Casos clínicos
Anterior Crossbite Correction with Self-Ligating System. Case Report

-
Publication dates-
August 08, 2025
Apr-Jun , 2022
- Article in PDF
- Article in XML
- Automatic translation
- Send this article by e-mail
- Share this article +
Abstract
Introduction:
Anterior crossbite is one of the most common problems in growing patients with class III malocclusion, both skeletal and functional. The correct diagnosis of this malocclusion is key to its correction and a good treatment plan.
Objectives:
obtain class I canine, maintain class I molar, obtain correct anterior guidance, maintain profile and improve function.
Case presentation:
A 13-year-old male patient comes to the clinic with the following reason for consultation: “my teeth are crooked and my jaw has moved forward”. Class III Skeletal due to a retruded maxilla, straight dolichofacial profile, , class I molar, canine class not established, canines 13, 23 and 33 retained, anterior crossbite. Treatment with “3M™ Unitek™ Gemini SL Self-Ligating Brackets MBT 0.022” brackets, lingual arch and transpalatal arch, bite lifting through build-ups on mandibular first molars, alignment and levelling phase, occlusion detailing and final retention (upper and lower removable) . The anterior crossbite was corrected by obtaining adequate anterior guidance and good chewing function. The profile and class I molar were maintained.
Conclusions:
treatment with self-ligating brackets is a good option to achieve correction of anterior crossbite, as long as a correct diagnosis and treatment plan is made.
Keywords::
anterior crossbite, self-ligation system, class III
Introduction
Patients with Class III malocclusion are considered the most complex cases to treat orthodontically, mainly due to their unpredictable nature and the unfavourable growth of those with this skeletal pattern1,2. Class III aetiology is multifactorial, genetics play an important role in its development, being a polygenic transmission not sex-linked3. Some studies mention that the frequency of this condition differs according to the geographical area and the population under study; in a population of Mexican Americans, a prevalence of 8.3% was found3. There are different characteristics that these patients may present, such as: maxillary retrognathism, mandibular prognathism or a combination of both, reverse bite, anterior and buccal crossbite, proclination of maxillary incisors and retroclination of mandibular incisors1.
-
1Treatment of Class III Malocclusion in an Adolescent with Banded RPE/Face Mask and Self-Ligating SystemUIP Health Med, 2016
-
2The Effectiveness of Protraction Face Mask Therapy: A Meta-AnalysisAm J Orthod Dentofacial Orthop, 1999
-
3Maloclusión Clase IIISalud en Tabasco, 2010
-
3Maloclusión Clase IIISalud en Tabasco, 2010
-
1Treatment of Class III Malocclusion in an Adolescent with Banded RPE/Face Mask and Self-Ligating SystemUIP Health Med, 2016
Focusing specifically on one of these characteristics, we find that the term anterior crossbite is used to describe an anomaly of occlusion in the anteroposterior plane where the mandibular teeth are in front of the maxillary teeth, which can have different aetiologies, these can be of functional or skeletal origin4. There is also pseudoclass III, which is identified as an anterior crossbite that develops as a result of mandibular displacement. The reported prevalence of anterior crossbite varies between 2.2% and 12%, depending on the age of the children and their ethnic origin5. Currently the optimal timing of treatment for orthodontic problems remains one of the most controversial issues in this field, especially for the correction of Class III malocclusion6. There are reports in the literature that suggest treatments for the correction of anterior crossbite, which include different appliances, both fixed and removable with heavy intermittent forces (inclined bite plane, tongue blade) or light continuous forces (removable appliance with auxiliary springs). However, solid evidence supporting any treatment technique is lacking5,7. One of the reported treatment options is the use of a self-ligating system, because it has many advantages over traditional brackets and is a good orthodontic treatment option for certain cases in need of slight expansion and mild to moderate crowding8.
-
4Tratamiento temprano de la mordida cruzada anterior. Revisión de la literatura/Early Treatment of Anterior Cross Bite. A Literature ReviewRev. estomatol. salud, 2011
-
5Early Treatment of Anterior Crossbite Relating to Functional Class IIIEmerging Trends in Oral Health Sciences and Dentistry, 2015
-
6Early Treatment for Class III MalocclusionJ Orthod, 2016
-
5Early Treatment of Anterior Crossbite Relating to Functional Class IIIEmerging Trends in Oral Health Sciences and Dentistry, 2015
-
7Early Correction of Anterior Crossbites: A Systematic ReviewJ Orthod, 2011
-
8Sistemas de autoligado. Caso clínicoOdontología Vital, 2017
A clear understanding of the factors involved in the development of anterior crossbites is fundamental for their timely treatment, and differential diagnosis is the key to planning treatment in accordance with the complexity of anterior crossbite4. The following clinical case shows the treatment of a patient with a Class III malocclusion with anterior crossbite and included canines. The treatment included the placement of self-ligating appliances and placement of build-ups on molars to correct the crossbite, as well as including the canines in the arch by traction.
