











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
Introduction
The global rise in the aging population has intensified interest in the impact of age-related physiological, biomechanical, and neuromuscular changes on quality of life and independence. Aging induces multiple physiological alterations, including sarcopenia, increased fat mass, decreased bone mineral density (osteopenia/osteoporosis), reduced flexibility, impaired balance, and diminished cardiorespiratory capacity. These changes impair daily living activities and overall well-being (Cruz-Jentoft and Sayer, 2019).
Physical activity is one of the most effective interventions to counteract these declines. Resistance training, in particular, is essential for maintaining muscle strength and mass. Evidence suggests that resistance exercises performed at least twice weekly significantly enhance muscle hypertrophy, balance, flexibility, and gait speed in older adults (Fiatarone et al., 1990; Liu and Latham, 2009).
Resistance training can be conducted on land or in aquatic environments. Land-based exercises involve working against gravity using body weight or external resistance, while aquatic exercise utilizes water’s buoyancy, viscosity, hydrostatic pressure, and thermal properties to reduce joint load, offering a safer alternative especially for older adults with balance or motor control limitations (Becker, 2009; Colado et al., 2009).
Extensive research demonstrates aquatic exercise improves flexibility, balance, aerobic capacity, and functional mobility. Deng et al. (2024) found water-based training equally or more effective than land-based exercise for balance improvement. Similarly, Dalamitros et al. (2024) reported significant fitness gains in both modalities, with aquatic training favoring flexibility and land-based exercise enhancing muscular strength.
Both exercise types beneficially modify body composition; aquatic exercise tends to reduce fat mass via increased energy expenditure, whereas land-based training better promotes muscle mass (Bergamin et al., 2013). A 12-week program showed comparable strength improvements in both settings, though joint pain decreased more in the aquatic group (Colado et al., 2012).
Current evidence supports integrating aquatic and land-based resistance training to harness the unique advantages of each, tailoring regimens to individual health profiles and preferences to optimize functional capacity in older adults (Kanitz et al., 2015; Rajesh, 2023).
Nevertheless, there is a paucity of controlled studies directly comparing aquatic resistance band exercises with light-weight land-based resistance training. Moreover, studies including diverse older populations and multidimensional assessments of body composition and function remain limited. Translating exercise science into practical, evidence-based programs for this demographic group remains a significant challenge (Becker, 2009; Colado et al., 2012; Kanitz et al., 2015; Prado et al., 2022; Ruangthai et al.; 2020).
Given this context, investigating the comparative effects of aquatic and land-based resistance training protocols, characterized by the progressive use of resistance bands and structured exercise sessions, considering body composition and functional capacity in older adults is essential for developing effective, evidence-based exercise interventions to promote healthy aging (Sun et al., 2025). This study aimed to address these gaps and provide valuable scientific and practical insights. The primary objective was to evaluate and compare the effects of these resistance training programs conducted in aquatic and land-based settings on body composition and functional fitness in older adults.
Material and methods
Participants and Sampling
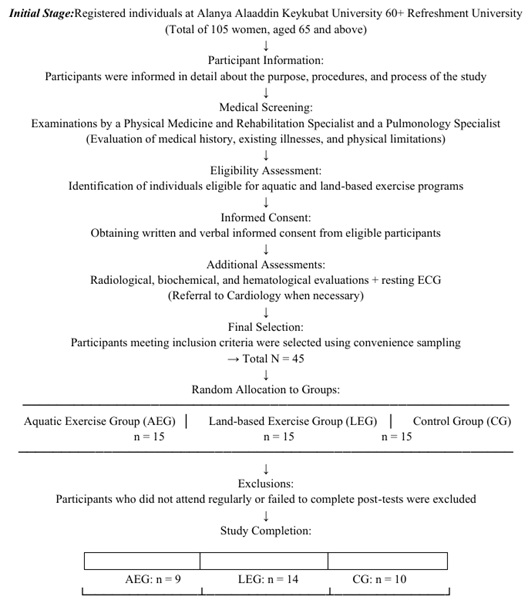
The study recruited 105 women aged 65 and older from a project at Alanya Alaaddin Keykubat University. All potential participants received detailed information about the study. Initial comprehensive medical evaluations, including history, physical assessment, and specialist consultations, determined eligibility for aquatic or land-based exercise programs. Additional tests (radiological, biochemical, hematological, ECG) and cardiology consultations were conducted as needed.
