











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Lawrence Kohlberg developed his "Moral development theory" in 1958 while investigating the ability to elaborate moral judgements1,2. He asked participants to reflect individually on several dilemmas that presented value-based conflicts, and to make decisions to solve the dilemmas3,4.
Kohlberg concluded that moral reasoning develops in three levels: pre-conventional, conventional, and post-conventional5. Each level has two cognitively structured stages that determine the way an individual gathers and processes information4. To move from one stage to another, the development of intelligence and logical operations is fundamental, as well as the social perspective from which we decide what is right, and the motives to act in an appropriate way2. Intelligence is related to moral development, individuals with a lower intellectual level tend to have a lower moral reasoning level; however, individuals with higher intellectual levels do not necessarily have a higher moral reasoning level1.
In the pre-conventional level, there is an individualistic perspective, focusing mainly on the self-interest. In the stage one, individuals have a punishment-obedience orientation; and in the stage two, the most crucial factor is to follow rules according to self-interests and individual needs2.
In the conventional level, individuals manage moral problems from the perspective of being a member of a society, considering the expectations of the group or society for the individual as a member or as a role player. Individuals identify with the society, and the group rules are the defining point for their moral judgments. This level is usually reached during adolescence and keeps a predominant place in the moral reasoning of most adults in many societies1,2.
In the post-conventional level, individuals generally comprehend and accept the society norms as they are based in universal moral principles, such as the respect for life and the dignity of each individual. If these principles are in conflict with the society norms, the post-conventional individual will judge and act accordingly to their principles over the social conventionalisms1,4,6. In the stage five, the values and rights preceding the social contract are considered, and in the stage six, individuals must be acknowledged by themselves by universal ethical principles2.
One of the most often used instruments to evaluate moral reasoning is the defining issues test (DIT), designed by James Rest. It is the most comprehensive as it was developed using Kohlberg's moral development theory4,7.
Through their training, medical professionals learn that values and human lives must be preserved, as well as to respect the illnesses that they find in every patient8. The main objective of medical education is to develop an appropriate interaction of social skills9. Some Mexican educational institutions, including the National Autonomous University of Mexico, the National Polytechnic Institute, the Autonomous University of the State of Mexico, the Autonomous University of Guadalajara, the Anáhuac University, and the La Salle University, contemplate in their academic programs the teaching of ethics and bioethics, promoting the comprehensive training10-16; however, most of the ethical training of undergraduate and postgraduate medical students happens during their clinical practice, by observing other physicians and students from a higher echelon, which is often referred to as a "hidden curricula"17. Medical ethics, moral reasoning, and complex medical decisions are not a recent subject of discussion. Ethical dilemmas that rise during the medical formation generate questions that many times are not solved or even discussed with students8,9,18.
Pediatricians face many ethically challenging situations. Having to decide when to limit life prolonging treatments, disagreements with the child's family, and end of life discussions are frequent ethical dilemmas in pediatrics18. Ethical capacitation in this medical specialty may help to face ethical dilemmas in a better way19.
Some studies have studied moral reasoning among medical students and physicians. One study found a lightly lower P-index (PI) in medical interns compared with surgical residents (37.2 vs. 46)6,20-25. Another 2019 study found that most of 88 medical graduates were in 5a and 5b stages. This could suggest that as individuals have more medical practice experience, they reach a higher level of moral reasoning, which is beneficial to the patients' treatment and the quality of the medical attention provided5.
The aim of this study was to describe the level of moral reasoning among physicians who are about to begin the pediatrics residency course in a tertiary hospital.
Methods
This is a descriptive cross-sectional study that took place between 2020 and 2023. The study population included 223 physicians who were about to begin their 1st year of the pediatrics residency course in a tertiary hospital. All physicians were invited to participate. All participants who were about to begin their 1st year of the pediatrics residency course and accepted to participate were included in the study. Participants from other hospitals who were in temporal rotations in the hospital were excluded from the study.
The study was explained to participants and an informed consent was obtained from all of them. Participants were asked to respond a socio-demographic questionnaire including general information about age, gender, and marital status, and to complete the DIT instrument26, which has been validated in Mexico among other Latin-American countries. The test validation has shown an adequate internal consistency, with a Cronbach's α = 0.71, and test-retest reliability of 0.657,26, similar to the original instrument designed by rest, which has a Cronbach's α = 0.70 and a test-retest reliability of 0.70-0.80.
