











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Intracranial or cerebral vascular malformations, including cavernomas, form a group of vascular lesions with variable hemodynamic or structural characteristics. Aneurysms, for example, are abnormal saccular dilatations of the cerebral arteries. Arteriovenous malformations are clusters of abnormal arteries and veins with an increased risk of intracranial hemorrhage. Capillary telangiectasia is characterized by dilated thin-walled capillaries due to the absence of smooth muscle or elastic fibers. Developmental venous anomalies (DVA), the most common intracranial venous malformation, are also known as venous angiomas or cerebral venous malformations. Cavernomas in contrast, consist of vascular spaces of varying sizes lined by a single layer of endothelial cells, without specific arterial or venous characteristics1.
Cavernomas, also known as cavernous angiomas or cerebral cavernous malformations (CCM), are benign, slow-flow vascular lesions2,3. Until 1960, they were considered rare lesions; with the arrival of cerebral magnetic resonance imaging (MRI)4,5, their prevalence has increased, ranging from 0.3% to 0.9%6-9, constituting between 9% and 15% of cerebral vascular malformations6,10.
Traditionally, cavernomas were thought to be congenital lesions, existing de novo only in the hereditary form. Nevertheless, an increasing number of cases have been reported where lesions develop de novo, either secondary to radiation or without any other identifiable risk factor2,8.
Cavernomas are angiographically hidden malformations lined with endothelium and filled with blood products at various stages of evolution4,10,11. They are dynamic lesions that can grow or downsize over time and rarely remain stable. The diameter of these lesions can vary significantly, ranging from millimeter-scale abnormalities to being considered giant when exceeding 6 cm in at least one dimension3.
Epidemiology
Cavernomas are considered the second most common vascular malformation of the central nervous system after DVA3. They do not exhibit a gender predilection and are typically presented between the ages of 20 and 50 years (with a mean range of 35-40 years)6. Cavernomas can exist in two forms: the hereditary form, characterized by a familial pattern (autosomal dominant with incomplete clinical penetrance), and the isolated form (sporadic)2,12.
Approximately 75% of cases present as a solitary lesion, while in familial cases, 62% are associated with multiple lesions13.
Topographically, most lesions are located in the supratentorial region (80-92%), followed by the infratentorial compartment (15%), and the spinal cord (5%). Less frequently, they appear in the retina, cranial nerves, meningeal layers, and intraventricular spaces3.
Associated genes
Cavernomas occur sporadically in 80% of cases, while their appearance in familiar forms is associated with three main genes that affect endothelial structure. One gene, KRIT1, also known as CCM1, is mapped to the long arm of chromosome 7, and two other genes, CCM2 (MGC4607) and CCM3 (PDCD10) have been found on the short arm of chromosome 3 (3q25.2-27), respectively12,14. Sporadic lesions show somatic mutations in three genes, although they lack germline inherited mutations. This indicates a molecular mechanism similar to that associated with the loss of gene function3.
Peyre et al., demonstrated in a study that sporadic cavernomas also originate from activating mutations in the PIK3K-AKT-mTOR pathway, primarily in PIK3CA, and these exceed the number of activating mutations in genes causing familial forms14.
The de novo formation of cavernomas with hereditary patterns has been documented at a frequency of 0.2 to 0.4 new lesions per patient per year15. In sporadic cases, they have only been described following radiation5 or radio neurosurgery2,7.
Etiopathogenesis
Cavernomas are vascular spaces that manage low pressure and slow blood flow within the lesion, which allows the formation of a clot, followed by its organization, and this process occurs repetitively. There is a deficiency in the tight and adherent junctions of endothelial cells, leading to leaks and impaired function of the blood-brain barrier2.
The occurrence of de novo cavernoma has been associated with exposure to radiotherapy, traumatic brain injury, previous surgery, or coexisting vascular lesions11.
Their relationship with DVA has been reported up to 33%15,16, such as capillary telangiectasia and moyamoya disease17.
