











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Early childhood caries (ECC) is a multifactorial disease that affects approximately 70% of pre-school children seeking dental care in Mexico1. Etiopathogenesis of ECC involves the interaction of community, family, and host-specific factors2. Low socioeconomic status3, social disadvantages4, mother's educational level and emotional state5-7, oral hygiene8, transmission of Streptococcus mutans9, and cariogenic diet10 are some of the factors that contribute to this disease. When caries reaches advanced stages, it can be limiting and affect the childs growth and development11.
In 2019, the World Health Organization (WHO) published the implementation manual: "Ending Childhood Dental Caries," which outlines action plans aimed at preventing and controlling ECC12. One proposed alternative is silver diamine fluoride (SDF), a high-concentration fluoride solution composed of silver, ammonium, and fluoride, which acts as an antimicrobial, cariostatic, and remineralizing agent13.
ECC is a significant public health problem that requires resources for designing effective prevention and control programs. However, in the health sector, needs are infinite while resources are increasingly limited. Mexico's health investment of approximately 3% of its gross domestic product falls short of the 6% recommended by the WHO14.
Economic evaluations are key decision-making tools that allow for the assessment of programs in terms of costs and consequences, with the aim of promoting more efficient use of resources in a scarcity environment15.
The objective of this research is to analyze the available information on the cost-effectiveness of SDF as a public health intervention in the prevention and control of ECC.
Method
A scoping systematic review was conducted, following Arksey and O'Malley's methodology16.
All articles published in indexed journals in English were selected, regardless of publication year. The review included all cohort studies and clinical trials reporting the cost and effectiveness of SDF in pre-schoolers. Furthermore, included were economic evaluations using any cost-effectiveness model and any treatment alternative in the control group for ECC prevention. Cost minimization or cost-utility economic evaluations focused on other pathologies or age groups were excluded.
The following search engines were used: Scielo, PubMed, Free Medical Journal, Science Direct, Springer Link, and Google Scholar. The information collection was conducted by three researchers working independently. The search was carried out from May 1 to May 26, 2024. The keywords used were: ECCs, effectiveness, cost, SDF, economic evaluation, caries, pre-school, infant, minimal invasive treatment.
The sample, phenomenon of interest, design, evaluation, research acronym was used to create the search strategy17. S: study population (preschoolers); PI: cost-effectiveness of SDF in the prevention and control of ECCs; D: all original publications with quantitative methodology addressing the phenomenon of interest were considered; E: the search strategy was not limited to the evaluation (E) of the publication, as a limited number of articles was found; R: all studies related to the topic of interest were selected.
The titles and abstracts from the initial search were evaluated by an independent researcher. Duplicate articles and those unrelated to the study objective were excluded. A list containing the author, title, and publication link was created in Microsoft Excel for data extraction.
Thorough evaluation and data extraction of the filtered articles was conducted by four researchers working collaboratively. The extracted data included: author, study publication year, study objective, study population, design, analysis perspective, options to compare, time horizon, discount rate, costs, and effectiveness evaluation.
The quality of selected articles was individually evaluated using M. Drummond's criteria18 for conducting economic evaluation studies; observational studies were evaluated using the strengthening of the reporting of observational studies in epidemiology guidelines19 and clinical trials using the CONSORT guidelines20. In addition, the grading of recommendations, assessment, development, and evaluation (GRADE) methodology was applied to evaluate the quality of scientific evidence21 (Table 1).
