











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
An individual’s initial years of life are of paramount importance, as they establish the foundational elements that underpin their health and well-being in those years. During this period, the physical, sensory, communicative, cognitive, and socioemotional skills are nurtured, paving the way for autonomy and the gradual acquisition of complex skills1. Therefore, children must receive loving and sensitive care from their caregivers, health professionals, teachers, and other frontline workers2. Considering the widely acknowledged crucial nature of the initial three years of life for early childhood development (ECD), it is imperative to capitalize on this period for the timely identification of children facing developmental challenges. Deviations from the anticipated parameters or timelines during developmental processes may cause potential disorders, health conditions, or other factors that may adversely impact the subject’s development3. Thus, early detection must be conducted through existing large-scale services and programs, such as the Control of Growth and Development (CRED), which is a pivotal starting point and the most accessible one to families4. Consequently, health professionals require instruments to facilitate the detection of these potential risks and developmental delays.
In Peru, the extent to which these instruments facilitate the timely identification of these issues remains ascertained; therefore, further data on their actual scope is necessary. The employed instruments were developed over twenty years ago and may possess some technical limitations inherent to a long-standing standardization5-7. Children with sustained developmental delays are at increased risk of learning difficulties, behavioral problems, and functional disorders later in life8. It has been demonstrated that, when detected early, interventions are significantly more effective; therefore, this circumstance requires prompt attention. Furthermore, periods of greater neuroplasticity allow greater receptivity to treatment9,10. Lack of early detection and timely intervention may cause greater developmental difficulties and hinder children’s ability to reach their full potential.
Developmental assessment instruments can be classified into two types based on their purpose: screening or evaluation. Screening instruments offer a preliminary assessment of the child’s health and developmental status and indicate whether further evaluation is necessary to identify potential difficulties that require specialized interventions or services. They are usually brief and accurate; however, they usually fail to detect the degree or extent of the problem. Conversely, assessment instruments facilitate a more comprehensive understanding of the individual needs of children at risk. These needs are identified through observation, collection, recording, and interpretation of pertinent information, enabling informed decision-making11. This important difference has been recognized in the process of updating the developmental assessment instruments in the Technical Health Standard for Growth and Development Monitoring of Children under Five Years Old, which is being conducted within the framework of the ECD Results-Based Budget.
In response, a multi-sectoral panel of specialists met weekly during the first half of 2020 to compile and analyze the evidences related to the developmental screening instruments currently in use, nationally and internationally, and to propose a shortlist for inclusion in the development of the “General Child Development Screening in the National Context” Deliberative Dialogue (DD). The objective of this dialog was to contribute to the formulation of a policy for the selection of a developmental screening instrument for use in Growth and Development Monitoring services, based on scientific evidence. In addition, this study investigated the factors influencing its implementation and strategies to approach it.
This paper reports the experience of a DD conducted at the height of the pandemic, an evaluative exercise to select the most appropriate screening instrument for monitoring the growth and development of children in health facilities in Peru.
Methods
Pre-selection of evidence
A comprehensive search of national and international evidence on developmental screening instruments was conducted from January to March 2020, including gray literature and taking major international databases as reference: Medline through Pubmed, Scielo, Cochrane Library, Epistemonikos, and TripDatabase. Words or phrases related to the subject, combined terms, free search terms, and specific terms related to the topics “psychomotor development,” “developmental assessment tools,” “developmental screening,” “screening,” “child development,” and “screening tools” were considered for this search. Moreover, the web pages of organizations and repositories of guidelines related to child development were reviewed. The search was conducted for information on the following criteria: (a) evidence of use in the Peruvian and Latin American context; (b) availability of the instrument in Spanish; (c) experience of use or knowledge by sectors; and (d) evidence of characterization of the psychometric properties. From this study, a preliminary list of 11 general child development screening instruments was obtained: (1) Peruvian Developmental Test (TPED, Spanish acronym)12; (2) Evaluation of Psychomotor Development Scale (EEDP, Spanish acronym)13; (3) Test of Psychomotor Development (TEPSI, Spanish acronym)7; (4) Evaluation of Child Development (EDI, Spanish acronym)14; (5) Global Monitoring of Child Development (GMCD)15; (6) Ages and Stages Questionnaire—Third Edition (ASQ-3-3)16; (7) Abbreviated Developmental Scale—Third Edition (EAD-3-3, Spanish acronym)17; (8) Test of Infant Development and Learning (TADI, Spanish acronym)18; (9) Pikler-Lòczy Institute Developmental Scale19; (10) Denver-II Developmental Screening Test (DENVER-II)20; and (11) National Screening Test (PRUNAPE, Spanish acronym)21.
