Bartlett & Varma24 in which a success rate of 83% of the restorations stands out, they also mention that greater maintenance and experience of the professional/specialist are required to reduce the range of complications. Ceramic occlusal veneers have several advantages in terms of abrasion resistance, biocompatibility, and colour stability, in contrast to resin occlusal veneers. In a study by Magne et al.25, it was shown that lithium disilicate with a thickness of 1.2mm in the centre and 1.8mm in the cusp area has a survival rate of 80% with loads of 1000N, remembering that in posterior teeth the masticatory loads range between 500 and 800N.
Moreira et al.26 describe a clinical case of complete adhesive rehabilitation performed with lithium disilicate in a patient with bruxism, who did not have biological or prosthetic complications after 4 years. In the same year, Malchiodi27 conducted an observational study in which he evaluated 43 lithium disilicate adhesive restorations in 8 different patients and had a success rate of 97.7% at 32 months of follow-up with thicknesses from 0.5mm to 2mm.
Although several authors have described clinical cases of patients with severe wear resolved by adhesive lithium disilicate restorations, long-term follow-ups are still necessary28,29.
Conclusions
Treatment for generalised loss of tooth substance carried out with minimally invasive restorations turns out to be a comfortable, quick and painless option, which involves less biological sacrifice of the teeth. The chosen material promotes adequate hygiene and meets the aesthetic, biological and functional requirements. Finally, it is imperative to manage the risk factor that bruxism represents for the success of restorations.
REFERENCES
1. The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94(1):10-92. DOI: 10.1016/j.prosdent.2005.03.013 [ Links ]
2. American Academy of Sleep Medicine. International classification of sleep disorders: Diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005. [ Links ]
3. Lobbezoo F, Ahlberg J, Glaros AG, Kato T, Koyano K, Lavigne GJ, et al. Bruxism defined and graded: an international consensus. J Oral Rehabil. 2013; 40(1):2-4. DOI: 10.1111/joor.12011 [ Links ]
4. Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros AG, Kato T, et al. International consensus on the assessment of bruxism: Report of a work in progress. J Oral Rehabil. 2018; 45(11):837-844. DOI: 10.1111/joor.12663 [ Links ]
5. Slade GD, Spencer AJ. Development and evaluation of the Oral Health Impact Profile. Community Dent Health. 1994; 11(1):3-11. https://europepmc.org/article/med/8193981 [ Links ]
6. Goldstein RE, Clark WA. The clinical management of awake bruxism. J Am Dent Assoc. 2017; 148(6):387-391. DOI: 10.1016/j.adaj.2017.03.005 [ Links ]
7. Bahillo J, Jané L, Bortolotto T, Krejci I, Roig M. Full-mouth composite rehabilitation of a mixed erosion and attrition patient: a case report with v-shaped veneers and ultra-thin CAD/CAM composite overlays. Quintessence Int. 2014; 45(9):749-56. DOI: 10.3290/j.qi.a32439 [ Links ]
8. Fradeani M, Barducci G, Bacherini L. Esthetic rehabilitation of a worn dentition with a minimally invasive prosthetic procedure (MIPP). Int J Esthet Dent. 2016; 11(1):16-35. [ Links ]
9. Schlichting LH, Maia HP, Baratieri LN, Magne P. Novel-design ultra-thin CAD/CAM composite resin and ceramic occlusal veneers for the treatment of severe dental erosion. J Prosthet Dent. 2011; 105(4):217-26. DOI: 10.1016/S0022-3913(11)60035-8. [ Links ]
10. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984; 52(4):467-74. DOI: 10.1016/0022-3913(84)90326-3 [ Links ]
11. Ammannato R, Ferraris F, Marchesi G. The “index technique” in worn dentition: a new and conservative approach. Int J Esthet Dent. 2015; 10(1):68-99. https://pubmed.ncbi.nlm.nih.gov/25625128/ [ Links ]