Using convenience sampling, 45 eligible participants were randomly allocated into three groups (n = 15 each): Aquatic Exercise Group (AEG), Land-based Exercise Group (LEG), and Control Group (CG). Participants who were non-compliant or did not complete post-tests were excluded, resulting in a final sample of 33 women (AEG = 9, LEG = 14, CG = 10) (Figure 1).
As presented in Table 1, the mean body mass index (BMI) of participants was 30.82 ± 3.3 kg/m² in the Aquatic Exercise Group (AEG), 29.63 ± 6.4 kg/m² in the Land-based Exercise Group (LEG), and 29.14 ± 3.7 kg/m² in the Control Group (CG). Baseline comparisons among the AEG, LEG, and CG groups demonstrated no statistically significant differences in weight (p = 0.701), height (p = 0.656), or BMI (p = 0.758). These results confirm the homogeneity of the groups with respect to key anthropometric characteristics prior to the intervention.
To ensure study safety and internal validity, strict inclusion and exclusion criteria were applied. Inclusion criteria required participants to have no severe cardiovascular, neurological, or musculoskeletal conditions; be independently ambulatory; have no falls in the past six months; obtain medical clearance for exercise; and provide informed consent. Exclusion criteria encompassed advanced osteoporosis, epilepsy, significant sensory impairments, medications affecting balance or mobility, and irregular attendance. Additionally, participants were screened using the Physical Activity Readiness Questionnaire (PAR-Q), with only those deemed low-risk included in the exercise programs.
Intervention and Implementation Process
Based on evidence supporting multicomponent exercise for older adults, this study’s intervention adhered to established protocols proven to enhance functional capacity (Aquatic Exercise Association, 2017; Martínez-Rodríguez et al., 2022). Both the Aquatic Exercise Group (AEG) and Land-based Exercise Group (LEG) engaged in 60-minute sessions, thrice weekly for eight weeks, each comprising a 10-minute warm-up, 40-minute main exercise, and 10-minute cool-down (see Table 2).
Tabla 2 Plan semanal de sesiones de entrenamiento y progresión de resistencia para los grupos de ejercicio AEG y LEG. AEG: Grupo de Ejercicio Acuático; LEG: Grupo de Ejercicio en Tierra.
Tabla 2. Weekly exercise training session plan and resistance progression for AEG and LEG exercise groups. EG: Aquatic Exercise Group; LEG: Land-based Exercise Group.
| Week | Session Phase | Exercise Examples | Sets × Reps | Resistance Band Level | Rest Between Sets | Session Duration | Frequency |
| (AEG / LEG) | |||||||
| 1–2 | Warm-up | Dynamic stretching, water/land walking | – | – | – | 10 min | 3×/week |
| Main Exercise | Hip extension, hamstring curl, scapular retraction, pulldown, chest fly | Week 1: 1×12Week 2: 2×12 | Yellow–Red | 60 sec | 40 min | ||
| Cool-down | Light walking, static stretching | – | – | – | 10 min | ||
| 3–4 | Warm-up | Same as above | – | – | – | 10 min | 3×/week |
| Main Exercise | Same as above | 2×12 | Red–Green | 90 sec | 40 min | ||
| Cool-down | Same as above | – | – | – | 10 min | ||
| 5–6 | Warm-up | Same as above | – | – | – | 10 min | 3×/week |
Aquatic Exercise Program (AE). Conducted in a temperature-controlled indoor Olympic pool (water: 28.5 - 30°C; air: 26 - 29°C; depth: 1.1 m), participants unfamiliar with aquatic exercise received two orientation sessions to ensure safety and proper technique. Exercises paralleled the land-based regimen, utilizing progressive resistance bands (yellow to black). Adherence was reinforced via reminder calls and make-up sessions, supported by motivational strategies.