In a study by Ha et al., they specifically investigated the connection between cavernomas and arteriovenous dural fistulas. Notably, in 83% of these cases, the cavernoma located adjacent to or within the venous drainage territory of the involved sinus associated with the arteriovenous dural fistula, this may be linked to the venous hypertension generated by these fistulas11,15.
The theories regarding the appearance of these lesions are 1) new lesions with rapid growth that makes them symptomatic, and 2) small lesions undetectable by imaging, remaining quiescent for an extended period with subsequent rapid growth. Cavernomas, in general, tend to decrease in size once they reach a predetermined size and stage of development, their growth potential undergoes some form of involution with concurrent stagnation or even contraction. In other words, their progression is parabolic and non-linear6.
The evolution of cavernomas can be classified into 1) quiescent, 2) variations in volume and signal in relation to hemorrhagic phenomena, and 3) luminal thrombosis and repermeabilization6.
Regarding radio-induced cavernomas, which are predominantly described in individuals under 15 years old undergoing radiation6,18, two explanations can be offered: First, while the cavernoma was present at the time of irradiation but undetectable, radiation may have favored its development or second, radiation resulted in the appearance of the cavernoma by inducing the proliferation and dilatation of vascular endothelium through hyalinization and fibrinoid necrosis of vascular walls6.
Evidence suggests that radiation-induced cavernomas develop from a cavitary lesion rather than a vascular malformation. Following tissue destruction, a new cavity forms and fills with blood, while fibrin inhibits the spread of hemorrhage, leading to the formation of a consolidated hematoma. Support for this hypothesis comes from the locations of radiationinduced cavernous hemangiomas (RICH), which turn out to be identical to the sites of stereotactic radiosurgery (SRS) treatment, where previous tumors or vascular malformations existed9.
Some authors have postulated the role of angiogenic factors in the occurrence of lesions in aggressive familial and sporadic forms6. In aggressive cases, Ki67 and bcl-2 are evident in cavernoma tissue, similar to proliferative lesions, platelet-derived growth factor, tenascin, and transforming growth factor beta are expressed in perilesional brain tissue, suggesting possible neoangiogenesis that initiates lesion growth6. Recent immunohistochemical studies have also demonstrated the expression of biological markers in cerebral cavernomas, such as nuclear antigen of cell proliferation, MIB-1, Flk-1, vascular endothelial growth factor, hypoxia-inducible factor-1α, and matrix metalloproteinase-9, indicating that cavernomas exhibit proliferative and neoangiogenic characteristics15.
The appearance or growth of cavernomas during pregnancy has been a longstanding controversy. Some researchers suggest that anemia and increased blood flow during pregnancy raise circulating blood volume and create turbulent flow within thin-walled sinusoids, which worsens the behavior of CCMs and raises the risk of rupture19. Others speculate that increased estrogen and progesterone levels lead to higher expression of growth factors and cause endothelial cell degeneration in the arterial walls. However, more recent studies have found no solid evidence supporting the presence of estrogen and progesterone receptors in CCMs20.
Tang et al.21, conducted a study highlighting the role of the gut-brain axis in the development of cerebral cavernomas. They demonstrated, through fecal sample analysis, that patients diagnosed with cavernous malformation (75 patients) have an intestinal microbiome rich in gram-negative bacteria compared to the healthy control group (29 patients). They proved that lipopolysaccharide (LPS) derived from gram-negative bacteria in the gut microbiota triggers Toll-like receptor 4 and mitogen-activated protein kinase kinase 3 signaling in cerebral endothelial cells, promoting the development of cavernomas. However, according to this study, cavernoma formation is not limited to its association with intestinal dysbiosis; they also found an association between the presence of cavernomas and the loss of function of the PDCD10 (CCM3) gene, which is involved in mucus secretion by goblet cells and its presence in the intestinal lining preventing the passage of millions of bacteria into the bloodstream21.
Histopathology
A cavernoma is composed of ectasic proliferation, a single layer of smooth muscle-lacking endothelium, a thin fibrous adventitia, and an absence of intermediate brain parenchyma within the lesion. Old hemorrhage and reactive gliosis are frequently found at the periphery of the lesion9,22.