Table 1 Characteristics of incluided studies
| Authors | Year of publication | Study objective | Study population | Study design | Analysis perspective | Comparison options | Time horizon | Discount rate | Costs | Effectiveness | Evaluation guideline | Quality of evidence GRADE |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Xiao et al. | 2008 | Investigate the cost-effectiveness of four methods in caries prevention of pits and fissures in permanent teeth | 161 Children from first to third grade in Shenzhen, China | Clinical Trial | Health Provider | FS: pit and fissure sealant resin ART: technique TRA NaF: sodium fluoride every 6 months SFD: annual application of silver diamine fluoride | 18 months | N/R | FS: US $0.3 ART: US $1.0 NaF US $0.3 SFD: US $0.7 Cost per tooth treated | FS: 97.3% ART: 97.2% NaF: 96.4% SFD: 98.7% (Chi-square test, P≥0.05) | CONSORT | High |
| Hansen et al. | 2017 | Estimate the impact of adopting treatment with silver nitrate/fluoride varnish on dental care costs and resource utilization | 18,110 children 4612 Children treated with silver nitrate/fluoride varnish 13498 Children with conventional treatment. | Retrospective cohort | Health provider | SN/FV Group of silver nitrate+fluoride varnish C: group with conventional treatment | 28 months | N/R | SN/FV: $1455.9 ± 1125.1 dollars C: $944.7 ± 1192.4 dollars (p ≤ 0.0001) | In the 28-month term, the number of dental consultations was higher, by 21%, in the Silver nitrate group compared to conventional treatment | STROBE | Low |
| Hansen et al. | 2019 | Evaluate the impact of silver diamine fluoride considering coverage and reimbursement policies | 117,599 pediatric patients from Oregon | Retrospective cohort analysis | Health provider | Medicaid=Inclusion of SDF in Medicaid EPDHS: use of SDF by expanded-function dental hygienists | 4 years | N/R | Costs of care Medicaid= −$7.73/1,000 patients/quarter EPDHS: −$201/1,000 patients/quarter | Utilization rate Medicaid: 84 more SDF treatments/1,000 patients per quarter EPOHS: −91.7 SDF treatments/1,000 patients per quarter | STROBE | Moderate |
| Davis et al. | 2020 | To compare dental care visits, procedures, and expenses between children with newly diagnosed early childhood caries who received and did not receive SDF. | 354 children under 6 years of age 104 with silver diamine fluoride 250 without silver diamine fluoride | Retrospective cohort study | Healthcare provider perspective | SDF = treatment with silver diamine fluoride Without SDF: conventional treatment | 2 years | N/R | General treatment expenses excluding subjects requiring general anesthesia SDF: $USD 619.72 ± 563.5 without SDF: $USD 958.04 ± 824.6 p = ≤ 0.001 | Average treatment effect on the treated (ATET): 515.30 (cost-benefit) | STROBE | Low |