Land-Based Exercise Program (LE). Held in a dry area adjacent to the pool, sessions targeted muscle strength, flexibility, balance, agility, and cardiovascular endurance. Resistance bands progressed systematically from yellow to black to match participants’ improving capacity.
Table 2 below presents the session plan and content applied in the warm-up, main exercise and cool-down phases of the AEG and LEG programs.
The structure and progression of resistance intensity, volume, and rest intervals across the 8-week intervention are summarized in Table 2, providing a detailed framework for replication and clarity regarding training load management.
Outcomes Measures
Data collection comprised three phases: pre-test, intervention, and post-test. At pre-test, participants’ height, weight, and BMI were recorded, followed by a 20-30 min battery of functional fitness tests.
The AEG completed a water-based resistance training program in an Olympic-sized pool, 60 minutes per session, three times weekly for eight weeks. LEG followed an identical protocol on land. The CG maintained usual activities without intervention but were offered the exercise program post-study if significant benefits were observed.
The overall study design is detailed in Table 3. The general structure of the experimental plan applied in the study is summarized in Table 3 below.
Tabla 3. Schedule of the trial process.
| Group | Pre-Test | Intervention Period (Weeks 2–9) | Post-Test |
| (Week 1) | (Week 10) | ||
| AEG | Body composition | Aquatic resistance exercises (8 wee- | Re-administration of the |
| (Aquatic Exercise Group) | +Functional fitness tests | ks / 3 sessions per week) | same tests |
| LEG | Body composition | Land-based resistance exercises (8 | Re-administration of the |
| (Land-based Exercise Group) | +Functional fitness tests | weeks / 3 sessions per week) | same tests |
| CG | Body composition | No intervention administered | Re-administration of the |
| (Control Group) | +Functional fitness tests | same tests |
The independent variable of the study was the type of exercise administered (aquatic or land-based). The dependent variables were defined as participants’ body composition (weight, Body Mass Index) and functional fitness levels, including muscular strength, flexibility, balance, agility, and endurance.
Material and methods subsection
Data Collection Tools
Physical function was assessed using the Senior Fitness Test (SFT) (Rikli and Jones, 2013), which includes seven standardized tests:
Back Scratch Test (BST): Assesses upper body flexibility via the distance between overlapping or non-overlapping middle fingers when reaching behind the back.
Chair Sit-and-Reach Test (CSRT): Measures lower extremity flexibility by assessing reach distance while seated.
Biceps Curl Test (BCT): Evaluates upper limb strength through the number of biceps curls performed in 30 seconds using a 2.27 kg (female) or 3.63 kg (male) dumbbell.
Chair Stand Test (CST): Measures lower limb strength by counting full stands from a seated position within 30 seconds.
6-Minute Walk Test (6MWT): Assesses aerobic endurance based on the total distance walked in six minutes on a 10-meter track.
Hand Grip Strength Test (HGST): Determines grip strength using a dynamometer; the best of two attempts was recorded in kilograms.
8-Foot Up-and-Go Test (8FUG): Assesses agility and dynamic balance through timed completion of standing, walking around a cone 2.44 m away, and sitting back down.
Body composition was evaluated via Body Mass Index (BMI), calculated using the standard formula: BMI = weight (kg) / height² (m²). To complement these, two validated balance assessments were administered:
Berg Balance Scale (BBS): Comprising 14 tasks (e.g., standing, reaching, turning), scored 0 - 4 per item (max 56), this test evaluates functional balance capacity (Berg et al., 1989).
Tinetti Balance and Gait Assessment (TBT): Includes 9 balance and 7 gait items, scored 0-2 each (max 28), providing a combined balance and gait profile (Tinetti et al., 1990).
