











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Over the past 20 years, functional magnetic resonance imaging (fMRI) has provided valuable insights into the psychopathophysiology of various psychiatric disorders, particularly post-traumatic stress disorder (PTSD)1-3. fMRI research involves task-based studies in which patients perform activities that engage specific mental processes. The neurons involved in these processes require increased energy, which is primarily supplied by the oxygen in the blood circulating through capillaries near the relevant brain areas. By analyzing variations in the fMRI signal, which reflect changes in oxygenation levels (oxyhemoglobin), researchers can infer functional changes in the brain activity of the regions involved.4
There is a growing consensus among researchers5 that the primary brain regions implicated in PTSD pathology are the amygdala, the medial prefrontal cortex (mPFC), and the hippocampus6-9. Shin et al.7 in their meta-analysis of neuroimaging research on the structure and neurochemistry of these regions in individuals with PTSD have identified the neurocircuitry involved: a hyper-reactive amygdala, leading to an exaggerated response to fear and threat-related stimuli10,11, the prefrontal cortex (PFC), and the hippocampus. In contrast to the amygdala, the PFC shows decreased responsiveness, which has been linked to the mPFCs partial failure to effectively inhibit the amygdala12. Regarding the impact on the hippocampus in individuals with PTSD, there is well-documented evidence of reduced hippocampal volume, decreased neuronal integrity, and impaired hippocampal function, which are associated with deficits in explicit memory13.
There is some consensus on the neurophysiopathology underlying PTSD14,15 and studies have shown the impact of certain psychotherapies on specific brain regions. The meta-analysis conducted by Pierce and Black15 provides a comprehensive study of various trauma-focused psychotherapies and their impact specific brain regions, including nine fMRI studies on Eye Movement Desensitization and Reprocessing (EMDR) Therapy16-24. However, no functional neuroimaging studies have yet examined the EMDR-protocol for recent critical incidents and ongoing traumatic stress (PRECI) in real-time. Some Pierce and Black15 suggest that Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) may lead to significant activity in the mPFC and orbitofrontal cortex compared to other psychotherapy modalities. Similarly, EMDR Therapy has been shown to stimulate the superior frontal gyri and the dorsolateral PFC more effectively than other approaches. In addition, EMDR Therapy demonstrates the greatest potential for deactivating the insula and regions of the hindbrain. These findings align with a recent meta-comparative study on the long-term effectiveness of various psychotherapies for PTSD25, which identified EMDR Therapy and Cognitive Processing Therapy26 as having the largest effect sizes for short- and long-term follow-up, respectively.
Some case studies report similar results27 with the administration of the EMDR Standard Protocol with females with PTSD during an fMRI study, showing significant changes in self-report measures and marked change in brain activation within the PFC, indicating a ventromedial shift. Invernizzi, et al.28 demonstrated significant brain functional changes on the right anterior par hippocampal gyrus and the left amygdala (LA) with the provision of EMDR Therapy in first responders that developed PTSD after responding to the 9/11 attacks.
Real-time fMRI studies and PTSD neuromodulation
Recent studies using real-time functional magnetic resonance imaging (rtfMRI) have explored the neurobiology of various disorders, particularly PTSD, and the potential for neuromodulation through specific interventions29. A pioneering series of studies30-32 investigated the use of neurofeedback as a neuromodulation technique. The research question was whether healthy volunteers could be trained to control blood oxygenation level dependent (BOLD) activity levels in the amygdala using rtfMRI neurofeedback while watching positive autobiographical memories. The findings revealed that participants who successfully learned neurofeedback through rtfMRI were able to enhance regional BOLD activity in the amygdala. Notably, the BOLD fMRI signal increased in the LA in response to the number of neurofeedback sessions in the experimental protocol, indicating that amygdala activity can be modulated through neurofeedback during emotional experiences. Later, Zotev et al.31 confirmed that rtfMRI neurofeedback in veterans with PTSD led to improvements in amygdala functioning, particularly in fMRI connectivity between the LA and the PFC. Similar results were recently observed in the amygdala and the cingulate cortex of patients with major depressive disorder who also received rtfMRI neurofeedback training with EEG32.
EMDR therapy
EMDR Therapy is a structured eight-phase, three-pronged protocol based on the Adaptive Information Processing (AIP) theoretical model. The AIP theoretical model posits that the basis of psychopathology is memory networks of traumatic events or adverse life experiences that have been inadequately processed and maladaptively stored in a state-specific form. In EMDR Therapy these pathogenic memories are reprocessed, resulting in changes in the way the memory is encoded and subsequently experienced33. EMDR Therapy and TF-CBT are the only psychotherapies recommended for children, adolescents, and adults with PTSD by the World Health Organization Guidelines for the Management of Conditions Specifically Related to Stress34. EMDR Therapy administered to patients with cancer has been proven to be effective in the reduction of PTSD symptoms and PTSD diagnostic remission35.
The EMDR-PRECI
The EMDR-PRECI is an evidence-based, eight-phase, and three-pronged individual EMDR Therapy protocol developed in the field specifically designed for the full reprocessing of pathogenic memory networks associated with recent, present, or past prolonged adverse experiences (e.g., ongoing or prolonged traumatic stress of patients with cancer-related PTSD diagnosis, victims of sexual and/or physical violence)14. The EMDR-PRECI utilizes eye movements (EM) as a first-choice method of bilateral stimulation (BLS) to reprocess pathogenic memories. Due to the impossibility of applying EM during the protocol's reprocessing phases inside the fMRI machine, the authors decided to use the Butterfly Hug (BH) method for self-administered BLS.
The EMDR BH Method
The EMDR BH method for self-administered BLS was originated by Lucina (Lucy) Artigas during her fieldwork with the survivors of Hurricane Pauline in Acapulco, Mexico in 1998. As of November 2024, over 80 peer-reviewed published studies have shown the effectiveness of EMDR Therapy protocols and treatment intervention procedures (e.g., ASSYST, EMDR-IGTP, EMDR-IGTP-OTS, EMDR-PRECI) using the BH as a self-administered BLS method for the reprocessing of pathogenic memories in various populations (e.g., disasters survivors, individuals living in ongoing geopolitical crises, child victims of severe interpersonal violence, female survivors of domestic violence, cancer patients, survivors of terrorist attacks, individuals living in situations of ongoing war trauma, refugees). The instruction for the BH method is as follows: "Raise your hands to face level with your palms facing you. Cross your hands and hook your thumbs. Put your hands on your chest, with your middle fingers below your collarbones. Make sure that your fingers are together and as vertical as possible. Now, move your hands alternately as if they were the flapping of a butterfly's wings. Close your eyes, or keep them partially opened, focusing on a spot ahead... (pause for 3 s) breathe slowly and deeply, while you observe what is going through your mind and body, without changing it, without judging it, and without pushing your thoughts away... (pause for 3 s) you can pretend what you are observing is like clouds passing by...stop when you feel in your body that it has been enough and lower your hands to your lap"36.