| Nguyen et al. | 2022 | To develop a cost-effectiveness model for a silver diamine fluoride intervention protocol compared to general anesthesia in Victorian children aged 2-10 years | 102 Children aged 2-10 years 85 with silver diamine fluoride 5 lost to follow-up 12 general anesthesia | Cohort study | Healthcare provider perspective | GA: treatment under general anesthesia. C: conventional treatment without general anesthesia. Base scenario: Children who received SDF in standard care without general anesthesia. Alternative scenario: SDF without standard care and without general anesthesia | 1 year | N/R | GA: $1793.23 Australian dollars C: $409.90 Australian dollars SDF: $190.81 Australian dollars in the first session $131.24 Australian dollars in second session | Children SDF in standard care without general anesthesia: Average savings of $171.01 AUD per child/mean effectiveness 0.298 of general anesthesia avoided per year. Children SDF without standard care without general anesthesia = average savings of $518.50 AUD per child/mean effectiveness 0.300 of general anesthesia avoided per year | STROBE | Low |
| Kodali et al. | 2022 | To analyze the cost-effectiveness of silver diamine fluoride compared to glass ionomer followed by 5% fluoride varnish application | 187 children aged 1-5 years Group A: 91 children Group B: 96 children | Randomized clinical trial | Healthcare provider | Group A: Prophylaxis + 38% SDF Group B: Prophylaxis+glass ionomer restoration + 5% sodium fluoride varnish application | 6 months | 3% | Global costs: Group A: $20,583 Group B: $34,369 (with discount rate). Group A: 67.30 Indian rupees to convert one active carious tooth to inactive Group B: 225.5 Indian rupees to convert one active carious tooth to inactive | Group A: 144 teeth with active caries after intervention Group B: 66 teeth with active caries after intervention. Incremental cost-effectiveness ratio was 89.9 (Per tooth inactivated with SDF) | CONSORT | High |
| Aly et al. | 2023 | To compare the clinical performance and cost-effectiveness of SMART technique versus conventional atraumatic Restorative Treatment (ART) in primary molars after 12 months of follow-up | 55 children aged 5-9 years SMART: 29 children (50 molars) ART: 26 children (49 molars) | Clinical trial | Healthcare provider | SMART: modified ART with silver ART: conventional ART | 12 months | N/R | SMART: 60.5 ± 3.5 Egyptian pounds per tooth ART: 67.4 ± 4.1 Egyptian pounds per tooth p ≤ 0.001 | Clinical performance (mean survival time) SMART: 11.8 months ART: 11.6 months (p = 0.41). Mean treatment time SMART: 7.8 min ART: 15 min (p ≤ 0.001) | CONSORT | High |
ART: atraumatic restorative treatment; GRADE: grading of recommendations, assessment, development, and evaluation; SDF: silver diamine fluoride; SMART: silver modified atraumatic restorative treatment, STROBE: strengthening the reporting of observational studies in epidemiology.
Results
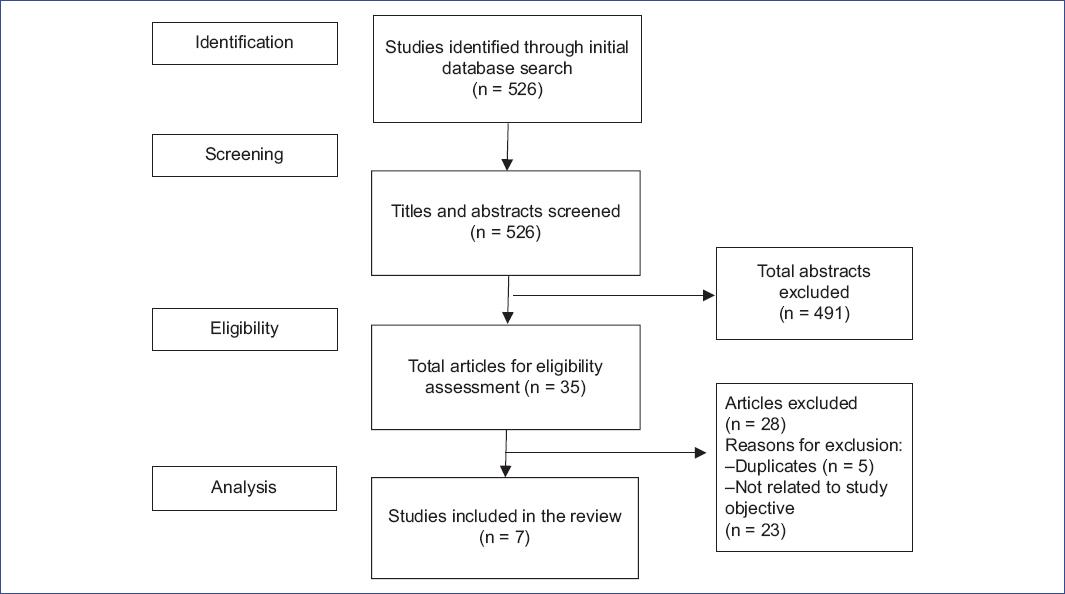
During the literature search, 526 articles were identified. 519 were eliminated (5 due to duplication and 514 due to lack of relevance to the study objective) (Fig. 1). The final sample consisted of 7 articles: 3 clinical trials and 4 cohort studies. The clinical trials obtained a high-quality level according to the GRADE methodology. Regarding the cohort studies, 3 obtained a low-quality level and one moderate (Table 1).