A summary of the evidence for each of these instruments was developed in the form of a matrix and included information on multiple aspects (Table 1).
Table 1 Information collected for each of the 11 instruments
| Author | Cost of tools and materials |
| Year | Cost of scoring materials |
| Language | License/permit requirements |
| Countries of use | Validation study/sample size |
| Type of instrument | Test-retest reliability |
| Domains evaluated | Inter-rater reliability |
| Definition of domains | Concurrent validity |
| Age range | Specificity |
| Periodicity of evaluation | Sensitivity |
| Evaluator/scorer | Administrators |
| Type of appraisal | Training duration |
| Administration time | Educational requirements |
| Scoring time | Cost of training |
| Number of items | Availability of online training |
| Type of response | Remarks |
| Score | Key references |
| Score interpretation | |
| Description of items | |
| Example item | |
| Required reading level |
The matrix with information from the 11 selected instruments was delivered to the multi-sectoral panel of specialists from three sectors (Ministry of Health, Ministry of Education, and Ministry of Development and Social Inclusion) for review and analysis, both independently and by teams (grouped according to their belonging to a particular sector), and always with the option of consulting other relevant sources of information.
The review criteria were: (A) importance and priority of the instrument for assessing the development in children under 5 years; (B) certainty of the available evidence about the instrument; (C) acceptability; and (D) feasibility. The teams also considered other relevant aspects for the selection or rejection of instruments. Each criterion was evaluated by questions with closed-ended and categorized answers, namely: (a) No; (b) Probably not; (c) Probably; (d) Yes; (e) Depends; (f) I don’t know. This is how teams were able to establish a priority ranking of three instruments. Third place was taken by the EAD-3-3, whereas the ASQ-3-3 ranked second, and the EDI test was at the top position, as all three teams were unanimous.
Deliberative dialog methodology
Deliberation is a collaborative process supporting the construction of common agreements, allowing re-evaluation of assumptions, highlighting strengths and broadening perspectives on particular issues to lead consensual decision-making processes, and assuming a set of recommendations based on evidence22.
DD is a group process of transformative discussion based on scientific evidence with the potential to address the challenges faced by policymakers and stakeholders while using information derived from research. These challenges primarily center on the observation that the information available to decision-makers is not always pertinent to the issues they encounter. In addition, it is often difficult to access, utilize, or translate this information into tangible action. DDs overcome these barriers and facilitate evidence-based decision-making by creating opportunities for policymakers and stakeholders to discuss, contextualize, and determine the meaning of evidence related to knowledge and experience, and provide policymakers with relevant knowledge for timely and actionable decisions23. The attainment of these objectives is contingent upon three factors: establishment of an appropriate environment, convocation of an adequate and representative group, and use of evidence.
This brings us to the central question of deliberation: What is the most appropriate screening instrument for the monitoring of growth and development in public health facilities nationwide?
PREPARATION OF DELIBERATIVE DIALOG
A document was developed containing a synthesis of the evidence on the instruments obtained in the pre-selection priority ranking. This document was to be read and reviewed before the DD sessions. Thus, the participants had a common basis from which to begin deliberation and consider the relevant24 evidence. Considering the need to hold virtual sessions due to the pandemic restrictions, a convenient date and time were decided, a technical support team was formed for the sessions, and an agenda was scheduled.
Methodologically speaking, adaptations were made to the method proposed by Acosta et al. (2018)25 and Boyko et al. (2012)23. The preparation of the DD was carried out with logistical support from UNICEF between March and June 2020. This support was part of the process of updating the Developmental Assessment Instruments in the Technical Health Standard for the Control of Growth and Development of Children under 5 Years of Age. This work was conducted within the framework of the Budget for Results with a focus on this topic26. During planning, potential participants were selected based on four criteria (Table 2) that could guarantee representativeness, the ability to articulate different points of view, experiences, and the interests of the represented groups, and a strong motivation to engage with the topic.