-
4Tratamiento temprano de la mordida cruzada anterior. Revisión de la literatura/Early Treatment of Anterior Cross Bite. A Literature ReviewRev. estomatol. salud, 2011
Clinical case presentation
A 13-year-old male patient came to the orthodontic clinic with the following reason for consultation: “my teeth are crooked and my jaw has moved forward”. In his medical history he referred a syndrome that could not be diagnosed because the studies carried out did not reveal any problems. In addition to asymmetric septal hypertrophic heart disease, for which he takes propanolol, and renal tubular acidosis, for which he ingests sodium bicarbonate. He presented a normal respiratory pattern and mentioned not having operations and poor diction, for which he attended speech therapy, with much improvement.
Facially, he had a straight profile, square face, symmetrical thirds, everted lower lip, enlarged middle fifth, large and broad nose, flat chin, medium smile, 100% of the mandibular teeth and closed nasolabial angle (Figure 1A). Intraorally he had Class I molar, Class I canine not established, permanence of teeth 63, 13, 23 and 33 retained, anterior crossbite, overbite 5 mm, overjet -3 mm, Spee’s curvature 1 mm, ovoid maxillary and mandibular arch form, severe maxillary crowding (-11 mm), mild mandibular crowding (-1.2 mm), upper and lower midline deviated to the right and left respectively, retruded maxillary incisors, protruded and proclined mandibular incisors (Figure 1B).
Thumbnail
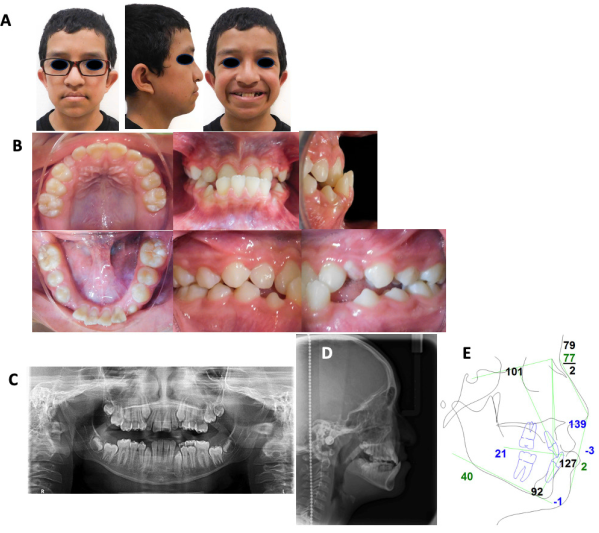
Figure 1
Initial studies. A. Extraoral photographs. B. Intraoral photographs, showing the level of crowding, anterior crossbite, overjet and overbite. C. Orthopantomography. D. Lateral cranial radiography. E. Initial Steiner cephalometric tracing performed in Dolphin Imaging Software version 11.0.
Initial studies. A. Extraoral photographs. B. Intraoral photographs, showing the level of crowding, anterior crossbite, overjet and overbite. C. Orthopantomography. D. Lateral cranial radiography. E. Initial Steiner cephalometric tracing performed in Dolphin Imaging Software version 11.0.
Orthopantomography shows the retained right canine due to lack of space, good bone level and immature apices of canines, premolars and molars. Permeable nasal sinuses and nasal turbinates, symmetrical condyles and gonial angles. Maxillary and mandibular third molar germs present (Figure 1C). Vertical growth pattern, incipient dolichofacial, Class lll skeletal by a retruded maxilla (Figure 1D). Steiner cephalometric analysis measurements were performed with Dolphin Imaging Software version 11.0 (Dolphin Imaging, Chatsworth, CA) in which we can observe the inclinations of the incisors and the skeletal discrepancy (Figure 1E). Functionally without alterations or joint pain (Table 1).
Table 1
Values of the Steiner cephalometric tracing before and after treatment.