Statistical Analysis
Data were analyzed using SPSS software version 25.0. Given the sample size was less than 50, normality of the data distribution was assessed using the Shapiro-Wilk test. Homogeneity of variances was evaluated with Levene’s test, while homogeneity of mean differences was examined through either ANOVA or Kruskal-Wallis tests, as appropriate. For within-group comparisons of pre- and post-test scores, paired samples t-tests were employed for normally distributed data, whereas the Wilcoxon signed-rank test was applied for data that did not meet normality assumptions. A significance level of p < 0.05 was adopted for all statistical analyses.
Ethical Considerations
The research protocol was reviewed and approved by the Clinical Research Ethics Committee of Selçuk University (Approval Number: 40, Date: 04,04,2024). All participants were informed in detail about the purpose, procedures, and potential risks of the study. Written informed consent, approved by the ethics committee, was obtained from each.
Results
This section presents the comparative pre- and post-intervention results for participants’ body composition and functional fitness measures, along with the statistical analysis of these differences.
Table 4 summarizes the comparisons of body weight and BMI across the groups. The AEG showed no statistically significant changes in body weight or BMI between pre- and post-intervention assessments (p > 0.05). In contrast, the LEG exhibited a significant reduction in body weight following the intervention (p = 0.047), while the change in BMI approached but did not reach statistical significance (p = 0.059). The Control Group (CG) showed no significant differences in body weight or BMI over the study period (p > 0.05).
Tabla 4. Pre- and post-test comparisons of participants’ body composition.
| Group | Variable | Tests | X ± SS | t | p | Cohen's d |
| AEG (n = 9) | Weight (kg) | Pre-Test | 72.19 ± 6.2 | 0.863 | 0.413 | -0.047 |
| Post-Test | 71.89 ± 6.7 | |||||
| BMI (kg/m²) | Pre-Test | 30.82 ± 3.3 | 0.864 | 0.413 | -0.038 | |
| Post-Test | 30.69 ± 3.5 | |||||
| LEG (n = 14) | Weight (kg) | Pre-Test | 71.48 ± 14.6 | 2.197 | 0.047* | 0.051 |
| Post-Test | 70.73 ± 14.5 | |||||
| BMI (kg/m²) | Pre-Test | 29.63 ± 6.4 | 2.070 | 0.059 | 0.045 | |
| Post-Test | 29.34 ± 6.4 | |||||
| KG (n = 10) | Weight (kg) | Pre-Test | 69.48 ± 7.3 | -1.530 | 0.160 | -0.104 |
| Post-Test | 70.25 ± 7.5 | |||||
| BMI (kg/m²) | Pre-Test | 29.15 ± 3.7 | -0.882 | 0.401 | 0.044 | |
| Post-Test | 29.31 ± 3.8 |
*p < 0.05, AEG: Aquatic Exercise Group, LEG: Land Exercise Group, KG: Control Group, BMI: Body Mass Index.
As presented in Table 5, the AEG demonstrated statistically significant improvements in multiple functional fitness measures, including 6MWT, CST, BCT, CSRT, BST, 8FUG, BBS, and TBT (all p < 0.05). These findings indicate that the aquatic exercise intervention effectively enhanced participants’ functional capacity, particularly in balance, muscular strength, and flexibility. No significant change was observed in HGST (p > 0.05). Additionally, effect size analyses revealed large effects for BCT (Cohen’s d = 1.500) and 6MWT (Cohen’s d = 0.998), further supporting the pronounced benefits of aquatic resistance training in these domains.
