











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
A greater number of elderly people and a decrease in the youngest characterize the world demographic transition, so the public health approach should aim for the majority to be able to age with a better quality of life and to reduce comorbidities. The inversion of the population pyramid brought with it an increase in the so-called geriatric syndromes (GS) that have been defined as «the cumulative effect of deficiencies in multiple physiological domains that increases the risk of negative outcomes in old age».1,2 In 2016 in Mexico there were 10 million elderly people, which represented 8.9% of the population and it is expected that by the year 2050 that amount will quadruple.1,3
The GS is a pathological entity of multifactorial etiology that occurs in old age, which reflects the poor ability of an aging body to deal with external stressors.1,3
A direct association between oral health conditions (OHC) and some GS has been described, in addition to the fact that poor oral health is associated with a lower quality of life.4-6 The negative impacts of poor oral health on daily life include reduced masticatory ability, limited food options, weight loss, poor communication, and a decrease in both self-esteem and well-being.7
Multiple risk factors for poor oral health in the elderly have been described; however, some of the factors that stand out most frequently in the Latin American population are poor water quality, a history of caries, high sugar consumption, poor oral hygiene, and smoking.8 The aging process produces diverse negative changes in the oral cavity, such as tooth loss, xerostomia, and the need for dental prostheses, which causes greater vulnerability to traumatic and infectious agents. Thus, comprehensive care for the elderly should not focus exclusively on the treatment of pathological diseases and their manifestations but should also pay attention to oral health because it affects the psychosocial and nutritional aspects that accompany the aging process.2 The present study aimed to determine the frequency of OHC and its association with some GS (depression, malnutrition, and frailty) in elderly people attending a high specialty geriatric care unit in Mexico.
Material and methods
Participants
This cross-sectional study included 124 participants aged 60 or older attending a geriatric unit in a tertiary care hospital affiliated with a university in Mexico.
Participants were identified through the appointment calendar at the geriatric outpatient clinic. Recruitment occurred between March 2018 and September 2018. Eligible patients were invited to participate in the study and provided their written informed consent. The study protocol was reviewed and approved by the local Ethics Committee.
Dependent variables
Three conditions considered geriatric syndromes were researched: frailty, malnutrition, and depression. All participants underwent a comprehensive geriatric assessment carried out by standard personnel.
Frailty
Frailty status was defined according to the five components proposed by Fried et al.9 Weight loss was defined as a self-report of unintentional weight loss (≥ 10 lbs. or more) in recent years. Exhaustion was determined by two expressions from the Center of Epidemiologic Studies-Depression scale (CES-D scale by their initials in Spanish): «I felt that everything I did was an effort» and «I could not get going». Slowness was defined by the lowest quintile in the 4-meter timed walk test, at the usual pace, adjusted for gender and height. Weakness was identified by the lowest quintile in the test of adequate grip-strength according to sex and body mass index. Low physical activity was established according to the Physical Activity Scale for the Elderly as recommended. As proposed, participants meeting three or more criteria were classified as frail, one or two were considered as pre-frail and non-frail if none were met.
Malnutrition
The nutritional risk was evaluated through the Mini Nutritional Assessment™ (MNA)10. ≤ 23.5 indicated nutritional risk and ≤ 17 was considered for malnutrition.
Depression
Depressive symptoms were assessed using the validated version of the 15 items of the geriatric depression scale (GDS). > 5 indicated the presence of depression.11,12
Oral health conditions
Three elements of oral health conditions (OHC) in elderly adults were researched as independent variables: oral hygiene, need for prosthesis/prosthesis hygiene, and xerostomia. Dentists carried out an oral clinical evaluation and the standardization of the examiners showed a kappa index of 0.88.