12. Nam J, Tokutomi H. Using zirconia-based prosthesis in a complete-mouth reconstruction treatment for worn dentition with the altered vertical dimension of occlusion. J Prosthet Dent. 2015; 113(2):81-85. DOI: 10.1016/j.prosdent.2014.08.001 [ Links ]
13. Loomans B, Opdam N, Attin T, Bartlett D, Edelhoff D, Frankenberger R, et al. Severe tooth wear: European consensus statement on management guidelines. J Adhes Dent. 2017; 19(2):111-119. DOI: 10.3290/j.jad.a38102 [ Links ]
14. Wetselaar P, Lobbezoo F. The tooth wear evaluation system: a modular clinical guideline for the diagnosis and management planning of worn dentitions. J Oral Rehabil. 2016; 43(1):69-80. DOI: 10.1111/joor.12340 [ Links ]
15. Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 3. Active restorative care 2: the management of generalised tooth wear. Br Dent J. 2012; 212(3):121-127. DOI: 10.1038/sj.bdj.2012.97 [ Links ]
16. Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012; 212(4):169-177. DOI: 10.1038/sj.bdj.2012.137 [ Links ]
17. Varma S, Preiskel A, Bartlett D. The management of tooth wear with crowns and indirect restorations. Br Dent J. 2018; 224(5):343-347. DOI: 10.1038/sj.bdj.2018.170 [ Links ]
18. Vailati F, Vaglio G, Belser UC. Full-mouth minimally invasive adhesive rehabilitation to treat severe dental erosion: a case report. J Adhes Dent. 2012; 14(1):83-92. DOI: 10.3290/j.jad.a21852 [ Links ]
19. Grandon F, Marcus N, Muster M. Esthetic rehabilitation with ultra-thin ceramic veneers and direct mock-up in the treatment of dental erosion - Case report. J Oral Res. 2018; 7(6):254-259. DOI: 10.17126/joralres.2018.053 [ Links ]
20. Vailati F, Carciofo S. Treatment planning of adhesive additive rehabilitations: the progressive wax-up of the three-step technique. Int J Esthet Dent. 2016; 11(3):356-377. [ Links ]
21. Tirlet G, Crescenzo H, Crescenzo D, Bazos P. Ceramic adhesive restorations and biomimetic dentistry: tissue preservation and adhesion. Int J Esthet Dent. 2014; 9(3):354-368. [ Links ]
22. Imburgia M, Canale A, Cortellini D, Maneschi M, Martucci C, Valenti M. Minimally invasive vertical preparation design for ceramic veneers. Int J Esthet Dent. 2016; 11(4):460-471. [ Links ]
23. Schlichting LH, Resende TH, Reis KR, Magne P. Simplified treatment of severe dental erosion with ultrathin CAD-CAM composite occlusal veneers and anterior bilaminar veneers. J Prosthet Dent. 2016; 116(4):474-482. DOI: 10.1016/j.prosdent.2016.02.013 [ Links ]
24. Bartlett D, Varma S. A retrospective audit of the outcome of composites used to restore worn teeth. Br Dent J. 2017; 223(1):33-36. DOI: 10.1038/sj.bdj.2017.583 [ Links ]
25. Magne P, Schlichting LH, Maia HP, Baratieri LN. In vitro fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers. J Prosthet Dent. 2010; 104(3):149-57. DOI: 10.1016/S0022-3913(10)60111-4 [ Links ]
26. Moreira A, Freitas F, Marques D, Caramês J. Aesthetic rehabilitation of a patient with bruxism using ceramic veneers and overlays combined with four-point monolithic zirconia crowns for occlusal stabilization: A 4-year follow-up. Case Rep Dent. 2019; 2019:1640563. DOI: 10.1155/2019/1640563 [ Links ]
27. Luciano M, Francesca Z, Michela S, Tommaso M, Massimo A. Lithium disilicate posterior overlays: clinical and biomechanical features. Clin Oral Investig. 2020; 24(2):841-848. DOI: 10.1007/s00784-019-02972-3 [ Links ]
28. Dallari G, Scalzo I, Rosati RM, Sampaio CS, Hirata R. Full-mouth adhesive rehabilitation of a severe case of erosion treated with v-shaped veneers. J Esthet Restor Dent. 2021; 33(3):422-431. DOI: 10.1111/jerd.12693 [ Links ]
29. Koubi S, Gurel G, Margossian P, Massihi R, Tassery H. A simplified approach for restoration of worn dentition using the full mock-up concept: Clinical case reports. Int J Periodontics Restorative Dent. 2018; 38(2):189-197. DOI: 10.11607/prd.3186 [ Links ]
Received: August 01, 2021; Accepted: November 01, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