Tabla 5. Aquatic exercise group functional fitness test results.
| Variable | Test | X ± SS | t / Z | p | Cohen's d |
| 6MWT | Pre-Test | 482.44 ± 57.9 | t = -3.583 | 0.007** | 0.998 |
| Post-Test | 540.22 ± 73.5 | ||||
| CST | Pre-Test | 11.55 ± 2.6 | t = -2.600 | 0.032* | 0.896 |
| Post-Test | 13.88 ± 1.9 | ||||
| BCT | Pre-Test | 13.88 ± 2.3 | t = -2.809 | 0.023* | 1.500 |
| Post-Test | 17.33 ± 3.8 | ||||
| HGST | Pre-Test | 21.03 ± 5.3 | t = -0.005 | 0.996 | -3.585 |
| Post-Test | 21.03 ± 4.2 | ||||
| CSRT | Pre-Test | 8.44 ± 11.1 | z = -2.214ᵇ | 0.027* | -0.480 |
| Post-Test | 3.11 ± 9.1 | ||||
| BST | Pre-Test | 11.11 ± 11.5 | t = 3.212 | 0.012* | -0.310 |
| Post-Test | 7.55 ± 11.5 | ||||
| 8FUG | Pre-Test | 7.72 ± 1.3 | z = -2.521ᵇ | 0.012* | -1.192 |
| Post-Test | 6.17 ± 1.0 | ||||
| BBS | Pre-Test | 49.11 ± 1.9 | z = -2.555ᶜ | 0.011* | 1.226 |
| Post-Test | 51.44 ± 2.3 | ||||
| TBT | Pre-Test | 91.11 ± 3.7 | t = -7.155 | 0.000** | 0.719 |
| Post-Test | 93.77 ± 4.0 |
* p < 0.05, ** p < 0.01 and ᵇ Positive significant change / ᶜ Negative significant change.
As shown in Table 6, the LEG demonstrated statistically significant improvements in CST, BCT, BST, 8FUG, BBS, and TBT (p < 0.05). Notably, large effect sizes were observed for CST, BCT, and 8FUG (Cohen’s d > 1), indicating substantial improvements. No significant changes were detected in the remaining tests (p > 0.05).
Tabla 6. Land exercise group functional fitness test results.
| Variable | Test | X ± SS | t / Z | p | Cohen's d |
| 6MWT | Pre-Test | 484.07 ± 81.0 | t = -1.915 | 0.078 | 0.543 |
| Post-Test | 528.07 ± 76.7 | ||||
| CST | Pre-Test | 7.59 ± 0.8 | z = -3.310ᵇ | 0.001** | -1.800 |
| Post-Test | 6.15 ± 0.7 | ||||
| BCT | Pre-Test | 16.21 ± 2.7 | t = -4.072 | 0.001** | 1.693 |
| Post-Test | 20.78 ± 4.6 | ||||
| HGST | Pre-Test | 21.79 ± 4.4 | t = -1.586 | 0.137 | 0.282 |
| Post-Test | 23.03 ± 3.9 | ||||
| CSRT | Pre-Test | 7.21 ± 8.9 | z = -1.304 | 0.192 | -0.361 |
| Post-Test | 4.00 ± 8.2 | ||||
| BST | Pre-Test | 10.21 ± 9.5 | t = 2.414 | 0.031* | -0.196 |
| Post-Test | 8.35 ± 10.3 | ||||
| 8FUG | Pre-Test | 7.59 ± 0.80 | t = 7.445 | 0.000** | -1.800 |
| Post-Test | 6.15 ± 0.70 | ||||
| BBS | Pre-Test | 47.71 ± 5.8 | z = -3.111ᵇ | 0.002** | 0.381 |
| Post-Test | 49.92 ± 6.7 | ||||
| TBT | Pre-Test | 83.85 ± 5.9 | t = -2.918 | 0.012* | 0.678 |
| Post-Test | 87.85 ± 5.4 |
* p < 0.05, ** p < 0.01 and ᵇ Positive significant change / ᶜ Negative significant change.
As shown in Table 7, the CG exhibited no statistically significant differences in functional fitness tests between pre-test and post-test measurements (p > 0.05).