Oral hygiene
To measure oral hygiene, the simplified oral hygiene index (OHI-S) was used. OHI-S is made up of two elements: debris index (DI-S) and calculus index (CI-S). To obtain the index, the denture was divided into 6 sections and one tooth was selected from each section to be evaluated. The OHI-S result is the sum of the CI-S and DI-S scores, both indexes are rated from 0 to 3 and the qualification is obtained by adding the scores for each surface reviewed and dividing by the number of surfaces examined. A higher score of 1.2 indicated poor hygiene (Figure 1).13
Need for prosthesis and prosthesis hygiene
To evaluate prosthesis hygiene Vigild criteria were used.14 A clinical evaluation was performed and the number of debris in the prosthesis was reviewed. To define the need for prostheses the criteria developed by Budz were used.15 At least 3 molars in occlusion were required and according to the clinical evaluation, the patient was classified into one of the following categories: no prosthesis required, prosthesis needed, prosthesis requiring repair, partial prosthesis required, complete prosthesis required, with the prosthesis in good condition.
Xerostomia
An adaptation was made to the visual analogue scale of xerostomia questionnaire proposed by Pai et al., adding a graph to help patients with low educational level to respond more objectively (Figure 2).16
Statistical analysis
Baseline descriptive data for the final sample are shown as means and standard deviations for continuous variables and frequencies for categorical variables. The χ2 test or Fisher's exact test was used as appropriate. A logistical regression analysis was used to determine the relationship between frailty, malnutrition, and depression and a selected set of oral conditions variables. To develop an explanatory model, an unadjusted linear regression analysis was created to identify the variables of geriatric syndromes with different OHC. The selection of the independent variables used in the univariate analyzes was based on a review of the literature and clinical judgment. Regression diagnostics were performed to research any violation of the assumptions of normality, linearity, multicollinearity, and homoscedasticity. All analyses were evaluated using 95% confidence intervals and a p < 0.05 was considered statistically significant. Statistical analysis was conducted using the statistical package Stata for Windows® (Stata Corp., Texas, IL., v. 14).
Results
The mean age was 78.76 ± 7.08 and 74.2% were females. 30.6% were illiterate and up to 67.7% took care of the home. Tables 1 and 2 show the sociodemographic and health characteristics of the participants classified according to the need for prostheses and prosthesis hygiene, respectively. Tables 3 and 4 show the characteristics according to oral hygiene index and xerostomia, respectively.
Table 1 Sociodemographic, dental, and geriatric characteristics according to the need for prostheses.
| Prosthesis, n (%) | ||||||
| No required | Repair required | Partial | Complete | Good condition | Not valuable | |
| Gender | ||||||
| Male | 3 (9.4) | 2 (6.3) | 17 (53.1) | 3 (9.4) | 7 (21.9) | 23 |
| Female | 3 (3.3) | 9 (9.8) | 34 (37.0) | 15 (16.3) | 31 (33.7) | 52 |
| Marital status | ||||||
| Married | 3 (7.9) | 2 (5.3) | 15 (39.5) | 7 (18.4) | 11 (28.9) | 23 |
| Widow (er) | 1 (1.6) | 9 (14.1) | 29 (45.3) | 7 (10.9) | 18 (28.1) | 39 |
| Schooling | ||||||
| Illiterate | 0 | 5 (13.2) | 13 (34.2) | 8 (21.1) | 12 (31.6) | 20 |
| Elementary | 4 (5.3) | 6 (8.0) | 34 (45.3) | 9 (12.0) | 22 (29.3)* | 48 |
| Dentate | ||||||
| Yes | 6 (65) | 5 (5.4) | 51 (55.4) | 10 (10.9) | 20 (21.7) | 65 |
| No | 0 | 6 (18.8) | 0 | 8 (25.0) | 18 (56.3)* | 10 |
| Frailty | ||||||
| Non-frailty | 2(33.3) | 1(16.7) | 1(16.7) | 2 (33.3) | 3 | |
| Pre-frailty | 4 (7.5) | 7 (13.2) | 22 (41.5) | 4 (7.5) | 16 (30.2) | 30 |
| Frailty | 2 (3.1) | 2 (3.1) | 28 (43.1) | 13 (20.0) | 20 (30.8) | 42 |
| Nutrition (MNA) | ||||||
| Adequate | 2 (7.1) | 3 (10.7) | 10 (35.7) | 5 (17.9) | 8 (28.6) | 16 |
| At risk | 3 (4.7) | 7 (10.9) | 27 (42.2) | 9 (14.1) | 18 (28.1) | 39 |
| Malnutrition | 1 (3.1) | 1 (3.1) | 14 (43.8) | 4 (12.5) | 12 (37.5) | 20 |
| Depression | ||||||
| No | 3 (5.6) | 3 (5.6) | 23 (42.6) | 4 (7.4) | 21 (38.9) | 30 (55.6) |
| Yes | 3 (4.3) | 8 (11.4) | 28 (40.0) | 14 (20.0) | 17 (4.3) | 45 (63.3) |
* p ≤ 0.05.