Cancer and trauma
There is evidence pointing to a relationship between cancer and trauma, with the prevalence of cancer being higher among the population with trauma compared to the general population. Specifically, women who suffered traumatic experiences, victims of domestic and sexual violence, and adverse childhood experiences have a higher prevalence of cancer37. The diagnosis of a chronic illness such as cancer is considered a risk factor for developing PTSD, according to the update made to the diagnostic criteria in the DSM-5 in 2013. This relationship between cancer and trauma may be implicated by chronic inflammation and immune dysregulation induced by changes in the hypothalamic-pituitary-adrenal (HPA) axis38,39.
Objective
This descriptive and comparative study aimed to develop an EMDR-PRECI-based fMRI protocol to explore neurobiological conditions associated with PTSD and to demonstrate the effects of the application of the EMDR-PRECI in general and the BH in particular, on specific brain structures associated with PTSD.
Material and method
Study design
The authors used a transversal quantitative quasi-experimental study design to develop the EMDR-PRECI-based fMRI protocol.
Research ethics
The research design and proposal were reviewed and approved by the Institutional Review Board of the Central Hospital "Ignacio Morones Prieto" in San Luis Potosí, Mexico and was registered as number 73-16 in September 2016.
Participants
This study was conducted between 2017 and 2021 in San Luis Potosí, Mexico. Potential participants were recruited through social media networks and referrals from other cancer patients. Interested individuals were invited to call for details about the research project. A total of 50 potential participants expressed interest and received information about the study. Of the 50, 20 completed the intake interview and met the inclusion criteria. To ensure eligibility, all participants were initially assessed using the Short Post-Traumatic Stress Disorder Rating Interview (SPRINT)40. If a participant scored 16 points or higher, the Global Assessment of Post-Traumatic Stress Scale (EGEP)41 was administered to confirm a PTSD diagnosis, after which the informed consent document was signed. The patients' ages ranged from 41 to 68 years old, with an average age of 51.6. Among the participants, 15 had breast cancer, two had colon cancer, two had lung cancer, and one had lymphoma.
Inclusion criteria were: (a) Female adult, (b) diagnosis of cancer, (c) having received or currently receiving cancer treatment (e.g., surgery, radiotherapy, and/or chemotherapy), (d) having a PTSD diagnosis related to their cancer diagnosis and treatment, and (e) free of acute infections. Exclusion criteria were: (a) a terminal phase of cancer, (b) ongoing self-harm/suicidal or homicidal ideation, (c) diagnosis of a psychotic or bipolar disorder, (d) diagnosis of a dissociative disorder, (e) an organic mental disorder, (f) present, active chemical dependency problem, (g) significant cognitive impairment (e.g., severe intellectual disability, dementia), (h) at present receiving specialized trauma therapy, (i) receiving psychofarmacotherapy for the management of PTSD symptoms, and (j) receiving any other psychological, psychosocial, or psychoeducational treatment.
fMRI data acquisition
fMRI studies were performed with General Electric 1.5 T HDe high-field equipment. A standard 4-channel quadrature scanning antenna for the skull was used. The protocol included T1 spin echo pulse sequences in axial projection and BOLD-EPI 2D in axial projection (Functional Imaging). The parameters of the pulse sequences were the following: T1 Fast FLAIR Axial 2D: TR 2675, TE minimum, TI 750, FOV 24, Matrix 250 × 224, NEX 2, Frequency band 31.25. BOLD-EPI Axial 2D: TR 3000, TE 28.7, FOV 40, Matrix 64X 64, NEX 1, Frequency Band Dead. The fMRI was planned in axial projection in a dorsoventral direction. Information was acquired every 30 s while the patient was at rest and with interspersed brain activity, with the study starting at rest.
Procedure
After participants completed the intake interview and were determined to have met inclusion criteria, they were randomly assigned to one of four EMDR therapists trained in the EMDR-PRECI participating in the study. The first session of the EMDR-PRECI was conducted in the therapist's private office. During this initial session, the history and treatment planning phase was completed. The therapist asked the patient to provide a brief, general description of the adverse experience from right before the cancer treatment until the present moment. The clinician assessed clinical symptoms and the patient's stabilization skills during the preparation and stabilization phase. The EMDR BH method for self-administered BLS was also taught during this session. The first target for reprocessing inside the fMRI equipment was the worst part identified by the patient by running a mental movie of the whole cancer-related experience from right before the beginning until the present moment or even looking into the future. This unique procedure covers the patient's entire traumatic stress clinical spectrum to identify the targets for reprocessing.
Once the patient and the therapist identified the worst part of the cancer-related adverse experience selected for reprocessing, the patient was scheduled for their first reprocessing session at the Radiology and Imaging Department of Ignacio Morones Prieto Central Hospital in San Luis Potosí, where the patient's brain activity was recorded using fMRI equipment. The selected worst part was reprocessed during this session using the EMDR-PRECI reprocessing phases and the BH as self-administered BLS. The BH was chosen instead of other BLS methods (e.g., EM, bilateral sounds, taping on the knees) because it could be used inside the fMRI machine, and studies have shown that it is a non-pharmacological intervention that has proven to be effective in reducing anxiety in various populations42. The EMDR-PRECI protocol was adapted for this fMRI study with specific research objectives.
Treatment
Once the patient was positioned inside the MRI machine, the study commenced with an initial 6-min block dedicated to equipment calibration, during which the patient remained at rest. After completing this phase, the patient received instructions to begin the first block of reprocessing. At this point, the Subjective Units of Disturbance Scale (SUDS) was used to measure the level of disturbance and was recorded for the previously identified worst part of the selected cancer-related adverse experience. Each reprocessing block has duration of 6 min with 24 s. These first 24 s were used for an adjustment period of the FMR equipment after the instruction that must be indicated on each block. As many reprocessing blocks as necessary were used until the SUDS score decreased to 0. The average time inside the MRI machine was 55 min.
Only the first block of reprocessing was divided into two parts of 3 min each (uninterrupted). In the first part, we made a sequence of blocks of exposure of the worst part (of 30 s) without the BH, followed by a block of breathing (30 s of breathing and up to 3 min). After these 3 min, the second part began with a reprocessing sequence (with the BH and breathing until completing another 3 min and adding the 6 min of the first block). This first block was used as a baseline measurement. After this first baseline block, the first (after 24 s) 6 min of the reprocessing block begins. Then, the patient starts with the fragment of 30 s of reprocessing with the BH and 30 s of breathing uninterrupted until completing 6 min, and SUDs are checked. A new reprocessing block was started if the patient reported SUDs >0. More than 6-min blocks were used to reduce the SUDs to 0 or the lowest possible SUD during the 1-h study time frame. When the SUDs reached 0 or when 15 min were remaining in the fMRI study time (even if the SUD did not reach 0), the therapist went to an intermediate 6-min block in which the first 30 s the patient concentrated on the worst part of the adverse experience being reprocessed, but without doing the BH. In the subsequent 30 seconds, they were asked to focus only on breathing.
The final 6-min block for stabilization purposes was done with the patient evoking their pleasant memory or safe place. Finally, when the fMRI study concluded, the therapist scheduled a follow-up appointment to continue the EMDR-PRECI. This protocol consisted of running the mental movie again, looking for any other disturbing parts, which were subsequently reprocessed in the therapist's private office.