Xiao compared the cost-effectiveness of: (1) Pit and fissure sealant; (2) atraumatic restorative treatment (ART) technique; (3) Sodium fluoride; and (4) SDF. Over an 18-month time horizon, the most economical preventive treatments per tooth were sodium fluoride at US$0.3 and pit and fissure sealant at US$0.3. No statistically significant differences were found in the effectiveness of the treatments (p ≥ 0.05)22.
Hansen estimated the impact of adopting silver nitrate and fluoride varnish treatment on dental care costs. They identified a total cost of US$1456 in the group treated with silver nitrate + fluoride varnish and US$945 in the conventionally treated group, over a 28-month time horizon (p ≤ 0.0001). The most expensive treatment with the highest number of appointments was silver nitrate + fluoride varnish23.
Two years later, Hansen evaluated the impact of SDF considering coverage and reimbursement policies in two study groups: (1) incorporation of SDF in Medicaid and (2) use of SDF by expanded practice dental hygienists. Greater savings were found when SDF was applied by dental hygienists (−US$201/1000 patients/quarter). However, the application of SDF through Medicaid showed a higher utilization rate24.
Davis compared the cost-benefit of children treated and not treated with SDF. In the SDF-treated group, an average of US$ 619.72 ± 563.51 was spent, and without SDF US$ 958.04 ± 824.65 (p ≤ 0.001). The average treatment effect on the treated was −515.30 (cost-benefit). The savings obtained after the SDF application were significant25.
Nguyen estimated the cost-effectiveness of: (1) Treatment under general anesthesia; and (2) Conventional treatment without general anesthesia (through a decision tree model where the base scenario was the application of SDF in standard care without general anesthesia and the alternative scenario was the application of SDF without standard care and without general anesthesia). In the base scenario, the average savings were $171.01 AUD/child/mean effectiveness 0.298 of general anesthesia avoided per year, and in the alternative scenario, the average savings were $518.50 AUD/child/mean effectiveness 0.300 of general anesthesia avoided per year26.
Kodali analyzed the cost-effectiveness of: (1) prophylaxis + 38% SDF and (2) prophylaxis + glass ionomer restoration + 5% fluoride varnish. The most economical intervention was SDF with a cost of 67.30 Indian rupees to convert a tooth from active to inactive caries. The incremental cost-effectiveness ratio was −89.9 (for each tooth treated with SDF, there was a saving of 89.9 Indian rupees)27.
Ali compared the clinical performance and cost-effectiveness of: (1) modified ART technique with SDF (silver-modified atraumatic restorative treatment [SMART]) and (2) conventional ART technique. The SMART technique showed greater savings (60.5 ± 3.5 Egyptian pounds per tooth compared to the ART technique 67.4 ± 4.1 p ≤ 0.001) with shorter treatment time28.
Discussion
SDF is a cost-effective public health intervention for ECC control. Three clinical trials and 4 cohort studies were included. All studies used the healthcare provider perspective. The time horizon periods ranged from 6 months to 4 years. The treatment options against which SDF was compared were resin pit and fissure sealants, ART technique, 5% sodium fluoride, glass ionomer, conventional treatment, and conventional treatment under general anesthesia. Only Kodali's study used a discount rate of 3%27. Different currencies were used to report costs: US dollars, Australian dollars, Indian rupees, and Egyptian pounds. The range of intervention costs with SDF was from $0.7/tooth to $1456 total cost. The effectiveness measures reported were incremental cost-effectiveness ratio, cost-benefit, average cases of general anesthesia avoided per year, mean survival time, and mean treatment time.
When comparing SDF with pit and fissure sealant and sodium fluoride, a lower cost was identified in these treatment alternatives (US $0.3) compared to SDF (US $0.7). There were no significant differences when comparing the effectiveness between SDF (98.7%) versus sealant (97.3%) and sodium fluoride (96.4%). The most expensive treatment alternative was the ART technique22.
Silver nitrate is an inorganic salt with the chemical formula AgNO3. This component, similar to SDF, has bactericidal and antimicrobial properties29,30. In the field of Dentistry, its use has been incorporated in the treatment of dental caries31.