Table 2 Sociodemographic, dental, and geriatric characteristics according to prosthesis hygiene.
| Prosthesis hygiene, n (%) | |||
| Good | Regular | Bad | |
| Gender | |||
| Male | 0 | - | - |
| Female | 4 (4.3) | 4 (12.3) | 5 (15.6) |
| Marital status | |||
| Married | 2 (5.3) | 7 (18.4) | 6 (15.8) |
| Widow (er) | 2 (3.1) | 9 (14.1) | 14 (21.9) |
| Schooling | |||
| Illiterate | 2 (5.3) | 6 (15.8) | 10 (26.3) |
| Elementary | 0 | 14 (18.7) | 13 (17.3)* |
| Dentate | |||
| Yes | 2 (2.2) | 11 (12.0) | 14 (15.2) |
| No | 2 (6.3) | 10 (31.3) | 10 (31.3)* |
| Frailty | |||
| Non-frailty | 0 | 0 | 3 (50) |
| Pre-frailty | 1 (1.9) | 11 (20.8) | 11 (20.8) |
| Frailty | 3 (4.6) | 10 (15.4) | 10 (15.4) |
| Nutrition (MNA) | |||
| Adequate | 1 (3.6) | 5 (17.9) | 6 (21.4) |
| At risk | 2 (3.1) | 10 (15.6) | 13 (20.3) |
| Malnutrition | 1 (3.1) | 6 (18.8) | 5 (15.6) |
| Depression | |||
| No | 3 (5.6) | 11 (20.4) | 10 (18.5) |
| Yes | 1 (1.4) | 10 (14.3) | 14 (20) |
* p ≤ 0.05.
Table 3 Sociodemographic, dental, and geriatric characteristics according to hygiene index.
| Hygiene, n (%) | ||
| Good | Poor | |
| Gender | ||
| Male | 6 (24.0) | 19 (76.0) |
| Female | 27 (40.9) | 39 (59.1) |
| Marital status | ||
| Married | 10 (37.0) | 17 (63.0) |
| Widow (er) | 18 (36.0) | 32 (64.0) |
| Schooling | ||
| Illiterate | 8 (30.8) | 18 (69.2) |
| Elementary | 22 (37.9) | 36 (62.1) |
| Frailty | ||
| Non-frailty | 1 (16.7) | 5 (83.3) |
| Pre-frailty | 15 (38.5) | 24 (61.5) |
| Frailty | 17 (37.0) | 29 (63.0) |
| Nutrition (MNA) | ||
| Adequate | 6 (28.6) | 15 (7.4) |
| At risk | 19 (38.8) | 30 (61.2) |
| Malnutrition | 8 (38.1) | 13 (61.9) |
| Depression | ||
| No | 15 (37.5) | 25 (62.5) |
| Yes | 18 (35.3) | 33 (64.7) |
Table 4 Sociodemographic, dental, and geriatric characteristics according to xerostomia.