The DIT consists of six stories in the original version and three stories in the brief version. The brief version was used in this study. Each story stands for a moral dilemma, and each story has three answering sections. In the first section, participants are asked for their opinions about the decision that the story's main character must make, the possible answers being "Agree," "Disagree," and "Indecisive." In the second section, participants must assign a level of importance in a five-point Lickert scale from "Not important" to "Very important" to 12 affirmations regarding the stories. In the third section, participants have to select the four affirmations from the second section that they consider to be the most important from each story and assign them a descending level of importance from one to four. Each of the 12 affirmations corresponds to a moral reasoning stage. Some examples of the affirmations include: "Community rules must be respected," "The pharmacist deserved to be robed for being cruel and ambitious."
The PI is used to classify the individual's moral reasoning in one of the three levels corresponding to Kohlberg's theory. A < 30 PI score in classified as a pre-conventional level, a score between 30 and 40 is considered as a conventional level, and a > 40 PI score indicates a post-conventional level.
With the answers from the three sections, a raw and a percentage score is obtained. The percentage score has a 0-100 scale to define the frequency in which each 2-6 sub-stage of moral reasoning is used. A raw and percentage score PI is obtained by adding the scores from 5a, 5b to 6 stages. The PI reflects an individual's tendency to use universal ethical principles to solve ethical dilemmas, which suggest that the individual may be in a post-conventional level.
On the other hand, a M score reflects an individual's tendency to consider meaningless affirmations as especially important. When this score is high, the level of participant's moral reasoning cannot be determined, and a higher than 16 score invalidates the test.
Statistical analysis
Descriptive statistics were used to describe sociodemographic variables. Qualitative variables were reported as totals and percentages, and quantitative variables were expressed with medians and maximum and minimum ranges. The quantitative DIT results (scores from stage 2 to 6 and IP scores) were reported with medians and maximum and minimum ranges. Qualitative DIT results (moral reasoning level) were reported as totals and percentages.
An exploratory inferential analysis was performed to compare the IP scores between the participants from different generations and socio-demographic variables with a Mann–Whitney U-test, and a linear X2 test was used to compare the levels of moral reasoning. Statistical analysis was performed using STATA v.24 software (STATA Corp, College Station, TX). The statistical significance level was defined with two-tailed p < 0.05. Confidence intervals were determined at the 95% confidence level.
Results
A total of 218 physicians agreed to participate in this study. Five tests were invalidated for having a high M score, and 188 tests were eliminated for being incomplete. A total of 195 participants with valid tests and questionnaires were included in the study.
Socio-demographic characteristics from the 195 participants are resumed as a whole and sub-divided by participants' generations in table 1. The median age was 26 and ranged between 23 and 32 years. About 71.8% of participants were female, 92.8% were single, and 51.3% was born in Mexico City or nearby areas, while 5.6% came from another country to study, and 44.6% of participants lived with a roommate. About 73.8% of participants reported to profess a religion, 55.4% describing themselves as Catholics, 2% as Christians, and 0.5% as agnostics, Buddhist, and others. The percentage of participants who began their specialty course in 2022 and 2023 (Generations 2022 and 2023) who reported professing a religion was higher than the one from Generations 2020 and 2021 (84% vs. ≈65%). The most frequent monthly family income bracket was $11,600-$34,999, and it was similar among generations.