Values of the Steiner cephalometric tracing before and after treatment.
| Standard | Initial patient | Final patient | |
|---|---|---|---|
| SNA | 82º | 72º | 74º |
| SNB | 80º | 74º | 77º |
| ANB | 2º | -2º | -3 |
| GO-GN-SN | 32º | 40º | 39º |
| SN-Occlusal Plane | 14º | 23º | 15º |
| Inc Superior- NA | 22º | 22º | 42 |
| Inc Superior-NA Seg | 4 mm | 4 mm | 8 mm |
| Upper Inc-PlaneS-N | 103º | 100º | 117º |
| Lower Inc-NB | 25º | 29º | 23º |
| Lower Inc-NB sec | 4 mm | 4 mm | 4 mm |
| Lower Inc-Mandibular Plane | 90º | 97º | 88º |
| Interincisal | 131º | 124º | 116º |
The aim of the treatment was to obtain Class I canine, maintain Class I molar, obtain correct anterior guidance, maintain profile and improve function. The possibility of orthognathic surgery was discussed in order to achieve maxillomandibular advancement, in conjunction with orthodontic treatment, and thus correct the skeletal discrepancy, improve facial aesthetics as well as establish ideal occlusion. Nevertheless, the patient rejected this alternative due to the surgical risks and his financial restrictions, therefore, non-surgical treatment alternatives were chosen.
Orthodontic treatment using non-extraction camouflage, maxillary arch expansion and protraction of the maxillary anterior teeth, using fixed orthodontic appliances, was the alternative chosen. The use of a self-ligating bracket system was chosen, since some studies have reported that the self-ligating system produces a significant increase in the maxillary transverse dentoalveolar width and results in a greater maxillary intermolar width than the conventional ligation system9.
-
9Camouflage Treatment of Skeletal Class III Malocclusion in an Adult Cleft-Palate Patient Using Passive Self-Ligating SystemAm J Orthod Dentofac Orthop, 2019
The treatment plan consisted of placing “3M™ Unitek™ Gemini SL Self-Ligating Brackets MBT 0.022” brackets, bands on maxillary and mandibular first molars with double tube and upper and lower lingual boxes. It began by placing lingual arch and transpalatal arch (TPA), build-ups on teeth 16 and 26, upper brackets with 0.016” heat activated (HA) archwire and lower brackets with 0.014” nitinol archwire; the following month the upper arch was changed for a 0.014” leftover steel arch to proclinate the maxillary incisors. Subsequently, a 0.016” x 0.022” steel arch, open coil between teeth 12 and 14 (Figure 2A) and ¼ 2.5 oz class III elastics were placed in the maxillary arch.
Thumbnail

Figure 2
Treatment progress. A. Placement of springs and build-ups. B. Intraoral photographs showing the beginning of traction on tooth 13 with a button and a flexible archwire.
Treatment progress. A. Placement of springs and build-ups. B. Intraoral photographs showing the beginning of traction on tooth 13 with a button and a flexible archwire.
Once the space was obtained and tooth 23 began to erupt, traction began. An ulectomy was performed to uncover tooth 13 and a button, 0.016” upper steel archwire and a 0.014” nitinol accessory archwire were placed, since it was in supra-occlusion, and it was not desired that the adjacent teeth suffer unwanted movements (Figure 2B). After two months, the bracket on tooth 23 and a 0.016” nitinol archwire were placed. When it was in a better position, the bracket on tooth 13 and 0.016” HA archwires were placed. The sequence of 0.016” x 0.022” HA arches in the maxilla and 0.017” x 0.025” nitinol in the mandible was continued and the build-ups were worn. The maxillary and mandibular teeth 6 were ligated (ligated 6 to 6) with a 0.018” x 0.025” upper and lower nitinol archwire (Figure 3A), box elastics were placed on ¼ 3.5 oz premolars to settle the bite. Orthopantomography was indicated (Figure 3B) and brackets for canines and first premolar of the maxilla and mandible were repositioned with 0.016” HA upper and lower archwires. A chain from maxillary teeth 3 to 3 was placed.