Deoxygenation change (DC) calculation
The DC between the treatment condition (TC) and the rest condition (RC) was calculated using the formula: DC = 100×(EC−RC)/RC. Since reduced oxygenation levels in the blood correspond to increased oxygen consumption, smaller values on the deoxygenation scale indicate higher oxygen consumption. Therefore, a positive DC relative to rest (DCExp−DCRest > 0) means that oxygen consumption in the experimental condition (BH, non-Butterfly Hug [NBH], in protocols B1, B2, and B3) was lower than at rest. Conversely, a negative DC (DCExp−DCRest < 0) indicates that oxygen consumption in the TC was higher than at the RC, reflecting an increase in oxygen consumption during the TRn.
Statistical analysis
As the time series did not meet the normality assumption (Shapiro-Wilk p < 0.05), non-parametric tests were used to evaluate differences in medians across the TCs. A Friedman Analysis of Variance (ANOVA) will be conducted to test for intragroup differences. This non-parametric test is suitable when the assumptions of parametric tests, such as normality or homogeneity of variance, are violated. The Friedman ANOVA is applied to assess differences across multiple conditions, where the same participants provide data for all conditions (i.e., repeated measures). If the Friedman ANOVA result is significant, post hoc analyses will be carried out using the non-parametric Wilcoxon test. The Wilcoxon test compares two sets of scores from the same participants, serving as the non-parametric equivalent of the dependent t-test for repeated measures data. Statistical significance will be determined using a two-tailed test. To control for Type I error, the Bonferroni correction will be applied to all Wilcoxon tests, adjusting the significance threshold to p < 0.0125. In addition, effect sizes (r) will be reported, with r > 0.5 indicating a large effect.
Results
This study measured changes in brain dynamics by analyzing blood oxygen levels between the resting state and the TC. The aim was to identify differences between pathogenic memory reprocessing moments and non-reprocessing moments. It was hypothesized that variations in blood oxygen levels would increase or decrease as an effect of the experiment, specifically during the reprocessing of pathogenic memories in the fMRI study.
Amygdala
Figure 1 illustrates the changes in blood oxygen levels within the amygdala across different phases of the study. The findings indicate that reprocessing during the fMRI study, particularly using the BH method during the reprocessing phases of the EMDR-PRECI, leads to a reduction in blood oxygen consumption in the amygdala. The literature reports that the amygdala tends to show hyperactivation in individuals with PTSD, which is linked to increased oxygen consumption due to higher energy demands10,43. Therefore, our results suggest a neuromodulator effect, implying that reprocessing through the application of the EMDR-PRECI in general, and the BH in particular, may help restore the amygdala to its baseline neurobiological state, facilitating emotional stabilization.
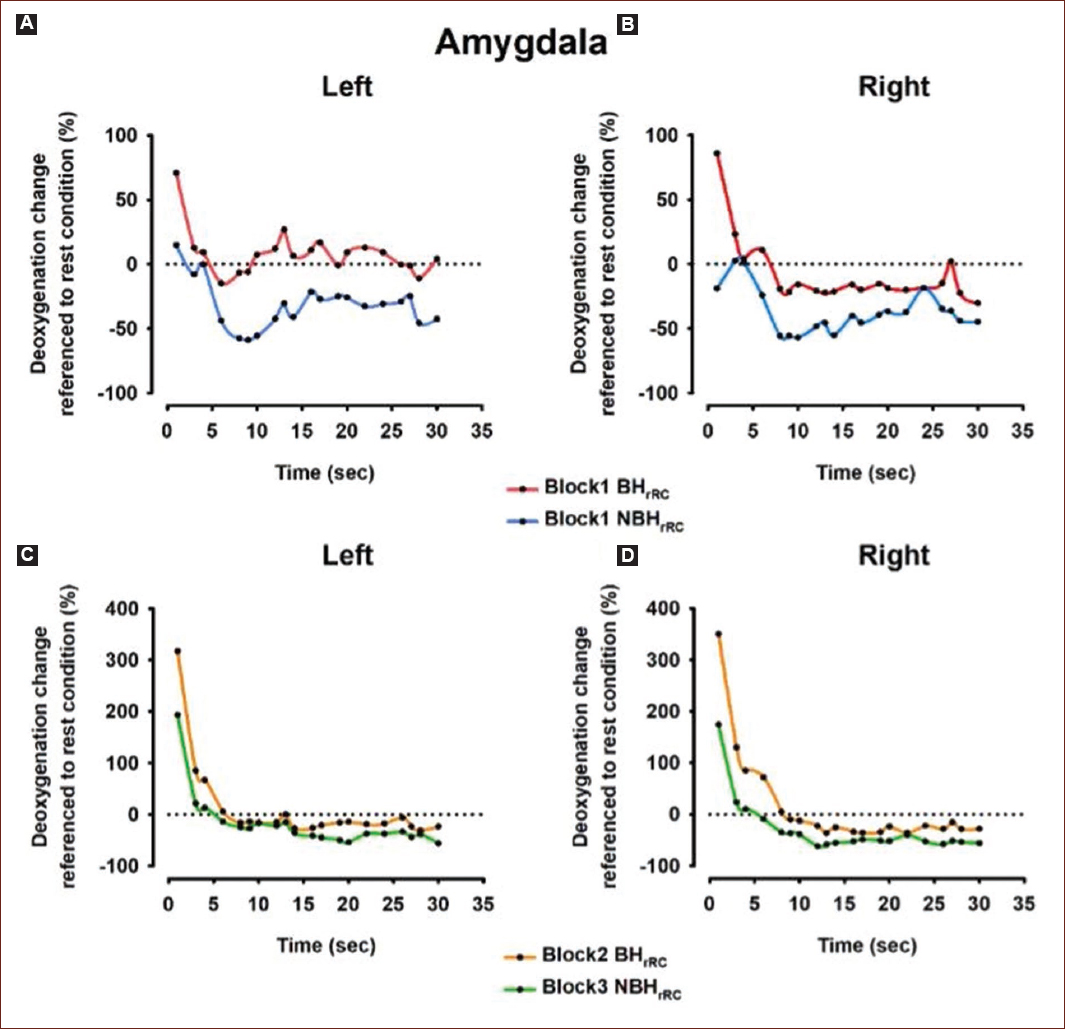
Figure 1 Time series of deoxygenation changes in the amygdala during the experimental conditions. A: the "butterfly hug" condition reduces deoxygenation levels compared to the "no butterfly hug" condition in the left amygdala. B: similarly, the "butterfly hug" condition reduces deoxygenation levels compared to the "no butterfly hug" condition in the right amygdala. C: the deoxygenation reduction profile in the left amygdala is similar between the "butterfly hug" and "no butterfly hug" conditions. D: the deoxygenation reduction profile in the right amygdala is also similar between the "butterfly hug" and "no butterfly hug" conditions. rRC = referenced to rest condition.