Macroscopically, cavernous malformations appear as a well-defined, lobulated mass with a dark blue color, resembling a "raspberry" or "popcorn" appearance9.
Microscopically, Cha et al.9, described histological differences in patients with de novo cavernomas without any pre-disposing factors versus those with a history of stereotactic radiosurgery. RICH showed capillary-sized irregular vascular channels, partially compressed, with capillary proliferation in the center of the lesion, thin walls, less hyalinization, and infiltration of foamy macrophages compared to de novo cavernomas. In contrast, de novo cavernomas were composed of thick, well-formed vessels with well-defined endothelial cell-lined lumens, hyalinized walls with scattered macrophages located in old hemorrhages, and outside the vascular walls9.
Clinical manifestations
The natural history of cavernomas involves five clinically relevant scenarios: 1) lesion stabilization, 2) lesion regression, 3) increased lesion density, 4) symptomatic hemorrhage, and 5) lesion growth23.
The most frequent clinical manifestations in all patient groups include headaches, seizures, focal deficits, and hemorrhagic events6,9. Intracranial hemorrhage stands as the primary cause of disability in patients. It is believed that all cavernomas harbor hidden bleeding, as studies have documented hemosiderin halo signals in all existing classifications24. However, defining a cavernoma hemorrhage is a clinical event that involves both characteristics25:
- Acute or subacute onset symptoms (headache, seizures, altered consciousness, or new/worsened focal neurological deficit related to the anatomical location of the cavernoma)25.
- Radiological, pathological, surgical evidence, or, rarely, cerebrospinal fluid evidence of recent extra or intralesional bleeding. The presence of hemosiderin halo or an increase in cavernoma size without other evidence of recent bleeding is not enough25.
The risk of bleeding varies based on age and gender. Women under 40 years had a higher risk of bleeding (34% per lesion per year) compared to men of the same age (22%). However, the authors did not establish a direct correlation between the risk of bleeding and pregnancy5.
Clatterbuck and colleagues did not find a significant relationship between cavernoma size and the risk of hemorrhage. The annual risk of hemorrhage in their study was determined to be 3.1%26. In general, the estimated risk of developing symptomatic hemorrhage is 0.1 to 1.3% per person-year in patients who have not experienced previous hemorrhages22,27-29. On the other hand, the clinical risk of hemorrhage increases to 4.5% in patients who had experienced a previous symptomatic hemorrhage28. The risk of hemorrhage is notably higher in cavernomas located in the brainstem (10.9%) compared to those in supratentorial regions (1.7%)4,30.
The location of cavernous malformations can significantly impact their clinical presentation. In one study, 53% of patients with supratentorial lesions presented with seizures, while 64% of patients with infratentorial cavernomas presented with focal deficits. The risk for developing epilepsy in parenchymal cavernomas is 1.51% per person-year (1.35% for a single lesion and 2.48% for multiple lesions)27.
In a series of 137 patients with brainstem cavernomas, 77% presented with cranial neuropathies, and 53% had limb paresis, for cases located in the midbrain, symptoms included diplopia (69%), hemiparesis (48%), hydrocephalus, and ataxia (each in 38%). Uncommon symptoms found in this series included rubral tremor, involuntary laughter, paroxysmal coma, and vertical gaze palsy. Parkinsonism, hemichorea, and extrapyramidal symptoms have been attributed to cavernomas located in basal nuclei or thalamus31.
Diagnostic imaging
MRI stands as the most sensitive and specific diagnostic tool for evaluating cavernomas. The MRI protocol should include conventional T1 and T2-weighted images, Gradient Echo/susceptibility-weighted imaging (SWI) in the axial plane, and diffusion-weighted images3.