Table 2 Selection criteria for participants
| Health professionals with specialized knowledge and experience in child development, especially in developmental assessment. |
| Policymakers and authorities (public officials and administrators) of institutions related to child development. |
| Researchers or academics from research institutions and national and international universities with a primary focus of child development and related topics. |
| Organizations and societies related to early childhood work. |
The potential participants were invited to participate through a letter including information regarding the objectives of the activity and logistical details. Participants who confirmed their involvement completed a conflict of interest declaration form and were contacted through phone to provide information about the event’s agenda. Reminders were also sent through e-mail and text messages one week and one day before the agreed date. A communication channel was used to answer questions or doubts and increase participants’ commitment to the process. The composition of the sample is presented in table 3.
Table 3 Sample composition
| Sex | |
| Male | 4 |
| Female | 21 |
| Group | |
| Health professionals with specialized | |
| knowledge and experience in child development, especially in child development assessment. | 6 |
| Policymakers and authorities (public officials and administrators) at institutions related to child development. | 6 |
| Researchers from national and international research institutions and universities | 7 |
| Representatives of early childhood organizations | |
| Type of institution | |
| Public | 14 |
| Private | 11 |
The design was entirely virtual and the moderators and reporters were designated in advance from among the members of the technical support team. They were instructed to create an atmosphere of meaningful communication among participants, confidence in expressing themselves, and fairness in the interventions. Furthermore, they were instructed to maintain neutrality and not influence the discussion23. As the virtual format was new at the time, the organizing team tested the technical issues in advance.
DEVELOPMENT OF DELIBERATIVE DIALOG SESSIONS
In August 2020, two remote sessions were held one week apart. The first session provided an overview of the purpose of the dialog and its importance by focusing on selecting a developmental screening instrument to be included in the update of the respective regulations. In addition to the assessment tool, the agenda, methodology, and practical and confidentiality provisions were provided (Supplementary Material). The five groups comprised five members each (25 participants), accompanied by a moderator and reporter (both from the technical support team not involved in the deliberation). They were designated a group secretary to complete the responses in the assessment format in the four domains and each of the three instruments (EDI, EAD-3, and ASQ-3) and to present the group’s final decisions. The criteria evaluated were: (A) importance and priority of the instrument in the assessment of development in children under 5 years; (B) certainty of the available evidence about the instrument; (C) acceptability; and (D) feasibility and implementation aspects.
Some guidelines were provided to adequately manage dialog, maintain the structure of the discussion, and create an environment where participants could freely express themselves (Table 4). At the end of the deliberation, the participants summarized the comments, opinions, and suggestions, and a plenary session was held.
Table 4 Important guidelines for deliberative dialog
| All participants are invited to intervene, none will be excluded. |
| It is not acceptable for one or two participants to dominate the discussion. |
| Participants are requested to listen to each other. |
| The deliberation will focus on the three developmental screening instruments. |
| Facilitators ensure to maintain a conducive environment for deliberation, respecting and tolerating discrepancies. |
During the deliberation, the participants analyzed and responded, guided by the moderator, focusing on the advantages and limitations of each instrument, as well as the potential barriers to their implementation. The sessions were recorded with prior consent. Observations, comments, and feedbacks were collected from each group. At the end of the first session, all notes and transcripts of the reporters were compiled, and the recordings were reviewed. The organizing team convened a debriefing meeting to analyze and synthesize the information collected. A report of the analysis was subsequently prepared and presented in a second session and participants were invited to ask queries (Table 5). They were also asked to provide observations, suggestions, or recommendations, emphasizing the most significant aspects for implementation in the national context.
Table 5 Questions for participants
| What are the positive aspects/advantages of the instrument or its use? |
| What are the negative aspects/disadvantages of the instrument or its use? |
| Do you think that the instrument could be implemented in some health facilities of the second and third levels of care to support the diagnosis of developmental delay? Why? |
| What would be the potential barriers to implementation? |
| Which professional (s) could make use of the instrument? Please specify. |
| Based on your knowledge about the instrument and your experience using it, do you consider it important/necessary to implement it at the level of public health facilities? |
| How would a developmental assessment be conducted in the context of public health facilities in the event of the unavailability of these instructions? Would the clinical assessment of the child be sufficient? |
| How long does it take for you to apply the instrument? |
| Do you have any suggestions or practical indications for the application of the instrument? |
Results
The two aforementioned sessions ran smoothly in each group. The multi-sectoral organizing team worked diligently to achieve the objectives of the activity. The findings for each of the objectives are described below:
About the instrument
The importance and priority criterion was assessed by the question “Is the application of the test for screening during the control of child growth and development at the first level of national care a multi-sectoral priority?” For this criterion, the EDI instrument obtained the highest score on a Likert scale (range of answers from “Not a priority at all” to “Very high priority”) followed by the ASQ-3-3 and EAD-3. In the question “Is the application of the test useful for screening risks in child development at the national level?” the EDI instrument obtained the highest score, followed by the ASQ-3 and EAD-3 (responses ranged from “Not useful at all” to “Very useful”).