When comparing costs between silver nitrate application and conventional restorative treatment, there is a higher cost of care in the AgNO3 group (US$1456 versus US$945). The increase in care costs is likely due to a higher number of consultations in the silver nitrate-treated group compared to conventional treatment23.
Medicaid is a national program that, through the State, provides free or low-cost medical care to people of all ages with limited income and resources. Medicaid program names vary by State. Oregon's program is the Oregon Health Plan (OHP).
The OHP provides medical care coverage for residents who meet eligibility criteria. Coverage includes doctor visits, hospital care, mental health services, dental care, and additional benefits for children and pregnant women32. Among the dental services offered by the OHP program is antimicrobial treatment for caries arrest with the application of 38% SDF33.
Hansen evaluated the impact of SDF considering coverage and reimbursement policies. When incorporating the SDF application into Oregons Medicaid program, a savings of US$7.73/1000 patients/quarter was obtained, and coverage of 84 more SDF treatments/1000 patients/quarter. The savings were greater when SDF was applied outside the program through expanded practice dental hygienists (US$201/1000 patients/quarter). However, coverage was lower (−91.7 SDF treatments/1000 inhabitants/quarter), meaning that despite having lower savings in SDF application through the Medicaid program, there is a higher demand for this treatment24.
On the other hand, Davis compared the average direct care expenses between children treated with SDF and those treated with conventional treatment. Savings of slightly more than US$300 were reported in children treated with SDF compared to conventional treatment (619.72 ± 563.51 versus 958.04 ± 824.65 p ≤ 0.001)25. This study coincides with the results reported by Nguyen, where greater average savings were observed using SDF, in addition to greater effectiveness in general anesthesia avoided/year26.
Glass ionomer is versatile cement that chemically adheres to dental tissues (enamel and dentin) and releases fluoride. It has been used as a restorative material, liner, pit and fissure sealant, in the ART technique, and as an adhesive agent in Orthodontics34.
SDF along with dental prophylaxis proved to have a lower cost compared to prophylaxis with glass ionomer restoration and 5% sodium fluoride application ($67.30 versus $225.5 Indian rupees, respectively). There was a saving of 89.9 Indian rupees for each tooth with caries that was inactivated with SDF27.
As previously mentioned, glass ionomer is used as a restorative material in the ART technique. This is a dental procedure that involves the removal of softened tissue through the use of manual instruments35. Some studies have implemented the application of SDF as an adjunctive material to the ART technique to ensure dental caries arrest before cavity filling36.
Aly compared the clinical performance and cost-effectiveness of the modified ART technique with SDF and the conventional ART technique. The ART technique modified with SDF proved to be more economical compared to the conventional one by almost 7 Egyptian pounds, and it also achieved a shorter working time for treatment application28.
Among the strengths of this scoping systematic review are: Information was collected about SDF (a public health intervention proposed by the WHO for the prevention and control of ECC); the direct costs and effectiveness of SDF after its application as a public health measure were disclosed from the healthcare provider perspective. In addition, each article was evaluated with the appropriate checklist according to its design and the GRADE methodology to assess the quality of evidence.
Its main limitation is the small number of published articles on the subject. In addition, when collecting information about SDF intervention costs from international sources, the monetary units are expressed in dollars or currencies other than Mexican pesos, so costs would need to be converted to our national currency.
Conclusion
There are a very small number of articles published in indexed journals that evaluate the cost-effectiveness of SDF used for ECC control and prevention. The quality of the clinical trials included in this review, considering the GRADE system, was high. Regarding the observational studies, they had moderate-to-low quality. Taking into consideration the results of the research included in this review, SDF is cost-effective compared to conventional treatment and treatment under general anesthesia.
Recommendations
It is recommended to conduct more studies evaluating the cost and effectiveness of health interventions to improve decision-making and, thus, optimize the use of resources while maximizing benefits.
Considering the results of the research included in this review, the incorporation of SDF into programs and public policies aimed at the prevention and control of ECC at the population level is recommended.