Typically, magnetic resonance imaging reveals enhanced multiloculated cystic lesions with a "popcorn" or "mulberry" appearance on T1 and T2 sequences due to continuous bleeding from capillaries and venules9. On the susceptibility - weighted imaging sequence, they appear as hypointense cavities that can be observed from a few millimeters in diameter5, proving highly sensitive in detecting the presence of small, cavernous malformations7 (Fig. 1).
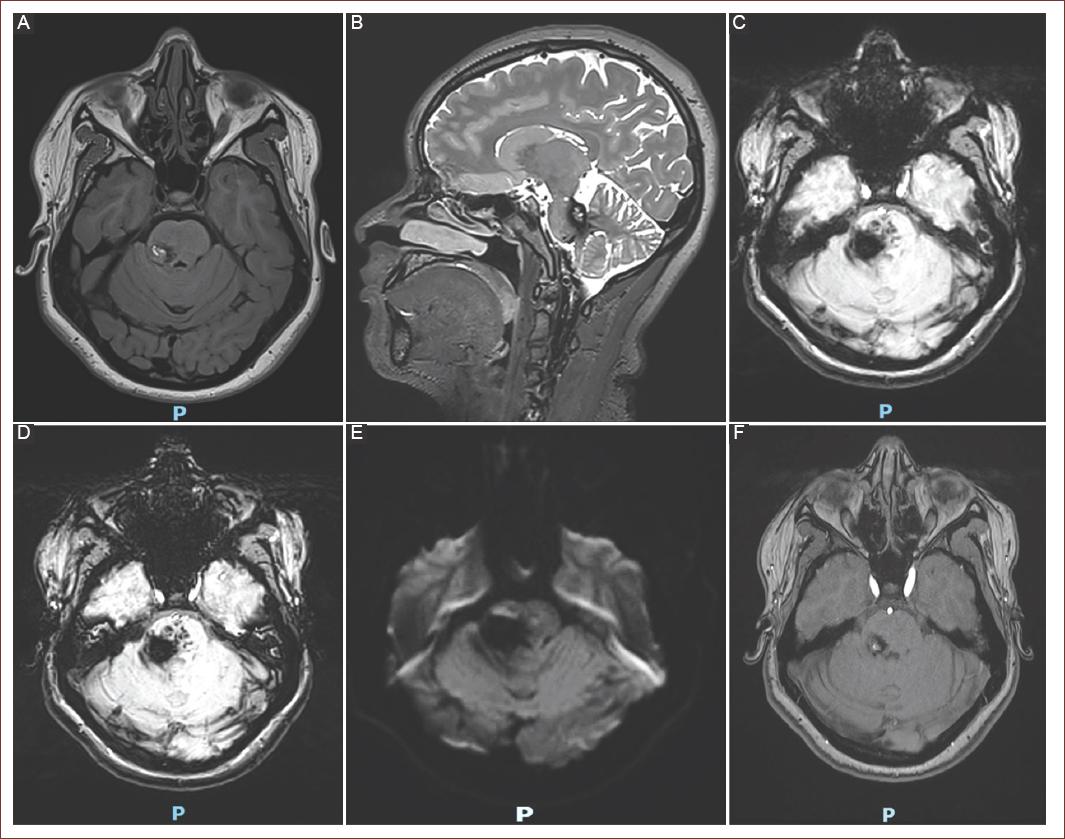
Figure 1 Magnetic resonance imaging sequences of a right posterolateral pontine cavernoma. A: axial T1-WI. B: sagittal T2-weighted imaging (T2-WI). C and D: axial gradient echo/susceptibility-weighted imaging sequences. E: diffusion-weighted imaging. F: axial contrast-enhanced T1-WI. G: axial 3D time-of-flight technique. T1-WI: T1-weighted imaging.