Thumbnail
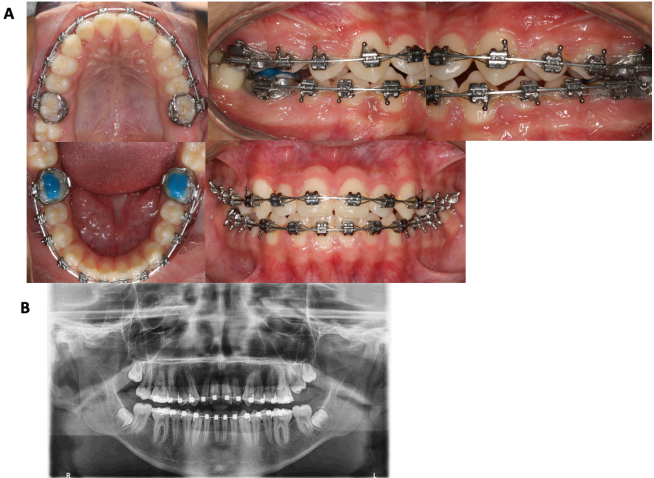
Figure 3
treatment progress. a. 0.018” x 0.025” nitinol archwire and ligation of teeth 6 to 6. b. advance orthopantomography for repositioning of maxillary and mandibular canine and first premolar brackets.
treatment progress. a. 0.018” x 0.025” nitinol archwire and ligation of teeth 6 to 6. b. advance orthopantomography for repositioning of maxillary and mandibular canine and first premolar brackets.
Subsequently, the upper and lower brackets were removed and an upper circumferential appliance and lower aligner were fitted. Extraorally, the patient’s straight profile was maintained (Figure 4A). Class I canine and Class I molar were obtained (Figure 4B). The anterior crossbite was corrected, obtaining adequate anterior guidance and good masticatory function. In the orthopantomography the included third molars were observed, so indications for extraction were given (Figure 4C). In the lateral skull radiography, as well as in the Steiner cephalometric tracing, the maxillary anterior teeth are observed proclined and the mandibular anterior teeth to be retroclined due to the compensation that was performed to correct the anterior crossbite (Figure 4D-E). Figure 4F shows the changes obtained in the superimposition of the Steiner cephalometric tracing. Referral to the extraction of third molar with the maxillofacial surgeon.
Thumbnail
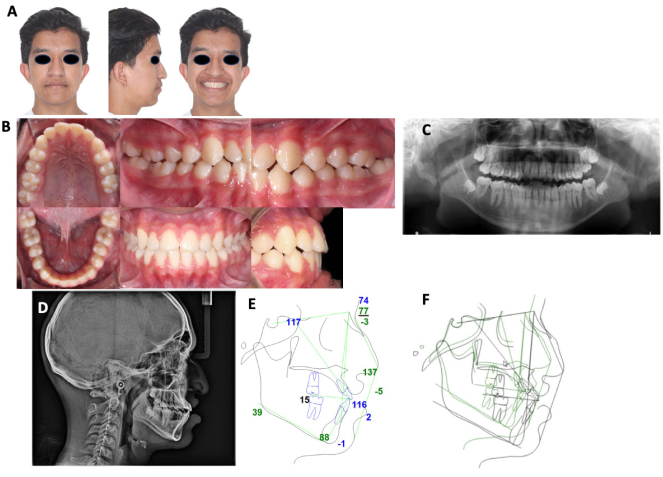
Figure 4
Final studies A. Extraoral photographs. B. Intraoral photographs and canine guidance. C. Orthopantomography. D. Final lateral cranial radiography. E. Steiner cephalometric tracing. F. Superimposition.
Final studies A. Extraoral photographs. B. Intraoral photographs and canine guidance. C. Orthopantomography. D. Final lateral cranial radiography. E. Steiner cephalometric tracing. F. Superimposition.
Discussion
The incidence of anterior crossbite in children is considerably high. Amarilis et al. reported 9.2% of school-age children affected by this malocclusion, slightly predominating of males among the affected individuals. These results coincide with the age and sex of our patient, whose treatment achieved total correction of the anterior crossbite, as reported by these authors10.
-
10Mordida cruzada anterior y tratamiento en la atención primaria Crossbite and Treatment in Primary Health CareRev Ciencias Médicas, 2016
Kanas et al. make a classification of Class III malocclusion, in which they suggest the type of treatment necessary and the ages at which its correction is most predictable. The types of treatment for Class III malocclusion that were conclusively identified were: 1) early orthodontics; 2) early combined orthodontics and orthopedics; and 3) combined orthodontics and orthognathic surgery. According to Kanas et al. the ideal treatment of our patient with a retruded maxilla and deep bite, should be performed at an early age, before the age of 10, using combined dentofacial orthopedics (palatal expansion/facemask) and fixed appliances, which will give very predictable results. Because our patient came for consultation at the age of 13, it was not possible to treat him as suggested in this article; however, the results obtained with fixed appliances alone were satisfactory and the correction of the anterior crossbite was achieved11.