Figure 1 shows the time series of DCs in the amygdala during the experimental conditions BH and NBH for B1, B2, and B3. Figure 2 shows the Box Plots for DC in the amygdala across different blocks of the study. Friedman's ANOVA revealed that DCs in the amygdala were significantly influenced by the protocol (BH versus NBH), χ2 (7) = 85.3, p < 0.0001. Paired comparisons showed the following: in the LA during Block 1 (B1), deoxygenation was significantly smaller in the BH condition (median = 8.15) compared to the NBH condition (median = −30.83), Z = −3.92, p < 0.0001, r = −0.62. A similar pattern was observed in the right amygdala, where deoxygenation during B1 was also significantly smaller in the BH condition (median = −18.66) compared to the NBH condition (median = −39.97), Z = −3.92, p < 0.0001, r = −0.62. In addition, when comparing Blocks 2 (B2) and 3 (B3), the LA showed significantly smaller deoxygenation in the B2 BH condition (median = −15.95) than in the B3 NBH condition (median = −35.10), Z = −3.92, p < 0.0001, r = −0.62. A similar trend was found in the right amygdala, where deoxygenation was significantly smaller in the B2 BH condition (median = −23.26) compared to the B3 NBH condition (median = −51.59), Z = −3.92, p < 0.0001, r = −0.62 (Table 1). These results indicate that, compared to the RC, both amygdalae exhibited smaller oxygen consumption in the BH condition than in the NBH condition during the B1 and B2-B3 protocols, except only for the LA during B1-BH (Fig. 2A).
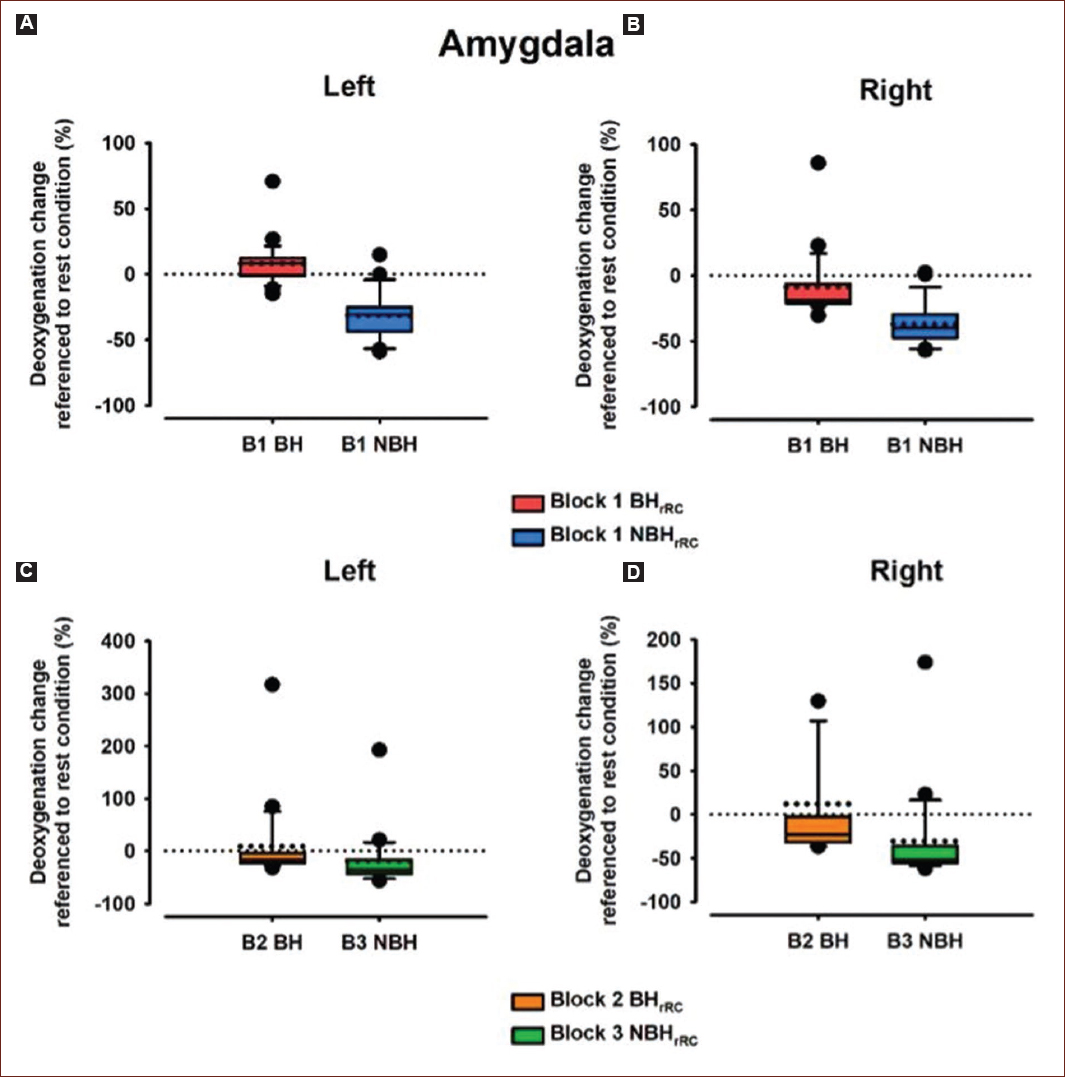
Figure 2 Box Plots for deoxygenation Change (DC) in the Amygdala. A: left amygdala DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. B: right amygdala DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. C: left amygdala DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. D: right amygdala DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. rRC: referenced to rest condition.
Table 1 Summary of the Wilcoxon test results for the Amygdala
| Condition | Median (a.u.) | Effect size | Difference | Significance |
|---|---|---|---|---|
| Amygdala left | ||||
| B1-BH | 8.15 | −0.62 | 38.98 | 0.0001 |
| B1-NBH | −30.83 | |||
| B2-BH | −15.95 | −0.62 | −19.15 | 0.0001 |
| B3-NBH | −35.10 | |||
| Amygdala right | ||||
| B1-BH | −18.66 | −0.62 | −21.31 | 0.0001 |
| B1-NBH | −39.97 | |||
| B2-BH | −23.26 | −0.62 | −28.33 | 0.0001 |
| B3-NBH | −51.59 | |||
B1: block 1; B2: block 2; B3: block 3; BH: butterfly hug; NBH: non-butterfly hug; a.u.: arbitrary units.
Hippocampus
Figure 3 shows the time series of DCs in the hippocampus during the experimental conditions BH and NBH for B1 and B2 and B3. Figure 4 shows the Box Plots for DC in the hippocampus across different blocks of the study. Friedman's ANOVA revealed that DCs in the hippocampus were significantly influenced by the protocol used (BH and NBH), Chi 2 (7) = 79.2, p < 0.0001.