Based on the MRI appearance, Zabramski et al.29, classify cavernomas into 4 types: Type I, subacute bleeding dominated by methemoglobin, showing hyperintensity on T1 and T2. Type II presents mixed signal intensity on T1 and T2 with a hypointense hemosiderin ring on T2, representing evolving hemorrhage with varying ages (thrombosis of different durations). Type III exhibits hypo- or isointensity on T1 and T2 due to chronic bleeding, commonly asymptomatic lesions often seen in familial forms2. Type IV, poorly visualized, appears normal on T1WI and T2WI except on susceptibility-weighted imaging (T1* and T2* sequences), and with contrast administration, it can be differentially diagnosed from capillary telangiectasias, which enhance with contrast. Among these, Type II is the most frequent and typical (50-67%)3,12,26,29. In the case of a large hemorrhage, a Type II or III lesion may revert to the appearance of a Type I lesion26. The classification serves to predict which cavernomas are at risk of bleeding6.
Following an acute hemorrhage, the only possible imaging manifestation of a cavernous malformation may be a parenchymal hematoma. Yun et al. reported T1 hyperintensity in perilesional edema surrounding an acute or subacute hematoma in 62% of cavernomas with recent bleeding. This finding was highly specific (98%) and predictive (95%) for a cavernoma, considered a useful sign to discriminate hemorrhagic cavernomas from other bleeding lesions3 (Table 1).
Table 1 Diagnostic imaging
| Lesion | T1 Sequence | T2 Sequence | Gradient echo sequence | Cause | Histopathology |
|---|---|---|---|---|---|
| Type I | Hyperintensity17 | - | Subacute hemorrhage17 | Principal component: methemoglobin, surrounded by macrophages and gliotic brain tissue12 | |
| Type II | Classic appearance of popcorn Mixed signal intensity attributed to localized areas of hemorrhage25 | - | Thrombosis at various stages of maturation11 | Lesions with localized hemorrhage, enveloped by gliotic tissue, and hemosiderin staining within the lesion. In the brain, larger lesions may exhibit calcifications29 | |
| Type III | Isointensity or hypointensity17 | Hypointensity with a hypotensive rim amplifying the lesion size17 | Magnified hypointensity compared to T229 | Chronic hemorrhages11 | Chronic blood products and hemosiderin rim2 |
| Type IV | Limited or no visualization25 | Small, punctate, hypointense foci, often multiple17 | Likely a pre-cursor lesion of the cavernoma or corresponding to telangiectasias12,25 | Multiple punctate microhemorrhage2 | |
BLED2 risk score
The BLED2 scale is a tool created to assist physicians to evaluate the risk of recurrent hemorrhage in case of not following treatment (Table 2). Survival without events was significantly higher in patients with lower score values (p < 0.001). The score and percent risk at 1, 2, and 5 years can be calculated at: https://bled2-score.shinyapps.io/BLED2_Score/32.
Treatment
The recommendations for the treatment of patients with cavernomas vary, ranging from operating on lesions as soon as they are discovered to opting for surveillance11. Consensus generally recommends surgery when cavernomas are symptomatic4.
Treatment should be individualized by comparing it with the natural history of cavernomas in specific clinical scenarios and the region where they are located33.
Neurological considerations
In clinical practice, for patients with epilepsy related to cavernomas, it is recommended to start antiepileptic treatment to achieve seizure freedom in 50-60% of cases after diagnosis. Conservative treatment should be offered to patients with incidental diagnoses due to their low risk of seizures (< 1%/year). Standard migraine therapy is suggested for patients with recurrent migraines and cavernous malformations. Although some studies show that non-steroidal anti-inflammatory drugs are safe, more research is needed to confirm this evidence33.
Surgical treatment
For asymptomatic patients, surgical resection is not recommended, regardless of whether there is a single lesion or multiple cavernous malformations. Surgery should be considered for symptomatic cavernomas in easily accessible areas (supratentorial regions), where the risks of mortality and morbidity are comparable to living with the cavernous angioma for approximately 2 years. In contrast, surgery in more eloquent locations is associated with higher risks; and is generally recommended only for symptomatic cases or after a hemorrhage, where the risks of mortality and morbidity are comparable to living with the cavernous malformation for 5-10 years. Surgical resection has shown success rates ranging from 70% to 90% in patients with seizures refractory to medical treatment and sporadic seizures. Some authors advocate for early surgery, even if the criteria for medically refractory epilepsy are not met, to reduce the risk of hemorrhage33.
