











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Bone marrow transplantation represents a therapeutic option for refractory malignant neoplasms; one of the most frequent complications is graft-versus-host disease (GVHD). The cutaneous manifestation of this disease can be severe with generalized erythroderma, desquamation, and blisters that mimic toxic epidermal necrolysis (TEN). The variety that simulates TEN is extremely rare, occurring in approximately 0.4-1.2/million people, causing almost 100% mortality.
Clinical case
An 11-year-old female patient post-transplanted with hematopoietic stem cell transplantation from an unrelated donor with 100% human leukocyte antigen (HLA) compatibility, with a history of acute lymphoblastic leukemia with early relapse to bone marrow and central nervous system. On day +35, she developed a disseminated dermatosis on the head, trunk, and upper extremities, affecting the cheeks, anterior chest, and anterior aspect of the arms. The dermatosis was characterized by a plaque composed of macules and papules on an erythematous base with irregular and poorly defined borders, disappearing with digital pressure, with acute evolution, and associated with mild pruritus.
A skin biopsy was performed, which reported epidermal atrophy, basal layer vacuolization, focally confluent apoptotic keratinocytes, no vesicle formation, and a dermo-epidermal junction with mononuclear inflammatory cells arranged around blood vessels (Fig. 1).
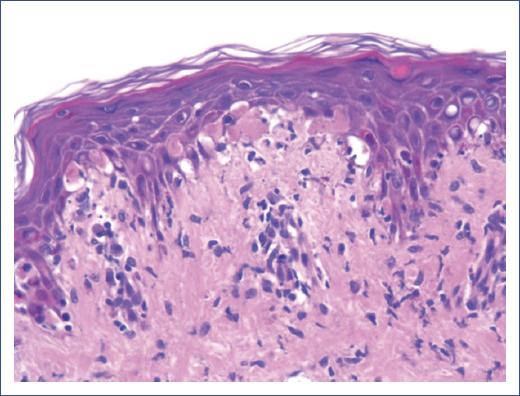
Figure 1 The image shows a section of the dermo-epidermal junction observed in a skin biopsy with hematoxylin and eosin staining. There is significant vacuolization of basal cells. A slight separation between keratinocytes is observed, suggesting intracellular edema. Keratinocyte necrosis is seen in the upper layers of the epidermis, indicating apoptosis. In the papillary dermis immediately adjacent to the epidermis, an inflammatory infiltrate composed predominantly of lymphocytes is observed. This is consistent with a T cell-mediated immune response, which is characteristic of graft-versus-host disease.
A disseminated dermatosis was observed, extensively affecting various body areas, including the head, face, ears, neck, anterior chest, arms, forearms, hands, thighs, and genitals. The morphology of the lesions was heterogeneous and characterized by the following findings: erythematous plaques formed by the confluence of macules and papules. The macules were erythematous, flat, and non-palpable, while the papules were raised and also erythematous. Both had well-defined and regular borders. In addition, flaccid blisters were present, indicating an intraepidermal or subepidermal lesion. Furthermore, a positive Nikolsky sign was observed, where applying pressure or rubbing on apparently healthy skin induced epidermal detachment, indicative of severe epidermal fragility (Fig. 2).

Figure 2 Day +55 post-hematopoietic stem cell transplantation: The lesions significantly affect the skin of the scalp, face, neck, and upper chest. Extensive areas of diffuse erythema with multiple erosions and ulcers are visible, some showing adherent hematic crusts. There are also areas of epidermal detachment, suggesting a severe cutaneous compromise.
Upon admission, the patient received systemic steroid treatment at 2 mg/kg/day; however, due to a poor evolution, immunomodulatory management was initiated with Sirolimus 1 mg/kg/day, Tocilizumab 8 mg/kg (4 doses), Infliximab 5 mg/kg (7 doses), Ruxolitinib 5 mg every 12 h, and human immunoglobulin 2 mg/kg (3 doses). At the time of this report, on day +65, the patient showed evident cutaneous improvement (Fig. 3).

Figure 3 Day +65 post-hematopoietic stem cell transplantation: The lesions are located in the lateral region of the neck, with partial extension to the upper chest. Erythematous and desquamative plaques with a rough appearance are observed. The skin shows areas of irregular hyperpigmentation, as well as patches of fine, dry desquamation, suggesting an inflammatory process.
Discussion
Acute GVHD is a multisystemic disorder that occurs within 100 days following hematopoietic cell transplantation. In this condition, donor T lymphocytes play a central role in the immunological attack on host tissues. The main risk factors include HLA incompatibility, prophylaxis regimen, intensity of the conditioning regimen, sex disparity between donor and recipient, cell origin, cellular inoculum number, and advanced age of the donor or recipient. The most important risk factor is the difference in HLA system antigens between the donor and the recipient1.
The cutaneous presentation initially shows an acral predilection, affecting the dorsum of hands and feet, palms, soles, forearms, face, ears, retro auricular area, and upper third of the trunk. Afterward, it can become generalized. Regarding morphology, it manifests as a maculopapular rash, with diffuse macules that blanch or a morbilliform rash. It can progress to erythroderma with a folliculocentric pattern; in rare forms, it presents with blisters1,2.
The patient’s case was initially classified as acute, presenting on day +35, and stage 1 according to the degree of involvement, initially affected 12% of the body surface area. It subsequently progressed, exhibiting characteristics of stage 4 due to the presence of blisters and denuded areas, affecting 50% of the body surface area, as well as a positive Nikolsky sign, despite management with systemic steroids and sirolimus. With these findings, a diagnosis of cutaneous GVHD of the TEN type was made, which is a rare and of poorly described complications3.
In the presence of TEN, it is important to rule out infections, which can also act as precipitating cofactors. Herpes simplex virus, some Mycoplasma species, mumps vaccine, and other genetic factors can act as predisposing factors in the pathogenesis4.
Treatment is multidisciplinary and based on the immunosuppression of donor T cells, which are responsible for the clinical manifestations of GVHD. Regarding the skin, first-line treatment for stages I and II includes topical steroids and calcineurin inhibitors, as well as symptomatic management with antihistamines. In cases of cutaneous and systemic involvement, systemic steroid management is suggested until resolution of the condition. If there is no response, human immunoglobulin, rituximab, infliximab, and extracorporeal photopheresis can be considered. Treatment may include steroids, monoclonal antibodies, JAK inhibitors, and immunoglobulin5.
In Mexico, no published studies have been found analyzing the incidence or mortality associated with this variant. An exhaustive search was conducted in scientific databases through the PubMed search engine, covering the past 10 years, without identifying relevant publications from Mexico.
Conclusion
A pesar de que la necrólisis epidérmica tóxica en el contexto de un trasplante de células progenitoras tiene una alta tasa de mortalidad, nuestro paciente presentó remisión de la sintomatología en un 80%, posterior al manejo dinámico de los inmunosupresores, lo cual demuestra que con un manejo oportuno y dinámico se puede mejorar la sobrevida de estos pacientes.