Table 1 Sociodemographic characteristics of resident physicians categorized by generation and as a group
| Variable | 2020 (n = 47) | 2021 (n = 55) | 2022 (n = 46) | 2023 (n = 47) | 2020-2023 (n = 195) | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | Min-max | M | Min-max | M | Min-max | M | Min-max | M | Min-max | |
| Age | 26 | 23-20 | 26 | 24-31 | 26 | 23-32 | 26 | 24-28 | 26 | 23-32 |
| TN | % | TN | % | TN | % | TN | % | TN | % | |
| Gender | ||||||||||
| Female | 32 | 68.1 | 37 | 67.3 | 35 | 76.1 | 36 | 76.6 | 140 | 71.8 |
| Male | 15 | 31.9 | 18 | 32.7 | 11 | 23.9 | 11 | 26.4 | 55 | 28.2 |
| Marital status | ||||||||||
| Single | 41 | 87.2 | 53 | 96.4 | 44 | 95.7 | 43 | 91.5 | 181 | 92.8 |
| Common law | 6 | 12.8 | 2 | 3.6 | 1 | 2.2 | 4 | 8.5 | 13 | 6.7 |
| Separated | - | - | - | - | 1 | 2.2 | - | - | 1 | 0.5 |
| Practices a religion | 29 | 61.7 | 37 | 67.3 | 39 | 84.8 | 39 | 83 | 144 | 73.8 |
| Place of birth | ||||||||||
| CDMX and MA | 18 | 38.3 | 22 | 40 | 28 | 63 | 31 | 66 | 100 | 51.3 |
| Other state | 25 | 53.2 | 31 | 56.4 | 13 | 28.3 | 15 | 31.9 | 84 | 43.1 |
| Other country | 4 | 8.5 | 2 | 3.6 | 4 | 8.7 | 1 | 2.1 | 11 | 5.6 |
| Living situation | ||||||||||
| Parents | - | - | 21 | 38.2 | 18 | 39.1 | - | - | 39 | 20 |
| Other family | 14 | 29.8 | 1 | 1.8 | - | - | 12 | 25.5 | 27 | 13.8 |
| Alone | 6 | 12.8 | 7 | 12.7 | 2 | 4.3 | 8 | 17 | 23 | 11.8 |
| Roomates | 25 | 53.2 | 25 | 45.5 | 15 | 32.6 | 22 | 46.8 | 87 | 44.6 |
| Other | 2 | 4.3 | 1 | 1.8 | 11 | 23.9 | 5 | 10.6 | 19 | 9.7 |
| Monthly economical income | ||||||||||
| 0-2,699 | - | - | - | 5 | 10.9 | - | - | 5 | 2.6 | |
| 2,700-6799 | 4 | 8.5 | 3 | 5.5 | 1 | 2.2 | - | - | 8 | 4.1 |
| 6,800-11,599 | 1 | 2.1 | 12 | 21.8 | 5 | 10.9 | - | - | 18 | 9.2 |
| 11,600-34,999 | 15 | 31.9 | 15 | 27.3 | 14 | 30.4 | - | - | 44 | 22.6 |
| 35,000-84,999 | 8 | 17 | 16 | 29.1 | 16 | 34.8 | - | - | 40 | 20.5 |
| > 85,000 | 15 | 31.9 | 3 | 5.5 | 4 | 8.7 | - | - | 22 | 11.3 |
| Doesn't know | 4 | 8.5 | 6 | 10.9 | 1 | 2.2 | 47 | 100 | 58 | 29.7 |
M: median; Min-max: minimum-maximum; TN: total number; CDMX and MA: Mexico City and metropolitan area.
Moral reasoning analysis
The moral reasoning profile from the group was obtained for each stage (Fig. 1). The score medians were found to increase from stage 2 (0, 0-23.3) through 4 (36.6 0-70), and then decreased in stage 6 (10, 0-26.6). Statistically significant differences were found for stages 4, 5a, 5b, and 6 (Mann–Whitney U: p < 0.05). The median PI was 40, with a minimum-maximum range of 0-76.6. There were no statistically significant differences in the PI median across generations.
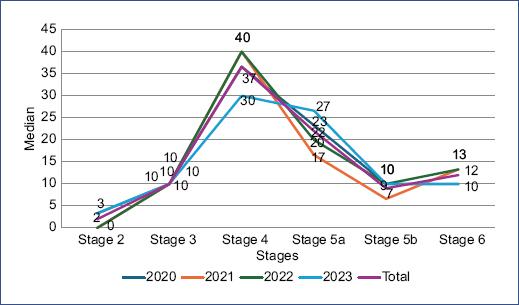
Figure 1 Medians of moral reasoning stages and P-index of resident physicians categorized by generation and as a group.
Moral reasoning development levels are shown in figure 2. Thirty-nine (20%) of the 195 participants were in a pre-conventional level, 61 (31%) were in a conventional level, and 95 (49%) were in a post-conventional level. The percentage of participants who were on a post-conventional level in Generation 2021 participants was lower than the one found in the other generations. This difference was not statistically significant.
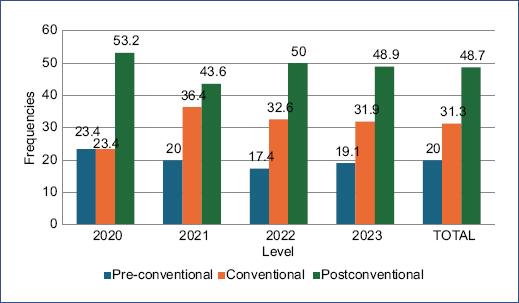
Figure 2 Percentages of moral reasoning levels of resident physicians categorized by generation and as a group.
As for gender differences, females had a PI median of 43 (0-76.6) while male participants had a median of 36 (16.6-66.6). The percentage of females who were on a pre-conventional, conventional, and post-conventional levels was 20.7%, 25%, and 54.3%, respectively, while the percentage distribution in males was 18.2%, 47.3%, and 34.5%, respectively. These differences were not statistically significant.
A PI median of 40 (0-76.6) and 43.3 (23.3-60) was found for single and married participants, respectively. About 47.8% of single participants and 62% of married participants were on a post-conventional level. This difference was not statistically significant.
There were no statistically significant differences between participants concerning religion or their monthly income.