Indications for surgery in brainstem cavernomas
General indications for operating on brainstem cavernomas include any of the following scenarios: first or second clinically symptomatic hemorrhage, aggressive lesions with multiple hemorrhages, superficial or exophytic lesions, lesions located near the pial membrane, mass effect on the brainstem causing altered consciousness or requiring life support, lesions ≥ 20 mm in size and severe or progressive neurological dysfunction34.
Currently, it is recommended to delay surgery for a period of 4-6 weeks after a symptomatic hemorrhage, unless the patient exhibits altered consciousness, cardiorespiratory instability, or progressive neurological deficits. This time frame corresponds to a subacute phase. Surgical intervention within the initial 2 weeks is discouraged because the hematoma remains solid, and perilesional edema reaches its peak, heightening the risk of post-operative complications. During the recommended period, the hematoma liquefies, and edema decreases, facilitating dissection. Evacuating the hematoma typically creates an ideal space for cavernoma removal without the need to retract the brainstem. In contrast, surgery after 8 weeks involves hematoma retraction and organization, accompanied by gliosis, hyaline degeneration, and calcifications. This leads to adhesion between the cavernoma and brain parenchyma, escalating the risk of mechanical trauma during the procedure34.
Management during pregnancy
In pregnancy, when dealing with seizure disorders secondary to cavernomas, the appropriate antiepileptic medication should be carefully chosen to minimize teratogenic effects33.
Neurosurgery during pregnancy is rarely required but must be performed immediately in life-threatening and rapidly progressing clinical situations. It may be considered in cases of previous hemorrhage, family history of cavernomatosis, high-risk genes, or uncontrolled seizures. If such symptoms arise after the 30th week of gestation, surgery should be performed during the postpartum period19,20.
It is important to highlight the challenges encountered when performing neurosurgery during pregnancy. The first challenge is pre-operative evaluation. Since the use of gadolinium is contraindicated, some authors recommend its use based on the risk-benefit ratio for the patient. Alternatively, they suggest considering the possibility of a subsequent surgery during the postpartum period after an MRI with gadolinium to complete the intervention performed during pregnancy. The second issue is the use of general anesthesia, primarily due to the difficulty in securing the airway, which is the most common cause of fatal adverse events associated with general anesthesia in pregnant women19,20.
Currently, there is no consensus on the optimal delivery method for pregnant women with CCM. Some specialists prefer cesarean delivery, reasoning that it may prevent elevated blood pressure and lower the risk of hemorrhage. However, vaginal delivery is not contraindicated19,20.
A multidisciplinary team should be involved to determine the most appropriate delivery method and assess the need for neurosurgical intervention to ensure the safety of both the mother and the fetus19,20.
Similarly, it is important to reach a consensus on the risks, or lack thereof, regarding hemorrhage during pregnancy, as a study by Witiw and colleagues found that patients reproductive decisions were influenced by counseling from neurosurgeons and obstetricians. On the other hand, some patients reported not receiving any information on this matter35.
Prognosis and follow-up
Due to the unpredictable evolution of CCM, there are no guidelines to guide follow-up in asymptomatic patients. In these cases, the use of serial imaging remains controversial. The emergence of new neurological symptoms suggestive of bleeding justifies a repeat imaging as soon as possible. Follow-up imaging is suggested when cavernoma growth of 5 mm or more has been demonstrated or in patients with risk factors for mimicking these malformations (e.g., advanced age or a history of systemic cancer)3.
Alafi et al. conducted a 10-year prospective study on 75 patients newly diagnosed with cavernoma. Twenty-one percent had the familial form, while 72% did not have a confirmed genotype. Initially, 36% were asymptomatic, and 64% exhibited symptoms. The most common included cerebral hemorrhage, seizures unrelated to hemorrhage, spinal cord hemorrhage, and focal neurological deficits. Regardless of the treatment provided (pharmacological, surgical, or SRS) and the number of surgeries, the study results indicate that at the last follow-up, 83% of the patients were independent, with a modified Rankin Scale (mRS) score of ≤ 2, and patients with multiple hemorrhages (> 1) were more likely to have an mRS score of 3 or higher36. However, data on short- and long-term functional prognosis remains limited.