In the certainty of evidence criterion, in the question “Does the test demonstrate reliability and validity of evidence (sensitivity, specificity, test-retest reliability, inter-rater reliability, concurrent validity)?” the ASQ-3 instrument obtained the highest scores, followed by EDI and EAD-3 (Likert scale, with options from “Not reliable at all” to “Very reliable”). In the question asking about the balance between the positive and negative effects of the instrument, participants mentioned the EDI and ASQ-3 as the instrument with the most positive balance, followed by EAD-3 (responses ranged from “Not favorable at all” to “Very favorable”).
In the acceptability criterion, assessed through the question “How acceptable would the test be to key stakeholders (health personnel who will apply the test) in relation to benefits and costs?,” EDI obtained the highest score, followed by ASQ-3 and EAD-3 (Likert scale responses from “Not acceptable at all” to “Very acceptable”). Regarding the question, “Do you consider that decision-makers would accept the use of the test at the national level for reasons related to the resources required for its implementation (cost of the test, materials, or training)?” EDI scored the highest, followed by EAD-3 and ASQ-3 (response range from “Unlikely” to “Very likely”). In the question “Overall, how likely do you think it is that the parties involved (parents/caregivers/health personnel who will administer the test) would agree to apply the test?,” EDI scored the highest, followed by ASQ-3 and EAD-3 (responses ranged from “Unlikely” to “Very likely”).
In the feasibility and implementation criterion, in the question “How likely is it that the application of the test will be sustainable?,” the highest score was obtained by the EDI instrument, followed by ASQ-3 and EAD-3 (Likert scale with options from “Unlikely” to “Very likely”). The question “How likely is it that the significant barriers may limit the feasibility of implementing the test or require reconsideration when implementing it?,” the highest score was obtained by EDI, followed by EAD-3 and ASQ-3 (Likert scale with options from “Unlikely” to “Very likely”). In the question “In general, how feasible do you consider the implementation of the test on a national level considering the target group of the ECD Outcome-Based Budget Program?,” the highest score was obtained by the EDI instrument, followed by ASQ-3 and EAD-3 (responses ranged from “Not feasible” to “Very feasible”).
The overall score obtained for the EDI instrument was 196 points, the ASQ-3 was 146 points, and EAD-3 was 103 points. The summary of the scores based on the criteria is described in table 6. The vital arguments for this selection focused on the psychometric evidence of validity (“good sensitivity, acceptable specificity”), applicability in the Peruvian context, minimum cost, accessibility of the materials, and free use. There was a possibility that its administration may take a little longer than usual; however, “it would not imply a change in methodology in the way health personnel applies it.” Another argument put forth is that the test is administered through staff observation, enabling the identification of developmental risks and incorporating a neurological evaluation. Regarding its implementation, training, supervision, and monitoring, as well as the establishment of a care pathway for cases of developmental delay were considered important.
Table 6 Summary of scores based on the criteria and overall score
| Main criterion | Subcriterion | Test | ||
|---|---|---|---|---|
| EDI | EAD-3 | ASQ-3 | ||
| Importance and priority of the instrument | Multi-sectoral priority | 27 | 21 | 25 |
| Usefulness to screen for risks in child development on a national level. | 27 | 18 | 26 | |
| Certainty of evidence | Reliability and validity | 24 | 12 | 27 |
| Overall test results | 24 | 13 | 24 | |
| Acceptability | Acceptability for the health professional | 25 | 13 | 21 |
| Acceptability for decision-makers | 26 | 13 | 11 | |
| Feasibility and implementation | Sustainability | 24 | 13 | 15 |
| Likelihood of barriers or constraints on implementation | 21 | 7 | 6 | |
| Feasibility of implementation under the Early Childhood Development Result-Based Budget Program Framework | 25 | 11 | 17 | |
| Total score | 196 | 103 | 146 | |
The following main advantages of the EDI instrument were reported by the groups:
- It has psychometric evidence of validity and an acceptable level of reliability
- It is comprehensive, because it evaluates motor, social, cognitive, and language areas, in addition to risk factors and warning signs
- It uses a traffic light rating system to better inform parents
- Materials to be used are accessible and easy to implement
- The application time is appropriate
- The application is simple
- It covers the target period established in the guidelines of the Results-Based Budget Program for ECD
- It involves direct and indirect evaluation
- It is in Spanish
- Support documents are available, such as the Complementary Manual for the Application of the Child Development Evaluation Test, the Neurological Examination Manual for children under 5 years old at the first and second levels of care, and the Manual for the training of facilitators in the EDI
- The test “would not imply a methodological change in the way health personnel apply it.”