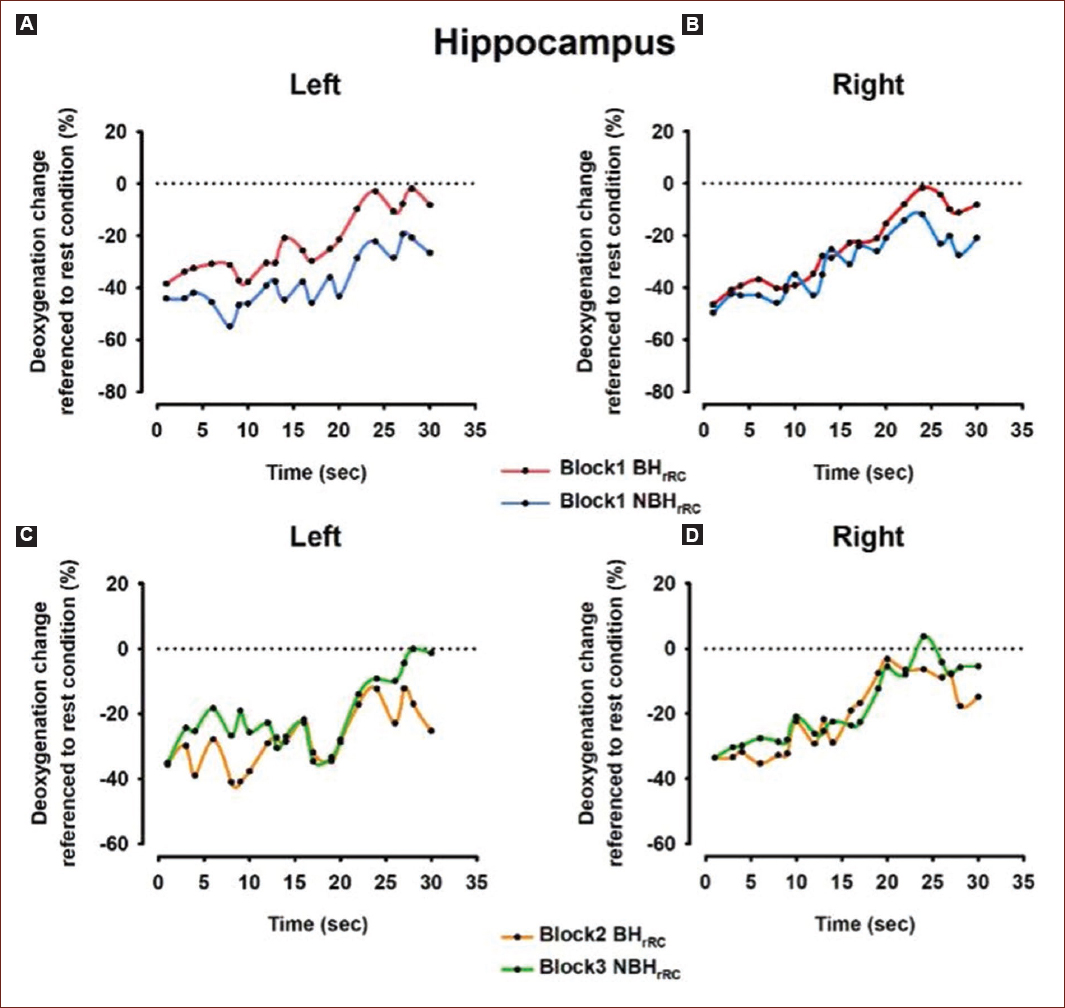
Figure 3 Time series of deoxygenation changes in the hippocampus during the experimental conditions. A: the "butterfly hug" condition reduces deoxygenation levels more rapidly compared to the "no butterfly hug" condition in the left hippocampus. B: in the right hippocampus, the "butterfly hug" condition also reduces deoxygenation levels, though at a similar pace to the "no butterfly hug" condition. C: the deoxygenation profile in the left hippocampus is similar between the "butterfly hug" and "no butterfly hug" conditions. D: the deoxygenation profile in the right hippocampus is also similar between the "butterfly hug" and "no butterfly hug" conditions. rRC: referenced to rest condition.
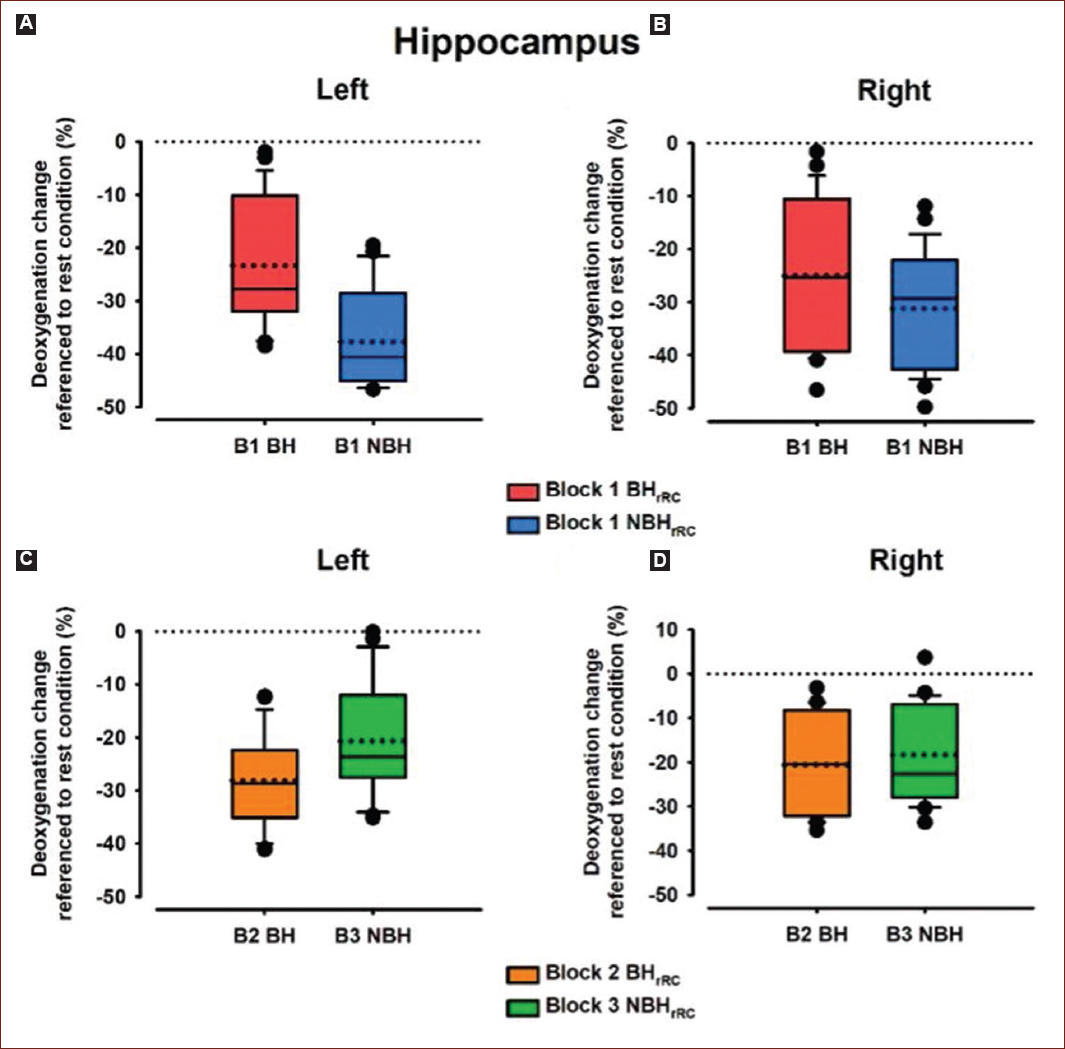
Figure 4 Box Plots for Deoxygenation Change (DC) in the Hippocampus. A: left hippocampus DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. B: right hippocampus DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. C: left hippocampus DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. D: right hippocampus DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. rRC: referenced to rest condition.