Clinical report
A 37-year-old woman with a medical history of well-controlled epilepsy and no family history of cavernomas, presented with an obstetric history of three pregnancies, three vaginal deliveries, and tubal ligation.
At age 28, during her third pregnancy (at 23 weeks of gestation), she suffered a left parietal intracerebral hemorrhage with ventricular rupture, requiring surgical intervention. This hemorrhage was not associated with pregnancy-induced hypertension, and diagnostic evaluation did not reveal any vascular malformations.
Eight years later, she had a recurrence manifesting as a left frontoparietal hemorrhage, which did not require surgical intervention. Subsequent brain imaging and angiography did not show any vascular malformations. Several months later, she experienced another bleeding episode, and MRI identified a circumscribed, heterogeneous, hyperintense lesion with a hemosiderin halo. She was discharged without complications for further outpatient evaluation.
One year later, during a follow-up visit, a left frontoparietal lesion was noted, showing contrast enhancement and perilesional edema, although it was neurologically asymptomatic. The imaging findings suggested a cerebral abscess (Fig. 2), prompting surgical resection. One month post-discharge, she was evaluated with a mRS score of 3, which improved to 1 after 3 months. During surgery, a 32×30×30 mm smooth, shiny, reddish-brown tissue fragment was excised. Histopathological examination revealed multiple cavities with identifiable vascular walls. Several sections confirmed the presence of a cavernous malformation, with three markedly dilated vessels, one of which contained a thrombus. The vessel walls were thin and irregular, primarily composed of collagenous tissue, as demonstrated by Massons trichrome staining. The thrombus demonstrated active recanalization, with numerous vessels lined by prominent endothelium, without atypia, and extensive hemosiderin deposits that extended into the vessel walls. The final diagnosis was cavernoma, with areas of calcification, hemosiderin deposition, and a large thrombus undergoing recanalization (Fig. 3). Currently, at 44 years of age, she has a mRS score of 0 and maintains good control of her epileptic seizures on carbamazepine 200 mg 3 times daily.
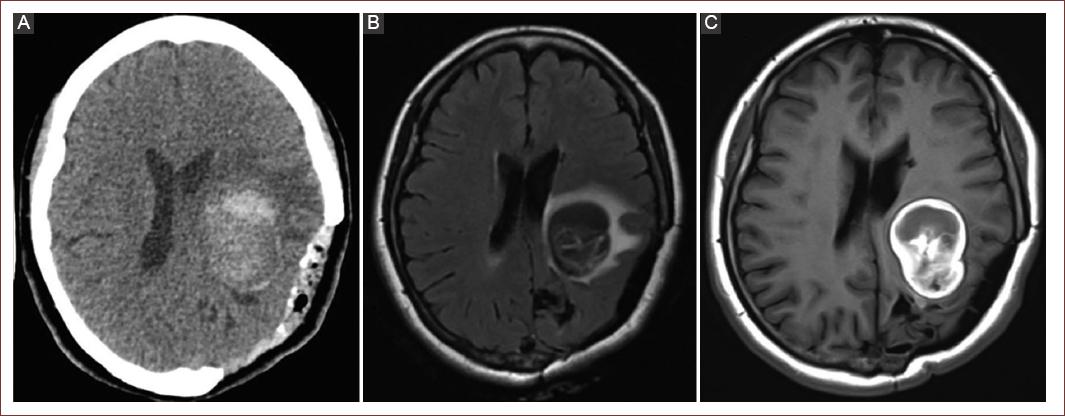
Figure 2 CT and MRI Images. A: a simple head CT scan shows a rounded heterogeneous left parietal lesion with a hyperdense border, surrounded by an area of hypodensity. B and C: axial T1 - weighted FLAIR MRI, left parietal lesion with heterogeneous content and perilesional edema. MRI: magnetic resonance imaging; CT: computed tomography.