| Xerostomia, n (%) | ||
| No | Yes | |
| Gender | ||
| Male | 11 (34.4) | 21 (65.6) |
| Female | 27 (29.3) | 65 (70.7) |
| Marital status | ||
| Married | 12 (31.6) | 26 (68.4) |
| Widow (er) | 21 (32.8) | 43 (67.2) |
| Schooling | ||
| Illiterate | 19 (50.0) | 19 (50.0) |
| Elementary | 16 (21.3) | 59 (78.7)* |
| Dentate | ||
| Yes | 26 (28.3) | 66 (71.7) |
| No | 12 (37.5) | 20 (62.5) |
| Frailty | ||
| Non-frailty | 2 (33.3) | 4 (66.7) |
| Pre-frailty | 17 (32.1) | 36 (67.9) |
| Frailty | 19 (29.2) | 46 (70.8) |
| Nutrition (MNA) | ||
| Adequate | 11 (39.3) | 17 (60.7) |
| At risk | 17 (26.6) | 47 (73.4) |
| Malnutrition | 10 (31.3) | 22 (68.8) |
| Depression | ||
| No | 14 (25.9) | 40 (74.1) |
| Yes | 24 (34.3) | 46 (65.7) |
* p ≤ 0.12.
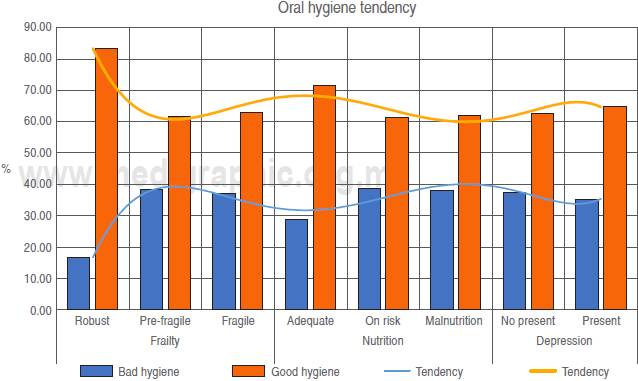
Regarding oral conditions, the frequency of edentulous was 25.8%, with a mean of missing teeth of 17 ± 9.0. Hygiene in jagged classified by OHI-S ≥ 1.2 was 63.7%, with a mean index of 3.57 ± 2.78) and only 16.3% had good oral hygiene.
Related to using dental prostheses up to 30.6% were classified in good condition; 41.1% required partial prosthesis and only 8.9% required prosthesis repair. In terms of prosthesis hygiene, only 3.2% were classified as having good hygiene; 16.9 with regular hygiene and the most frequent index (19.4%) was poor prosthesis hygiene.
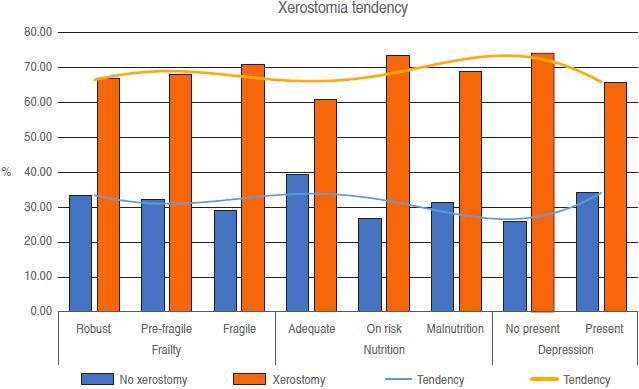
In connection with xerostomia, the level of discomfort due to dryness classified as severe was only 0.8% and up to 83.1% denied having any discomfort. Similarly, dryness when eating was denied up to 75.8%; a frequency of 12% was found in the medium dryness and only 3.2% in a severe degree. On the other hand, when speaking, the perception of dryness increased remarkably, reaching 17.7% in the moderate degree group and 8.9% in a severe degree group.
Concerning the prosthesis need index, 60.5% required some type of prosthesis, either total or partial. About the prosthesis users, only 4.3% had good prosthesis hygiene.