In the left hippocampus during B1, deoxygenation was significantly smaller in the BH condition (median = −27.79) compared to the NBH condition (median = −40.61), Z = −3.9, p < 0.0001, r = −0.87. A similar pattern was observed in the right hippocampus, where deoxygenation during B1 was significantly smaller in the BH condition (median = −25.38) compared to the NBH condition (median = −29.30), Z = −3.5, p < 0.001, r = −0.78.
On the other hand, when comparing B2 and B3, the left hippocampus showed significantly greater deoxygenation in the B2 BH condition (median = −28.66) compared to the B3 NBH condition (median = −23.67), Z = −3.2, p < 0.001, r = −0.71. However, in the right hippocampus, no significant difference in deoxygenation was found between the B2 BH condition (median = −20.45) and the B3 NBH condition (median = −22.66), Z = −1.6, p > 0.05, r = −0.36 (Table 2).
Table 2 Summary of the Wilcoxon test results for the Hippocampus
| Condition | Median (a.u.) | Effect size | Difference | Significance |
|---|---|---|---|---|
| Hippocampus left | ||||
| B1-BH | −27.79 | −0.87 | −12.82 | 0.001 |
| B1-NBH | −40.61 | |||
| B2-BH | −28.66 | −0.71 | 4.99 | 0.001 |
| B3-NBH | −23.67 | |||
| Hippocampus right | ||||
| B1-BH | −25.38 | −0.78 | −3.92 | 0.001 |
| B1-NBH | −29.30 | |||
| B2-BH | −20.45 | −0.36 | −2.21 | >0.05 n.s. |
| B3-NBH | −22.66 | |||
B1: block 1; B2: block 2; B3: block 3; BH: butterfly hug; NBH: non-butterfly hug; a.u.: arbitrary units; n.s.: non-significative.
These findings indicate that, compared to the RC, both hippocampi exhibited smaller oxygen consumption in the BH condition in comparison to the NBH condition, during the B1 protocol. However, in the left hippocampus, there was smaller oxygen consumption in the NBH condition than in the BH condition during the B2-B3 protocols (Fig. 4).
mPFC
Figure 5 shows the time series of DCs in the mPFC during the experimental conditions BH and NBH for B1 and B2 and B3. Figure 6 shows the Box Plots for DC in the mPFC across different blocks of the study. Friedman's ANOVA revealed that DCs in the mPFC were significantly influenced by the protocol used (BH and NBH), Chi 2 (7) = 104.6, p < 0.0001.
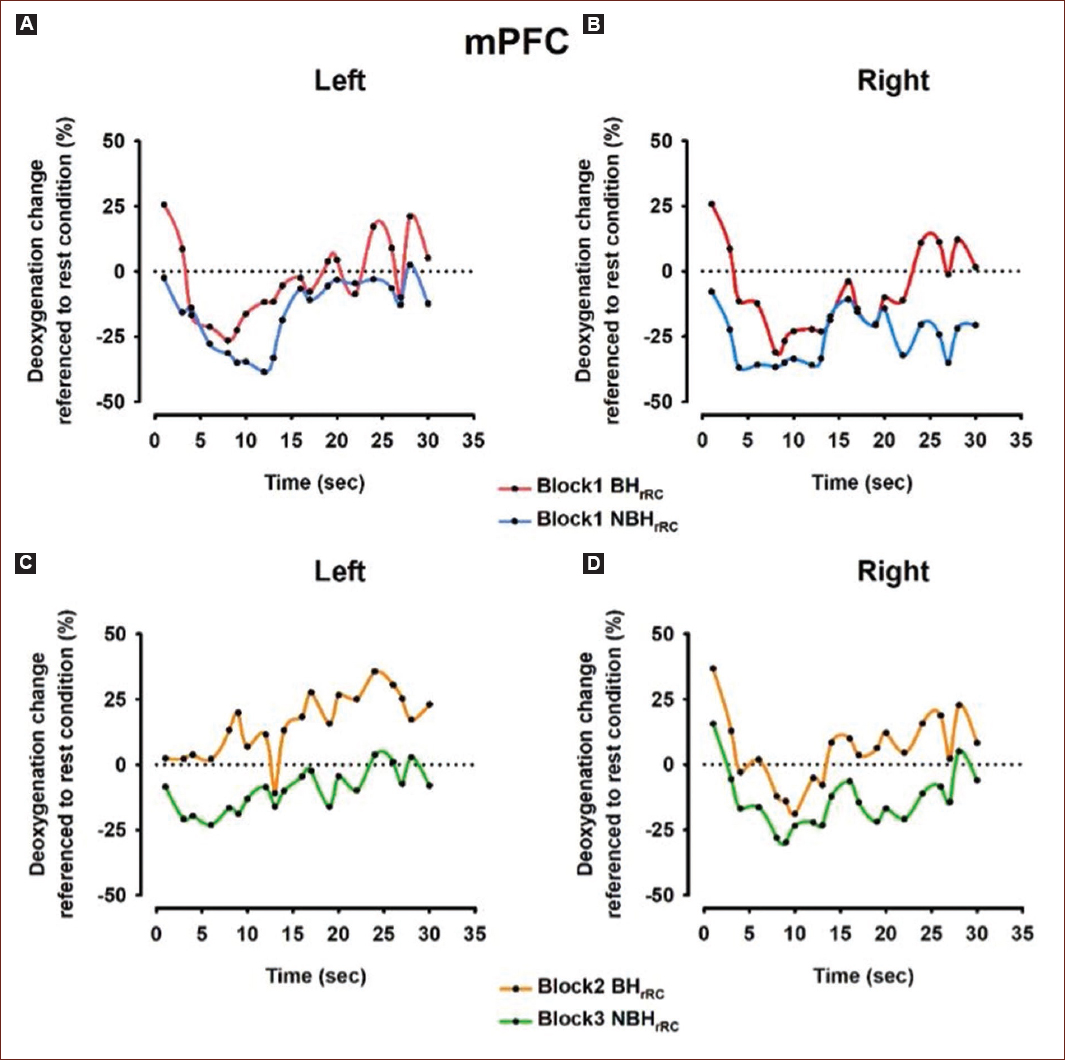
Figure 5 Time series of deoxygenation changes in the Medial prefrontal cortex (mPFC) during the experimental conditions. A: the "butterfly hug" condition shows similar deoxygenation profiles compared to the "no butterfly hug" condition in the left mPFC. B: in the right mPFC, the "butterfly hug" condition reduces deoxygenation levels compared to the "no butterfly hug" condition, particularly after 20 seconds. C: the "butterfly hug" condition reduces deoxygenation levels in the left mPFC compared to the "no butterfly hug" condition. D: similarly, the "butterfly hug" condition reduces deoxygenation levels in the right mPFC compared to the "no butterfly hug" condition. rRC: referenced to rest condition.