-
11Treatment Classification of Class III MalocclusionJ Clin Pediatr Dent, 2008
The case reported by Pratiwi and Soegiharto, Class lll skeletal and molar, which was corrected through the use of a palatal expander and facemask, followed by orthodontic treatment without extraction with a self-ligating system, presents similar characteristics to our case; however, it was not resolved in the same way. This may be because our patient did not have the Class III molar and concave profile mentioned by the authors, so we can conclude that the use of a palatal expander and facialmask was not necessary in this particular case, due to both the facial and dental characteristics, we only opted for the use of a self-ligating system, successfully correcting the patient’s malocclusion1.
-
1Treatment of Class III Malocclusion in an Adolescent with Banded RPE/Face Mask and Self-Ligating SystemUIP Health Med, 2016
According to various studies, such as those by Alami et al, Ramirez et al and Borrie and Bearn, patients with class III malocclusion should be treated as soon as possible, with the aim of allowing normal growth, improving the function and psychosocial well-being of the children, in whom removable appliances, with proper patient cooperation, are a good tool for correction. However, our patient’s treatment was not carried out in the manner suggested, since he did not present for consultation at an appropriate age, and therefore the mechanics described above were chosen, which allowed us to achieve satisfactory dental, functional and facial objectives3,5,7.
-
3Maloclusión Clase IIISalud en Tabasco, 2010
-
5Early Treatment of Anterior Crossbite Relating to Functional Class IIIEmerging Trends in Oral Health Sciences and Dentistry, 2015
-
7Early Correction of Anterior Crossbites: A Systematic ReviewJ Orthod, 2011
There are studies that show that the protraction mask is effective in young children, but not in patients over 10 years of age, so in the study presented by Konno et al, based on the unfavourable growth characteristics of their patient, who had a mandibular prognathism, he opted for a camouflage treatment to improve the occlusal relationship, and just as in our case, the results obtained were classified as successful2,12.
-
2The Effectiveness of Protraction Face Mask Therapy: A Meta-AnalysisAm J Orthod Dentofacial Orthop, 1999
-
12Correction of a Skeletal Class III Malocclusion during a Pubertal Growth Spurt by Bone-Anchored Maxillary ProtractionJ World Fed Orthod, 2017
In another case presented by Park et al, a Class III patient with an anterior crossbite, but older than our patient and with similar characteristics, was also treated with a camouflage orthodontic treatment; the results were satisfactory facial aesthetics and adequate occlusion, as well as proclination of the anterior maxillary teeth and retroclination of the anterior mandibular teeth, which are the effects obtained by compensating for this type of malocclusion. This can lead us to the conclusion that orthodontic treatment can also lead to a favourable and functional outcome9,13,14.
-
9Camouflage Treatment of Skeletal Class III Malocclusion in an Adult Cleft-Palate Patient Using Passive Self-Ligating SystemAm J Orthod Dentofac Orthop, 2019
-
13Adult Skeletal Class III Correction with Camouflage Orthodontic TreatmentAm J Orthod Dentofac Orthop, 2019
-
14Camouflage Treatment for Skeletal Class III Patient with Facial Asymmetry Using Customized Bracket Based on CAD/CAM Virtual Orthodontic SystemAngle Orthod, 2020
The comparison carried out by Miamoto et al, of two protocols for the correction of the anterior crossbite, did not find statistically significant differences when a spring-loaded anterior bite plane was used and when glass ionomer cement was placed on the occlusal surface of the first molars of the mandible, since both protocols achieved the correction of the anterior overjet; the same was observed in our patient, in whom build-ups were placed on mandibular molars that in conjunction with self-ligating brackets, achieved the correction of the anterior crossbite15,16.
-
15Comparison of Two Early Treatment Protocols for Anterior Dental Crossbite in the Mixed Dentition: A Randomized TrialAngle Orthod, 2018
-
16Early Anterior Crossbite Correction through Posterior Bite Opening: A 3D Superimposition Prospective Cohort StudyEurJ Orthod, 2018
Conclusion
Although the ideal age to treat Class III malocclusions, according to what different authors report, is at an early age, in this case the crossbite was successfully corrected with a self-ligation system and the placement of build-ups, meeting the objectives indicated from the beginning of the treatment. However, a long-term study will be necessary to determine the effectiveness and stability of this treatment.