About implementation
The second objective was to identify the probable factors influencing the implementation of the selected instrument and the strategies to address them. The following aspects were considered when developing an appropriate implementation process:
TRANSFER PROCESS
Administrative processes and formalities must be considered before application to ensure free and sustained use of the test, which involves:
- Permissions for use must be requested from the developers who hold the copyright to the test
- Requests must be made, in addition to all arrangements for technical support from the development team in different phases of the implementation process
- The potential costs involved in the initial training process for developers must be assessed
- Requests and arrangements for initial training in the use of the test must be made.
TRAINING/COACHING
Training and coaching in the use of EDI were identified as key components to ensure effective implementation within the national context. According to the participants, adequate training is essential to standardize the conditions of administration, ensuring homogeneity in the formulation of the questions to the caregivers and the correct instrument application.
According to the findings, participants argued that training processes must meet certain characteristics:
- Since the test covers multiple axes, including neurological examination, it needs to be complemented with training in psychomotor development and neurological assessment, aimed at professionals in charge of CRED control at the first level of care.
- Training sessions should focus on practical workshops and include activities of application, correction, and interpretation of the instrument, promoting experiential learning.
- Training should incorporate parent and caregiver training, thereby strengthening their knowledge of child development and providing them with the tools to actively support their children and understand how to provide that support.
- The virtual modality is pivotal in facilitating access to “different levels, with intensive training in health facilities located in remote areas, where there is often only one health professional or even technical staff.” These trainings can be implemented through platforms like the National School of Public Health. To ensure the validity of dichotomous answers, it is essential to train professionals in the correct formulation of questions. Consequently, a standardization process must be established to favor optimal conditions for the application of the instrument.
Two main modalities are proposed to perform the training processes:
- Staggered, with the training led by master trainers or facilitators, such as those assigned by the Integrated Health Network Directorates and Regional Health Directorates and Management.
- Generalized, massive implementation through the National School of Public Health platform.
IMPLEMENTATION IN THE GROWTH AND DEVELOPMENT MONITORING SERVICES
Participants noted that, once the required permits are in place, the following aspects should be considered before implementation:
- Contextual adaptation through cultural and linguistic adaptation by reviewing possible barriers or other anthropological considerations.
- Revision of administrative aspects (effective application time within the CRED consultation, coding in records, development of indicators, etc.).
- Revision of logistical aspects (having the manuals in physical form, adaptation/acquisition of materials).
INCORPORATION IN THE UPDATE OF THE TECHNICAL HEALTH STANDARD FOR GROWTH AND DEVELOPMENT CONTROL
Regarding the integration of the EDI test within regulatory frameworks, its application should not be confined to its use as a screening instrument; instead, it should be incorporated into a comprehensive system for the identification of developmental delays, with a particular emphasis on the early detection and intervention of such issues. Within this system, other components complementary to the use of the instrument were proposed, which must be differentiated and correctly applied by CRED professionals):
- Developmental monitoring: use of an instrument specifically designed for continuous observation.
- Assessment: application of a gold standard instrument to enable a comprehensive evaluation of the level of developmental delay and the detection of an underlying diagnosis or condition.
- Intervention and care: implementation of a care pathway for detected cases of developmental delay, as well as decentralization of specialized care on a regional level.
- Furthermore, a review and selection of the ages of mandatory application was deemed necessary in the context of the update to the Technical Health Standard for Growth and Development Control.