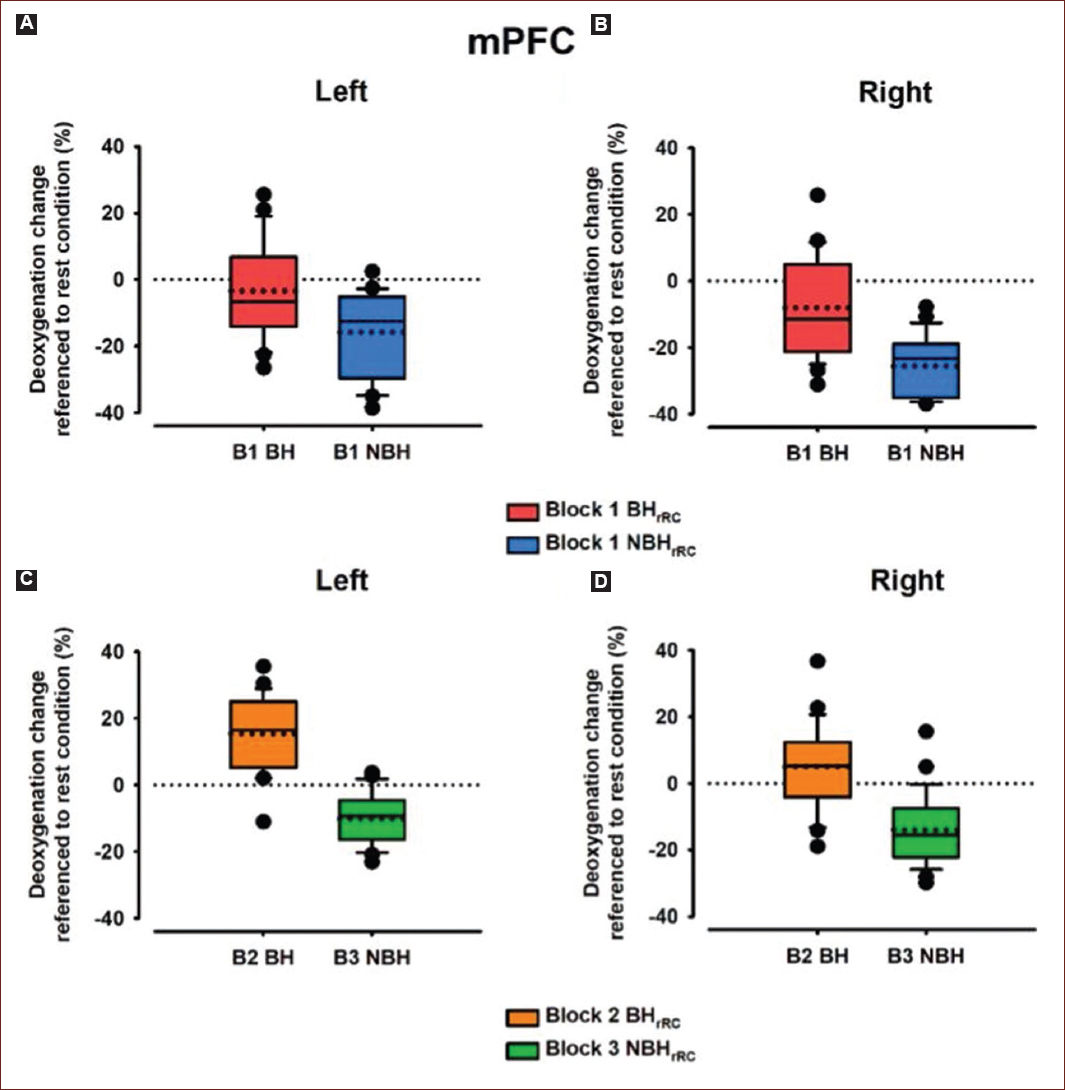
Figure 6 Box Plots for Deoxygenation Change (DC) in the Medial prefrontal cortex (mPFC). A: left mPFC DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. B: right mPFC DC for Block 1 (B1) under the butterfly hug (BH) and no butterfly hug (NBH) conditions. C: left mPFC DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. D: right mPFC DC for Block 2 (B2) under the butterfly hug (BH) condition and for Block 3 (B3) under the no butterfly hug (NBH) condition. rRC: referenced to rest condition.
In the left mPFC during Block 1 (B1), deoxygenation was significantly smaller in the BH condition (median = −6.73) compared to the NBH condition (median = −12.62), Z = −3.7, p < 0.0001, r = −0.58. A similar pattern was found in the right mPFC, where deoxygenation during B1 was significantly smaller in the BH condition (median = −11.42) compared to the NBH condition (median = −23.39), Z = −3.8, p < 0.0001, r = −0.60.
In addition, when comparing B2 and B3, the left mPFC showed significantly smaller deoxygenation in the B2 BH condition (median = 16.36) compared to the B3 NBH condition (median = −9.34), Z = −3.9, p < 0.0001, r = −0.61. A similar trend was observed in the right mPFC, where deoxygenation was significantly smaller in the B2 BH condition (median = 5.29) compared to the B3 NBH condition (median = −15.51), Z = −3.9, p < 0.0001, r = −0.61 (Table 3).
Table 3 Summary of the Wilcoxon test results for the medial prefrontal cortex
| Condition | Median (a.u.) | Effect size | Difference | Significance |
|---|---|---|---|---|
| Medial prefrontal cortex left | ||||
| B1-BH | −6.73 | −0.58 | −5.89 | 0.0001 |
| B1-NBH | −12.62 | |||
| B2-BH | 16.36 | −0.61 | −25.70 | 0.0001 |
| B3-NBH | −9.34 | |||
| Medial prefrontal cortex right | ||||
| B1-BH | −11.42 | −0.60 | −11.97 | 0.0001 |
| B1-NBH | −23.39 | |||
| B2-BH | 5.29 | −0.61 | −20.80 | 0.0001 |
| B3-NBH | −15.51 | |||
B1: block 1; B2: block 2; B3: block 3; BH: butterfly hug; NBH: non-butterfly hug; a.u.: arbitrary units.
These results indicate that, compared to the RC, both mPFC regions exhibited lower oxygen consumption in the BH condition than in the NBH condition during the B1 and B2-B3 protocols. The positive DC observed in figure 6C and D indicates that oxygen consumption was higher at rest than during the BH condition, indicating a decrease in oxygen consumption during the experimental condition (Fig. 6).
Discussion
Over the past 20 years, psychology and neuroscience have generated significant evidence on how psychological disorders affect the human brain44. This has allowed us to understand the neurobiology underlying various disorders, particularly PTSD. In addition, advances in brain imaging technology, such as fMRI, have enabled us to examine the effects of different psychotherapy modalities on brain activity associated with these conditions. The literature suggests that PTSD is characterized by specific neurobiological changes that few psychotherapy approaches - apart from EMDR therapy and EMDR therapy protocols - are capable of effectively modifying and restoring15-45.