Referencias bibliográficas
-
1Pratiwi D, Soegiharto B. Treatment of Class III Malocclusion in an Adolescent with Banded RPE/Face Mask and Self-Ligating System. UIP Health Med. 2016; 1(1): 1-6. DOI:10.7454/UIPHM.V1I0.13 Links
-
2Kim J, Viana M, Graber T, Omerza F, BeGole E. The Effectiveness of Protraction Face Mask Therapy: A Meta-Analysis. Am J Orthod Dentofacial Orthop. 1999; 115(6): 675-85. DOI: 10.1016/s0889-5406(99)70294-5 Links
-
3Ramírez-Mendoza J, Muñoz-Martínez C, Gallegos-Ramírez A, Rueda-Ventura MA. Maloclusión Clase III. Salud en Tabasco. 2010; 16(2-3): 944-50. Links
-
4Hernández J, Padilla M. Tratamiento temprano de la mordida cruzada anterior. Revisión de la literatura/Early Treatment of Anterior Cross Bite. A Literature Review. Rev. estomatol. salud. 2011; 19(2): 40-7. Links
-
5Alami S, Aghoutan H, El Quars F, Diouny S, Bourzgui F. Early Treatment of Anterior Crossbite Relating to Functional Class III. En: Virdi M (Eds.). Emerging Trends in Oral Health Sciences and Dentistry. 2015. DOI: 10.5772/59251. Disponible en: https://www.intechopen.com/chapters/47781 Links
-
6Cobourne M. Early Treatment for Class III Malocclusion. J Orthod. 2016; 43(3): 159-60. DOI: 10.1080/14653125.2016.1215860. Links
-
7Borrie F, Bearn D. Early Correction of Anterior Crossbites: A Systematic Review. J Orthod . 2011; 38(3): 175-84. DOI: 10.1179/14653121141443 Links
-
8García GE, Gurrola B, Casasa A. Sistemas de autoligado. Caso clínico. Odontología Vital. 2017; 2(27): 59-68. Links
-
9Deswita Y, Soegiharto BM, Tarman KE. Camouflage Treatment of Skeletal Class III Malocclusion in an Adult Cleft-Palate Patient Using Passive Self-Ligating System. Am J Orthod Dentofac Orthop. 2019; 155(1): 117-26. DOI: 10.1016/j.ajodo.2017.07.028 Links
-
10Mato González A, Pérez Mendoza L, Rodríguez Fuego MC, González Gutiérrez A. Mordida cruzada anterior y tratamiento en la atención primaria Crossbite and Treatment in Primary Health Care. Rev Ciencias Médicas. 2016; 20(4): 458-64. Links
-
11Kanas RJ, Carapezza L, Kanas SJ. Treatment Classification of Class III Malocclusion. J Clin Pediatr Dent. 2008; 33(2): 175-86. DOI: 10.17796/jcpd.33.2.431877341u182416 Links
-
12Konno M, Iijima M, Nagasaka-Konno M, Mizoguchi I. Correction of a Skeletal Class III Malocclusion during a Pubertal Growth Spurt by Bone-Anchored Maxillary Protraction. J World Fed Orthod. 2017; 6(2): 62-8. DOI: 10.1016/j.ejwf.2017.03.002 Links
-
13Park J, Emamy M, Lee SH. Adult Skeletal Class III Correction with Camouflage Orthodontic Treatment. Am J Orthod Dentofac Orthop. 2019; 156(6): 858-69. DOI: 10.1016/j.ajodo.2018.07.029 Links
-
14Sha HN, Lim SY, Kwon SM, Cha JY. Camouflage Treatment for Skeletal Class III Patient with Facial Asymmetry Using Customized Bracket Based on CAD/CAM Virtual Orthodontic System. Angle Orthod. 2020; 90(4): 607-18. DOI: 10.2319/102318-768.1 Links
-
15Miamoto CB, Marques LS, Abreu LG, Paiva SM. Comparison of Two Early Treatment Protocols for Anterior Dental Crossbite in the Mixed Dentition: A Randomized Trial. Angle Orthod. 2018; 88(2): 144-50. DOI: 10.2319/052117-344.1 Links
-
16Vasilakos G, Koniaris A, Wolf M, Halazonetis D, Gkantidis N. Early Anterior Crossbite Correction through Posterior Bite Opening: A 3D Superimposition Prospective Cohort Study. EurJ Orthod . 2018; 40(4): 364-71. DOI: 10.1093/ejo/cjx074 Links