IN-OFFICE USE OF CRED CONTROLS
The participants expressed the need to implement a comprehensive application with greater involvement of health professionals. The use of the instrument must be supported by specific training in communication and intercultural skills, thus ensuring the provision of effective and respectful care for families. Furthermore, the significance of incorporating physicians—as opposed to solely nursing professionals—was underscored, thereby promoting their active involvement in the detection and intervention processes for children exhibiting developmental delays.
STAFF TURNOVER AND WORKING CONDITIONS
The high turnover of healthcare providers in health facilities was a significant challenge as it can lead to interruptions in the application of the instrument. Many participants suggested taking necessary steps to maintain the permanence of the staff, provide greater job stability, and take charge of a sufficient number of nursing professionals so that care can be provided with greater peace of mind and diligence.
SUPERVISION AND MONITORING OF USE
This aspect arose recurrently during deliberation. It was considered essential to establish a system of supervision, monitoring, and follow-up, including the suggestion of re-evaluating the operation annually. Furthermore, pilot testing was recommended to determine the learning curve and adjust the implementation aspects. Other points to be considered include:
- Carrying out a validation study within a national context to confirm the psychometric properties described in the original study. Accompanying and monitoring the operational implementation as part of the support to the health professional until the implementation process itself becomes sustainable.
Other considerations reported by participants
- Its use may procure some level of complexity for people outside the field of health care or unfamiliar with pediatric care. In addition, it is recommended to provide a manual of guidelines for parents and caregivers, which provides them with access to practical tools to support the comprehensive development of children. This manual should also facilitate constant follow-up and training on child development. Although most of the participants consider EDI a simple and quick test to administer, some people regard it as “laborious” because it takes approximately 15 min, which may be excessive in the context of CRED Controls, considering the length of the consultation and the number of procedures to be performed during the consultation.
- An attitudinal barrier was identified, related to the acceptance in the change of instrument due to their greater familiarity with the tests in current use (TPED, EEDP, and TEPSI).
- The environment in which the application is to take place must be sufficiently spacious to allow for a comprehensive evaluation of the children involved.
- It is essential to implement “cascade sensitization,” starting with health professionals, parents, and health authorities.
- It was recommended that the topic of ECD be incorporated into the training of health professionals, beginning with the undergraduate level, to strengthen the competencies in this area. Moreover, comprehensive care-related aspects should be considered, such as the mother’s mental health, the family environment, the quality of the mother–child relationship, care time, and psychosocial risk. In addition, it is important to consider factors such as weight, height, and breastfeeding, and emphasize social development to rule out the suspicion of autism.
- Adequate advocacy is necessary to prioritize the above issue and promote a political decision translated into plans, strategies, and budget allocations to enable implementation and facilitate scaling up at the national level.
- The new instrument selected should be widely disseminated by appropriate means, ensuring technical training for health professionals, including attitudes, practices, and knowledge.
Discussion
The priority of having a screening instrument for the detection of developmental delays in children has been widely recognized as a fundamental approach in the national ECD policy for achieving the health outcomes proposed for children under 3 years. Instead of being an isolated intervention, the application of screening instruments should be a universal measure in primary health care that promotes the timely and effective identification of developmental delays and disabilities, ensuring prompt referral to specialized services within a system of care responsive to each child’s individual needs27.
In recent years, questions have arisen about the real usefulness and efficiency of the instruments used in our country because the past literature has not been able to establish their validity. The COVID-19 pandemic exacerbated this problem by significantly impacting growth and development monitoring services and the application of such instruments. This decreased the opportunities for timely detection of developmental delays. This scenario has prompted an immediate undertaking of efforts to establish an updated and adequate instrument. In the field of public health, DDs are useful for inspiring discussions, improving complex understanding, and fostering consensus on health priorities with the potential to address the challenges that policymakers and stakeholders face when using evidence23. The aforementioned process, under the leadership of the health sector and with the involvement of representatives from the education and social development sectors, has identified the necessity for support in making contextualized decisions on a national level. Other experiences of deliberative dialog have been developed in our country in the field of health, such as those promoted by the National Institute of Health to formulate recommendations for clinical practice guidelines28 and establish policies and interventions to reduce injuries caused by traffic accidents29. However, this is the first study that focused on child development in Latin America providing greater visibility to the urgency of detecting developmental risks and determining the need to implement a standardized screening instrument.