The preset study has found some evidence of neurobiological changes associated with the reprocessing phases of the EMDR-PRECI using the BH as a self-administered BLS method. These changes may include modifications in brain activity related to memory and emotional regulation. The BH method, a form of self-administered BLS used in EMDR therapy, was used in our study to reprocess cancer-related pathogenic memories and induce behavioral changes related to the patient's overall emotional stabilization. The BH appears to trigger simultaneous changes across multiple brain regions, suggesting that this method impacts broader brain circuits. Our findings indicate that the brain areas consuming the most oxygen during this process include the right and LA, the right and left hippocampus, and the mPFC on both sides. This neurobiological system may play a key role in generating responses related to post-traumatic stress.
Furthermore, the effect sizes were consistently large, except in B2 and B3 of the right hippocampus. This suggests that the BH condition exerts a strong effect in reducing oxygen consumption. A decrease in oxygen consumption during an emotional state, such as that induced by the BH, has various clinical implications depending on the physiological and pathological context in which it occurs.
One possible interpretation is autonomic regulation and relaxation. A reduction in oxygen consumption may indicate a shift toward parasympathetic activation, promoting a state of relaxation and reducing right hippocampus activation46. Some reports indicate that emotional regulation techniques, such as meditation and diaphragmatic breathing, can lower cerebral and systemic oxygen metabolism, fostering a sense of calm.
Conversely, a decrease in cerebral metabolism has been associated with certain psychiatric conditions. For example, in major depressive disorder, reduced metabolic activity in specific brain regions, particularly those involved in emotional regulation has been linked to lower oxygen demand47. Similarly, altered metabolic patterns have been observed in states of dissociation and ineffective emotional regulation. Research suggests that trauma-induced dissociative states or extreme stress can lead to decreased activity in limbic structures such as the amygdala and mPFC, which in turn reduces oxygen consumption48.
In addition, an abnormal decrease in oxygen consumption in response to emotional stimuli has been associated with affective dysregulation, as seen in PTSD. Furthermore, some PTSD patients exhibit altered cerebral oxygen dynamics, potentially due to hyperactivation of the HPA axis, which affects cerebral blood flow regulation7. This mechanism could underlie the significant changes in oxygen consumption observed in our study, particularly given the large effect sizes associated with the BH condition.
These findings highlight the complex interplay between emotional states, autonomic regulation, and cerebral metabolism, suggesting that the observed reduction in oxygen consumption may reflect either a beneficial relaxation response or a pathological state, depending on the broader clinical context.
The data suggest that oxygen consumption in both the right and LA during the BH condition is associated with participants being exposed to distressing memories. This aligns with the assertion1 that the amygdala assigns emotional significance to various stimuli. Similarly, other authors2,3 propose that the amygdala processes exteroceptive information, regardless of sensory modality, further supporting the idea that the BH method strongly stimulates this region.
In addition, the mPFC shows higher oxygen consumption during the BH condition compared to the NBH condition. Previous studies4 suggested that this region is involved in processing emotions related to complex social and personal situations. This could explain why patients in highly stressful conditions may experience a lack of initiative or akinesia. Activating this area through the use of the BH method likely facilitates patients re-experiencing of their emotional state.
Furthermore, the increased oxygen consumption observed in the hippocampus during the BH condition appears to support the retrieval of long-term memories, particularly those consolidated over an extended period of learning or experiencing significant events5. The co-activation of cortical and subcortical regions during the BH condition suggests a coordinated effort that underpins the formation of signs and symptoms associated with PTSD.
This description of the brain circuit activated by the BH highlights that the EMDR-PRECI in general, and the BH in particular, not only aids in recovery from stressful events, modulating brain activity in the regions associated with PTSD but also has a strong scientific basis, offering valuable insights into the neurobiological mechanisms of PTSD.
The EMDR-PRECI-based fMRI protocol opens the doors to explore neurobiological conditions associated with PTSD diagnosis on specific brain structures associated with PTSD and establish a precedent that can serve as a new tool for advancing our understanding of the neurobiology of PTSD and EMDR Therapy treatment.
Conclusion
This study sheds new light on understanding the effectiveness of the EMDR-PRECI in general, as it is an EMDR therapy protocol designed explicitly for populations with recent, present, or past prolonged adverse experiences, and the BH method in particular, during the reprocessing of pathogenic memories, triggering simultaneous changes across multiple brain regions, suggesting the impact of this method in broader brain circuits. Our findings suggest that EMDR-PRECI, particularly using the BH, induces neurobiological changes associated with PTSD recovery. It also provides a fMRI protocol for future neurobiological research using the EMDR-PRECI for a better understanding of PTSD treatment. Future research should explore these effects in diverse populations and assess long-term outcomes.
The perspective that suggests the use of neuroscience tools in psychotherapy could be one of the most promising practices since it assumes that any action (psychotherapeutic procedure) inevitably has an effect on some brain system. The present work suggests that there is a possible order of activation (successive series of oxygen expenditure) during the application of the EMDR PRECI and the BH method in those patients suffering from PTSD.
Limitations and future directions
fMRI is a powerful tool in neuroscience research; however, it has several methodological and technical limitations, as well as potential confounding factors that can impact the interpretation of results. For instance, its spatial resolution is insufficient to capture neuronal activity at the level of microscopic circuits or individual synapses, while its temporal resolution is lower than that of techniques such as EEG or MEG, limiting the ability to record rapid neural dynamics49. In addition, fMRI relies on the BOLD signal, an indirect measure of neural activity that can be influenced by vascular and metabolic factors50.
Motion artifacts, even from minor head movements, can distort data, posing particular challenges in studies involving children, psychiatric populations, or neurodegenerative patients51. Many fMRI studies also suffer from small sample sizes (n < 20-30), reducing statistical power and increasing the likelihood of false positives52. Moreover, uncontrolled physiological variables - such as emotional states, fatigue, attentional fluctuations, and individual differences in cerebral vasculature - can introduce additional noise into the data, further complicating result interpretation53.
Thus, while fMRI provides valuable insights into brain function, its inherent limitations and confounding factors must be carefully addressed to ensure the validity of findings in future studies. Adopting rigorous methodological practices, including larger sample sizes, appropriate statistical corrections, and the control of physiological variables, is essential for improving the reproducibility and reliability of research in cognitive and clinical neuroscience. Other limitations of this study are the sample size (n = 20), lack of a randomized controlled trial (RCT) study design, and subsequent absence of a control group. Future studies must have access to hospitals, cancer treatment centers, or NGOs focused on providing mental health services to women with cancer to facilitate a larger sample size. Therefore, to enhance the robustness of this study, we suggest future RCT studies with a longitudinal design, a larger sample size with long-term follow-up to evaluate change stability of treatment, and populations with recent, present, or past prolonged adverse experiences and related PTSD diagnosis, with treatment as usual control group or control group Solomon four-group design with other treatment groups receiving another trauma-focused treatment, such as TF-CBT, psychological transpersonal treatments, such as holotropic breathwork54, multi-modal motion-assisted memory desensitization, and reconsolidation (3MDR)55.