Tabla 7. Control group functional fitness test results.
| Variable | Test | X ± SS | t / Z | p | Cohen's d |
| 6MWT | Pre-Test | 492.50 ± 54.3 | t=-0.639 | 0.539 | -0.202 |
| Post-Test | 502.30 ± 69.1 | ||||
| CST | Pre-Test | 12.40 ± 1.4 | z=-0.447 | 0.655 | -0.141 |
| Post-Test | 12.50 ± 1.4 | ||||
| BCT | Pre-Test | 17.60 ± 2.3 | z=0.000 | 1.000 | 0.000 |
| Post-Test | 17.60 ± 2.4 | ||||
| HGST | Pre-Test | 23.80 ± 1.9 | t=1.352 | 0.209 | 0.427 |
| Post-Test | 23.04 ± 1.9 | ||||
| CSRT | Pre-Test | 4.00 ± 3.6 | t=1.221 | 0.253 | 0.386 |
| Post-Test | 3.10 ± 3.9 | ||||
| BST | Pre-Test | 7.80 ± 6.7 | t=-0.514 | 0.619 | -0.162 |
| Post-Test | 8.00 ± 6.5 | ||||
| 8FUG | Pre-Test | 6.29 ± 0.5 | z=-0.524 | 0.600 | -0.165 |
| Post-Test | 6.38 ± 0.6 | ||||
| BBS | Pre-Test | 51.90 ± 1.4 | t=0.712 | 0.494 | 0.225 |
| Post-Test | 51.50 ± 1.5 | ||||
| TBT | Pre-Test | 93.30 ± 3.4 | t=-0.129 | 0.900 | -0.041 |
| Post-Test | 93.50 ± 2.9 |
* p < 0.05, ** p < 0.01 and ᵇ Positive significant change / ᶜ Negative significant change.
Discussion
This study examined the effects of aquatic and land-based exercise programs on body composition and functional fitness in older adults. The results demonstrated that both exercise modalities produced positive outcomes, with distinct benefits across different parameters. These findings are discussed below under the subheadings “Body Composition” and “Functional Fitness”, contextualized within the existing literature.
Body Composition
Our findings revealed a significant improvement in body composition exclusively within the land exercise group (p < 0.05), indicating the potential of land-based interventions for weight management in older adults. However, the lack of significant change in BMI suggests that the program’s duration and intensity may have been insufficient to affect this metric.
In contrast, the aquatic exercise group showed no significant changes in body composition. This may be due to the buoyancy effect of water, which reduces gravitational load and mechanical stress on muscles and bones, potentially limiting metabolic stimuli required for fat loss and muscle hypertrophy. Additionally, the relatively short duration (8 weeks) and moderate intensity of the aquatic program might have constrained observable changes.
Previous studies have reported mixed results regarding the effects of aquatic exercise on body composition. Irandoust and Taheri (2015) observed significant improvements in BMI, waist-to-hip ratio, body fat percentage, and muscle mass following a 12-week aquatic exercise program. Similarly, Bergamin et al. (2013) reported positive outcomes in body composition after 24 weeks of water-based training. Buitrago-Restrepo et al. (2024) also concluded in their systematic review and meta-analysis that aquatic exercise contributes to improvements in lower limb muscle power and overall physical performance in older adults. These studies highlight that the effectiveness of aquatic exercise is influenced by factors such as program duration, intensity, and structure.
The discrepancy between the lack of significant change in our aquatic exercise group and the positive outcomes reported in previous literature, may be attributed not only to program parameters but also to the baseline functional levels and characteristics of the participants. Therefore, to enhance the effects of aquatic exercise on body composition, longer and more intensive interventions may be recommended.
Importantly, aquatic exercise offers a low-impact, supportive, and safe environment, facilitating participation among older adults with balance impairments or joint issues. This supports its use for populations at high risk of falls or musculoskeletal limitations, despite limited impact on body composition. In summary, while land-based exercise appears more effective for improving body composition, aquatic exercise’s safety and functional benefits make it a valuable option for certain high-risk groups.