Discussion
In this study, physicians who were about to begin their 1st year of pediatric residency training in a tertiary hospital had a moral reasoning PI median of 40, corresponding to a borderline place between a conventional and a post-conventional level according to Kohlberg's theory, where almost half of them were in the latter level. This finding differs from other studies where moral reasoning has been evaluated in other populations, such as non-medical bachelor's students and general population. In these studies, an average PI between 25 and 38 has been found, with most participants being in the conventional level27,28. On the other hand, the findings from this study are similar to those that evaluated moral reasoning among undergraduate medical students5,6,21.
Although the research about this subject is scarce, a previous study found significant differences between pediatric residents and recent graduates from other careers, where a 33.3 and 26.6 PI was found, respectively5.
In this study, the PI was similar across the different generations. This may be explained because all participants had been medical students at some point. Medical students frequently face difficult circumstances during their clinical practice that require from them to develop both a humanistic and a clinical perspective to make appropriate decisions for their patients, in which their conduct is based on professionalism and ethics.
One interesting finding from this study is that the Generation 2021 had a 10% lower percentage of participants in a post-conventional level compared to other generations. Although this difference was not significant, it is relevant to consider that this generation was measured after the 1st year of the COVID-19 pandemic, so the mental health consequences that this health crisis brought29,30 may have indirectly affected the residents' moral reasoning; thus, more research evaluating the impact of health crises in moral reasoning is needed.
A difference of more than 6 points between female and male participants' PI was found in favor of female participants. Although this difference was not significant, the magnitude of the difference is interesting, especially considering that the PI score of females (43) classified them in a post-conventional level, while the males' PI score (36.6) classified them in a conventional level. There are slight but non-significant differences in moral reasoning between men and women4,7, so it would be interesting to continue studying the gender variable in the future.
Healthcare workers face ethical dilemmas in a daily basis in which they must come up with functional answers, since many times the life of a patient depends on those answers. Precise decision-making is a highly important skill for training medical specialists to adequate their clinical practice in an ethical manner. The study and understanding of moral reasoning across different stages of medical education and comparing it to the moral reasoning of individuals with different professional careers might be useful to determine if there is an association between the individual's moral reasoning level and the probability to choose medicine as a career, as well as to understand morality and its' role in a society31.
Although formal ethics courses are offered in some medical residency programs, resident physicians truly delve into ethical and moral situations during their clinical practice, with their mentor's guidance. Professional conduct is shaped by many complex factors, which highlights the importance of cultivating "virtuous" ethics during the medical education. Ethical orientation and learning content should be present in every stage of the formative process17,32,33. Academic education during medical training is highly important for the development of clinical practice skills and medical ethics17. Resident physicians consider humanism to be fundamental to their formation, as well as the awareness of their own conditions and abilities to make appropriate decisions, since they think that by being aware of those factors, future medical specialists might improve their moral reasoning level, strengthening it with study and ethical basis. They also consider to be essential to develop ethical, moral, and medical knowledge in real situations for them to be able to apply this knowledge in decision-making11,13,16.
Ethical learning is not only a crucial component but also a cornerstone of medical education. It is imperative that structured and formal ethics and morals courses are available in all stages of the future physicians' education. It is required that students submerge themselves in real situations, where they can develop ethical abilities and be able to apply them in a practical way in decision-making, transcending the limits of the conventional clinical practice34,35.
Among the limitations of this study are that moral reasoning scores could have been affected by factors such as participants being sleep deprived among others. These factors were not controlled for the analysis. Another limitation is that the sample may not be representative of other populations. On the other hand, the instrument that was used to assess moral reasoning presents dilemmas concerning general situations, rather than medical context situations. A necessity to develop instruments including dilemmas contemplating specific medical scenarios arises for future research to assess the professionals' moral reasoning facing problems directly related to their job field. This approach could facilitate to determine if the dilemma's modifications contribute to significant variations in moral reasoning, providing a more precise and applied outlook of medical ethics in the clinical practice, for future research.
Conclusion
Physicians who were about to begin their 1st year of pediatric residency training in a tertiary hospital had a moral reasoning PI median of 40, corresponding to a borderline place between a conventional and a post-conventional level according to Kohlberg's theory, where almost half of them were in the latter level. The PI was similar between generations, although Generation 2021 had a lower percentage of participants in the post-conventional level, which could be explained by the COVID-19 pandemic onset.
An appropriate formative education during clinical medical training is essential for the development of clinical and ethical skills. Training physicians acknowledge the importance of the integration of humanism and moral reasoning in their learning process, and they highlight the importance of practical educational situations. Future research should study the influence of gender and other factors on the moral reasoning level of young adults.