In relation to geriatric syndromes, 52.4% of the participants were classified as frail, and 56.5% were diagnosed with depression. According to the MNA, 51% were classified at risk of malnutrition, 25.8 malnourished, and only 22% had an adequate nutritional status.
Fifty percent of dentate patients were classified as non-frailty, and 53.5% of the patients with xerostomia had frailty. About the participants who needed prostheses, 56.8% presented depression and xerostomia and 53.5% were also diagnosed with depression. The rate of poor prosthesis hygiene was similar in the depression group (56.9 vs 54.5%, respectively). 78% of the elderly who required some type of prosthesis presented malnutrition, and 80.2% with xerostomia were also classified within this category.
The difference between the OHC and GS variables did not reach statistical significance at this level of analysis. The logistical regression analysis did not show statistical significance either.
Discussion
In this research there was not found any significant risk association between oral health conditions and some geriatric syndromes. These results contrast with the evidence obtained by other researchers. Several studies have shown a significant association between OHC and GS.3,17 Unexpectedly, in the present study, participants with xerostomia had a lower prevalence of depression than those who did not, probably due to methodological differences in the diagnostic test and the sample size of our study. Interestingly, the prevalence of edentulous subjects in the present study was twice that reported by another's.18 A probable explanation is that our sample was taken from patients attending a highly specialized geriatric care unit, and therefore with greater health problems, while the samples in other studies were taken from the general population.
Wostmann et al. found that the use of dental prostheses in the elderly had a short-term positive impact on nutritional status. In the present study, participants with a need for prostheses presented higher rates of malnutrition compared to those who did not have such a need, which suggests this same risk association. It is likely that this group of patients benefit from being referred to dental services for the use of prostheses.4
Evidence also shows that in patients with masticating and swallowing problems there are variations in micronutrient levels that are not reflected in the MNA.19 In our study, MNA was used for the diagnosis of malnutrition. Although this instrument does not measure micronutrient variations, the usefulness of the intentional search for deficiencies and its interventions is not very important to generate clinically significant changes.19-21
There is significant evidence on the benefits of different oral health interventions (prosthetics, masticatory rehabilitation, orthodontics, xerostomia treatment, etc.) in improving the quality of life and some GS, especially malnutrition.5,6,22 As we did not find a significant association between OHC and GS in our sample, the question arises as to whether oral health problems are the consequence of some geriatric syndromes and whether oral health behaves more as a protective factor than as a predisposing factor.7,23,24 In this sense, it is important to carry out longitudinal studies to establish a precise association. Researching carried out in other populations concluded that oral pathology measured with self-perception indices was related to the development of GS. These results do not agree with our findings, since in this study the assessment of oral pathology was performed by a professional in the area, which increased the sensitivity to make the diagnosis, finding, despite this, fewer self-reports of xerostomia. Regardless of the oral conditions described, the high frequency of frailty and malnutrition syndromes stands out, which reflects the health deficiencies of our population that can be explained by several factors.
Our study presents several limitations. First, it is a cross sectional design, and it is not possible to know the direction of the tendencies found. Second, the participants were recruited to attend their medical consultation in a geriatric clinic and thispaperwasnotbased on the general population. The sample probably consisted of individuals with heterogeneous characteristics, such as many patients at risk; therefore, the participants in this study had the presence of multiple diseases and related GS.
On the other hand, the most valuable part of this research was to perform the dental evaluation through standardized indices and the diagnosis of geriatric syndromes through a comprehensive geriatric assessment. In our best knowledge, this work is the first in Latin America to describe oral health conditions in the elderly through standardized dental indices. The results of the regression analysis showed a tendency despite of the already known multifactorial origin of geriatric syndromes. However, it was not statistically significant.
Conclusion
The presence of frailty, malnutrition, and depression was greater in patients with prostheses, xerostomia, and poor oral hygiene. The statistical analysis showed a non-significant risk association between oral health conditions and depression, malnutrition, or frailty. These results highlight the importance of the intentional search for oral pathology during the comprehensive geriatric assessment.

