











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Leukemia is a neoplasm of the hematopoietic system very common in the pediatric population1. It can also have manifestations in other organs, including the skin. The skin manifestations, called leukemia cutis (LC), are very heterogeneous and non-specific, it can also be present previous to the systemic manifestations even though it is rare. The most common type of leukemia associated with LC is acute myeloid leukemia (AML) and the least common pre B acute lymphoblastic leukemia (ALL). We report the case of a teenager who presented with facial edema and infiltration and systemic symptoms as the initial manifestation of pre-B ALL.
Clinical case
A previously healthy 14-year old male developed facial edema that worsened in the mornings and improved spontaneously during the evenings, associated with asthenia and adynamia. He consulted several physicians without obtaining any specific diagnosis or treatment; during this time, a complete blood count (CBC) was done and found to be normal. Due to persistent edema he was brought to our clinic 2 months later. Physical exam was notable for facial edema, diffuse indurated plaques affecting the cheeks, palpebral erythematoedematous plaques (Fig. 1), bilateral cervical, inguinal and axillary adenopathy, and splenomegaly. A new CBC was taken showing pancytopenia, and a chest X-ray revealed a mediastinal mass. Bone marrow (BM) biopsy was taken as part of the diagnostic protocol revealing small to medium cells with scarce cytoplasm, and immunohistochemistry (IHC) positive for TdT and PAX5. A skin biopsy of the cheek showed a dense dermal inflammatory infiltrate composed of atypical lymphocytes (Fig. 2A), IHC was positive for TdT and PAX5 and negative for CD56 (Fig. 2B). With these pathology results, pre-B ALL with skin infiltration (LC) was confirmed.
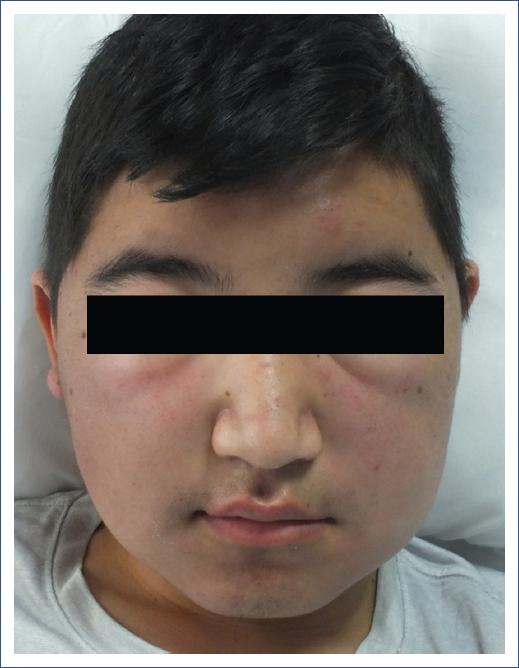
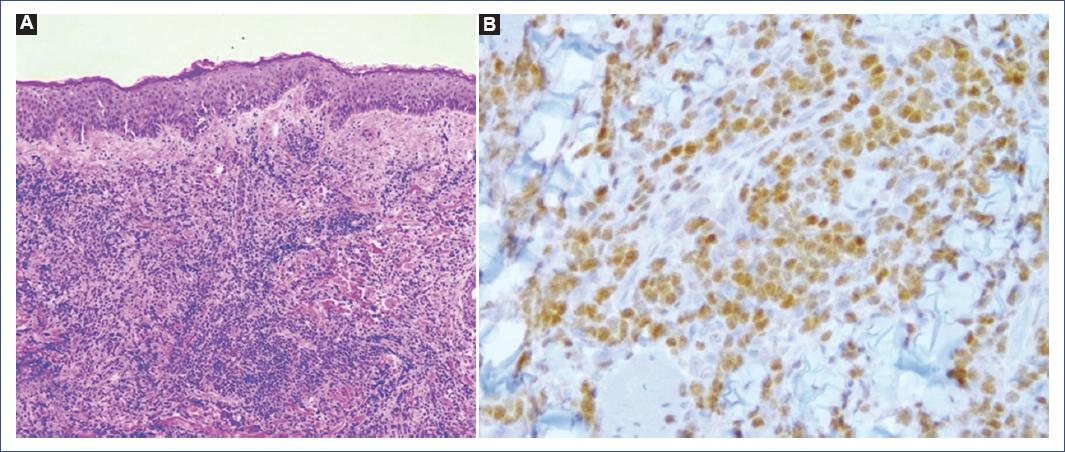
Figure 2 A: the dermis has a dense infiltrate of small blastic monomorphic cells (×10). B: inmunohistoquímica de Pax – 5 positiva para células blásticas linfoides de linaje B (×40).