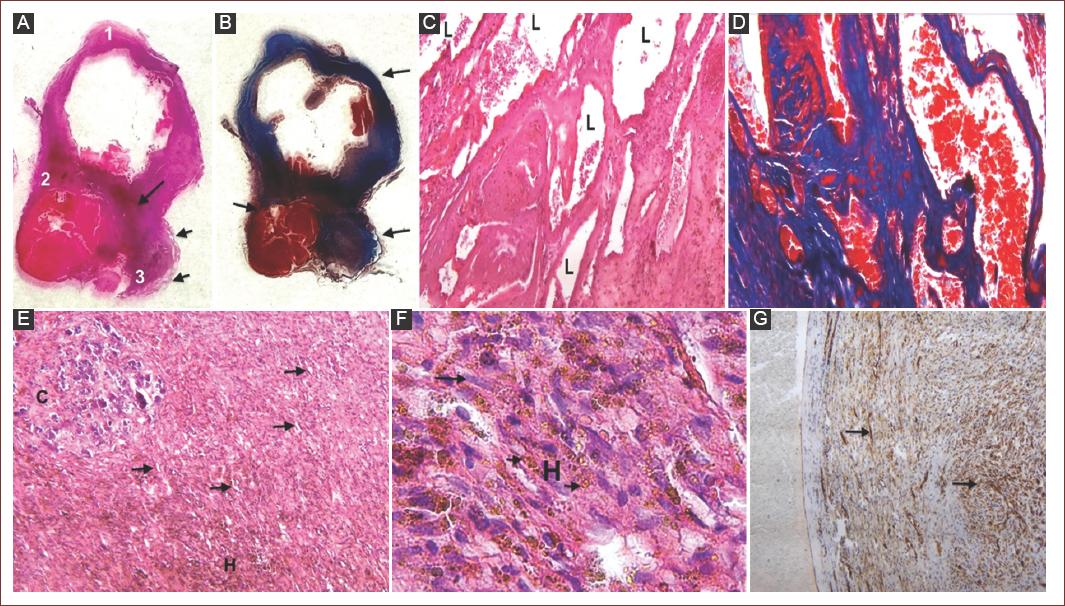
Figure 3 Histopathology. A: a complete section of the lesion is observed showing at least three very dilated venous vessels (1-3) and the periphery, numerous dilated vessels with smaller diameters (short arrows). A more hyperchromatic irregularly nodular area is also observed (long arrow), which corresponds to part of a thrombus in the process of recanalization and endothelial proliferation without atypia, as well as numerous hemosiderin deposits. B: Masson's trichrome stain shows that the vascular walls are made of collagen. C: at higher magnification, the vessels in the periphery show dilated lumen (L) and fibrous, irregular walls. The vessels are in close contact with each other. D: the walls of these vessels are made up of collagenous tissue (blue staining). Masson's trichrome. ×50. E: the thrombus in the process of recanalization shows calcifications (C), and moderate cellularity, with a proliferation of small vascular channels, lined with endothelial cells (arrows), and numerous hemosiderin deposits (H), H&E, ×50. F: at higher magnification in the area of the thrombus, the proliferation of small vessels is observed, with prominent endothelium, with elongated nuclei, slightly hyperchromatic, but without atypia (long arrow), as well as numerous hemosiderin deposits (short arrows). G: immunohistochemistry for CD34 shows vascular proliferation (arrows).
Conclusion
Cavernomas present a challenge in treatment selection due to their clinical variability. Medical attention should focus on evaluating risk factors and cavernoma characteristics, considering that the risk of seizures and bleeding is directly proportional to the number of cavernomas. In addition, the risk of bleeding increases after a previous hemorrhage. However, there is no causality between bleeding and pregnancy. MRI and risk scales, such as BLED2 score are crucial for diagnosis, patient guidance, prognosis assessment, treatment, and personalized follow-up based on symptoms, location, and short/long-term morbidity.