Functional Fitness
Significant functional fitness improvements were noted in the aquatic exercise group, including enhanced aerobic endurance, upper and lower extremity strength, flexibility, agility, and balance (p < 0.05). Handgrip strength did not improve significantly (p > 0.05), suggesting the need for targeted resistance training to address this parameter.
These results align with Kieffer et al. (2012) who reported positive effects of short-term aquatic exercise on functional strength and agility. Oh and Lee (2021) similarly found greater improvements in hip strength, balance, and quality of life with aquatic versus land exercise. Suomi and Collier (2003) also demonstrated that aquatic exercise benefits older adults with arthritis, particularly in balance, supporting our findings. In the assessment of aerobic endurance, while the aquatic exercise group showed significant improvements in the six-minute walk test results (p < 0.05), no similar enhancement was observed in the land-based exercise group (p > 0.05). This suggests that the intensity and content of the land-based program were insufficient to elicit improvements in aerobic capacity, highlighting the need for future interventions to more directly target this parameter. Similar findings reported by Oh and Lee (2021) further support this interpretation.
The study conducted by Takeshima et al. (2022) reported that water-based exercises promoted multidimensional physical development in elderly women. This finding is consistent with the significant improvements observed in flexibility, agility, and muscular strength in our study (p < 0.05). However, the absence of significant improvement in handgrip strength in both studies suggests that exercises specifically targeting grip strength may not have been adequately implemented.
A thesis by Yüzlü (2014) comparing aquatic and land exercise effects on older adults reported no significant differences between groups but noted overall functional improvements, similar to our findings. Our data, however, suggest that aquatic exercise may confer superior benefits in balance, agility, and aerobic endurance, likely due to enhanced proprioceptive feedback and reduced fall risk.
Overall, both exercise modalities effectively enhance functional fitness in older adults. Given its low-impact and proprioceptive advantages, aquatic exercise offers a safer alternative for individuals with balance or musculoskeletal challenges. Incorporating targeted resistance training may optimize gains in specific domains such as grip strength. Future research should explore combined aquatic-land programs to maximize functional improvements.
The study exhibits several methodological strengths. Its experimental design allows for causal inference, while the implementation of multicomponent, standardized protocols across aquatic and land-based settings enhances both comparability and intervention fidelity. Comprehensive outcome measures encompassing strength, balance, flexibility, agility, and endurance afford a robust, multidimensional assessment of physical function. Adherence was supported through reminder calls and make-up sessions, further strengthening study rigor.
However, certain limitations warrant consideration. The sample consisted solely of older women with a modest size, limiting the generalizability of findings. The eight-week intervention period restricts conclusions regarding long-term effects. Participant blinding was unfeasible, and potential confounding factors such as diet, medication, and baseline activity levels were uncontrolled. Moreover, important domains including psychological, cognitive, and quality-of-life outcomes were not evaluated. This study also lacked assessment of participants’ subjective perceived effort and did not monitor weekly progression; incorporating such measures (e.g., Borg Rating of Perceived Exertion scale) in future research could yield valuable insights into motivation, adherence, and program feasibility. Finally, attrition and the absence of per-protocol analyses may have introduced bias. Future investigations should prioritize extended follow-up durations, gender-balanced cohorts, and a broader range of outcome variables to support the development of more comprehensive and sustainable intervention strategies.
Conclusions
This study demonstrated that both aquatic and land-based resistance exercise programs significantly improved body composition and functional fitness in older women. While land-based exercises yielded greater improvements in body composition, aquatic exercises were more effective in enhancing balance, agility, and aerobic endurance. Given its low-impact, joint-friendly, and proprioceptive-enhancing properties, aquatic exercise appears especially suitable for older adults with balance impairments or a high risk of falls.
Incorporating targeted resistance exercises-particularly to improve grip strength-may further enhance functional outcomes. Moreover, combining exercise interventions with nutritional strategies could optimize muscle health and overall functional capacity. Future studies should investigate the long-term effects and psychosocial outcomes of these interventions in more diverse populations, including older men, to develop comprehensive strategies supporting healthy aging and independent living.