The clinical differential diagnoses of facial edema and palpebral erythema include cellulitis, nephrotic syndrome, superior vena cava syndrome and parasitosis (such as onchocerciasis). The patient also presented facial induration and systemic symptoms which extends the differential diagnoses to include lymphoproliferative diseases infiltrating the skin. Pancytopenia and a mediastinal mass leads to a high suspicion of LC, confirmed by histopathology.
Discussion
ALL is one of the most frequent oncological diseases in children1, affecting the BM first and subsequently appearing in peripheral blood and other organs, including the skin2.
LC refers to cutaneous infiltration of neoplastic leukocytes (myeloid or lymphoid) and LC occurs more frequently in patients with myeloid leukemias, especially in subtypes with monocytic components (AML)1. Skin involvement is more common in children, occurring in up to 50% of patients with AML, 4-20% with chronic lymphocytic leukemia (CLL), and around 1-3% in ALL. It is particularly uncommon in pre B-cell ALL3,4.
Usually LC occurs after the diagnosis of leukemia (55-70%) and up to 30% patients have concomitant systemic and cutaneous involvement2,4. LC may also be the presenting sign of tumor relapse or recurrence and generally is a poor prognostic sign, however the exact survival rate of patients with LC secondary to pre-B ALL in unknown3,5. Aleukemic LC refers to cutaneous involvement without other manifestations, affecting up to 7% of patients, and may precede peripheral blood or BM disease for several months or years2.
The clinical presentation of LC is heterogeneous varying from hemorrhagic papules or violaceous nodules to plaques of different sizes; erythematous papules and nodules are the most frequently seen4. Different skin lesions can be seen in the same patient during the course of the disease. The most commonly involved sites are the extremities (particularly lower), followed by arms, back, chest, scalp, and face4. In pre-B cell ALL, the most common findings are infiltrated nodules and plaques on the head and neck5.
The diagnosis of LC is based on histopathologic findings characterized by: a Grenz zone (superficial dermis without any inflammatory cells), a lymphocytic infiltrate that can be perivascular and periadnexial or dense diffuse or nodular involving the dermis and subcutis, with numerous mytoses and necrotic cells3,4. IHC is important to determine the cell lineage. In ALL the B lymphoblasts are positive for CD79a, CD19, PAX - 5 and TdT, the combination of the last two being the most useful2,4. T lymphoblasts to CD1a, CD3, CD43 and TdT. CLL lymphocytes express CD5, CD19, CD20, CD432,4. In AML the most frequently used markers and are positive are: NASD, MPO, CD43, lysozyme and CD743,4. Additional to the skin biopsy, a BM biopsy as well as peripheral blood analysis is necessary to confirm the diagnosis3,4.
The treatment is aimed to eradicate systemic disease; systemic chemotherapy and local therapy, such as local radiation or surgery, is indicated4. At the same time as remission of hematological findings, there is partial or complete resolution of cutaneous manifestations2.
Conclusion
LC may present heterogeneously and is a poor prognostic factor in patients with leukemia3. The diagnosis should always be considered in patients with unexplained edematous or indurated lesions, innocent as these may look. The presence of LC in patients with pre-B cell ALL is extremely rare and only a few are reported in the literature.