This exercise helped determine the selection of the EDI test as a developmental screening instrument for use in health services through the DD. It also helped recognize that this instrument is a viable option for rethinking the psychomotor development assessment strategy. As with our findings, previous reviews have highlighted the validity of the instrument, its accessibility, and its low administration time as positive aspects30.
Figure 1 shows the summary of the selection process. Overall, the EDI test scored the highest on the appraisal criteria, compared to ASQ-3 and EAD-3. Regarding the importance and priority of the instrument, the EDI test achieved scores similar to those of ASQ-3, a widely recognized international test, although the latter obtained a higher score in the certainty of evidence criterion. The EDI test also outperformed in the acceptability criterion, especially among decision-makers, which could be related to the fact that ASQ-3 has a high and restrictive cost for the Peruvian context, where there are fewer economic resources. A significant finding is that, although the EAD-3 has been recognized as a useful and priority test, it presents difficulties in terms of its sustainability, despite being an open-access instrument. Another relevant aspect is that the EDI test scored higher in the feasibility of implementation within the ECD Budget Program Framework, which is a priority for Peru.
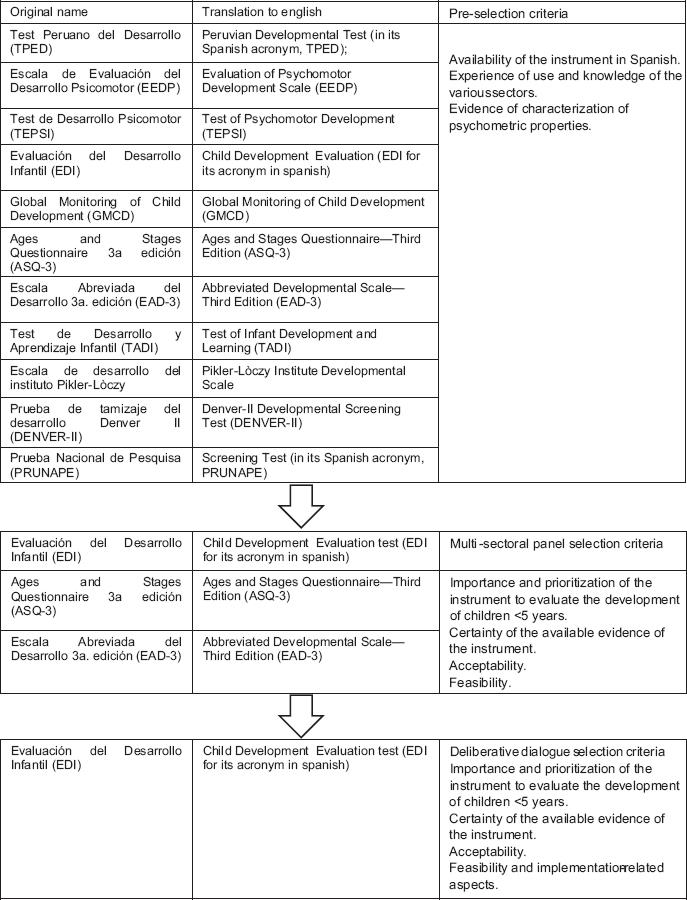
Figure 1 Summary of the selective process. The original name (acronym) in the native language of the screening test analyzed is shown together with its translation to English.
However, there are some limitations considered when interpreting the results. Although efforts were made to achieve the greatest possible representativeness in the sample and have a variety of participant profiles, the small sample size could limit the generalization of the results to a wider population. In addition, although participants were provided with a matrix with all the test information to facilitate evaluation, complete knowledge of the instruments cannot be guaranteed and previous experience in their use may be necessary for a more accurate assessment. The present study was conducted in August 2020, so there may be more recent evidence not included in this paper at the time of publication.
To guarantee the effectiveness of its implementation at the national level, it is essential to incorporate these characteristics in the normative documents, as well as in the processes of training, sociocultural adaptation, preparation of services, supervision, monitoring, and validation. All these aspects should be discussed and accounted for by the test developers to assess the suitability of the implementation and training processes before scaling up in the current context and considering the logistical and operational needs.
All these measures will ensure the reliability of the results obtained during implementation. It is imperative that screening be complemented by continuous developmental monitoring activities, performed by health professionals during regular contact with families and in congruence with them. This will assist in identifying children who require screening, even in the absence of specific psychomotor developmental concerns reported by caregivers.

