











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkA 29-year-old female with systemic lupus erythematosus was admitted due to persistent fever. Imaging studies and transthoracic echocardiography (TTE) were non-diagnostic for infectious foci. Salmonella Typhi was detected in three separate blood cultures, and an intravenous antibiotic was prescribed; however, the fever persisted and the blood cultures remained positive. Transesophageal echocardiography (TEE) revealed a low-density, thin, hypermobile, filiform lesion on the ventricular surface of the aortic valve, consistent with Lambl’s excrescence (LE) (Fig. 1A-E). Despite the TEE findings, the infectious disease department switched antibiotics, alleviating symptoms and resolving the fever. On the 14th day, blood cultures were negative, whereas follow-up TEE revealed no change in the filamentous structure. The patient was discharged symptom-free and completed 6 weeks of oral antibiotics without recurrence of fever. A 6-month follow-up TEE revealed no changes in the mobile structure or evidence of valvular disease (Fig. 1F and G).
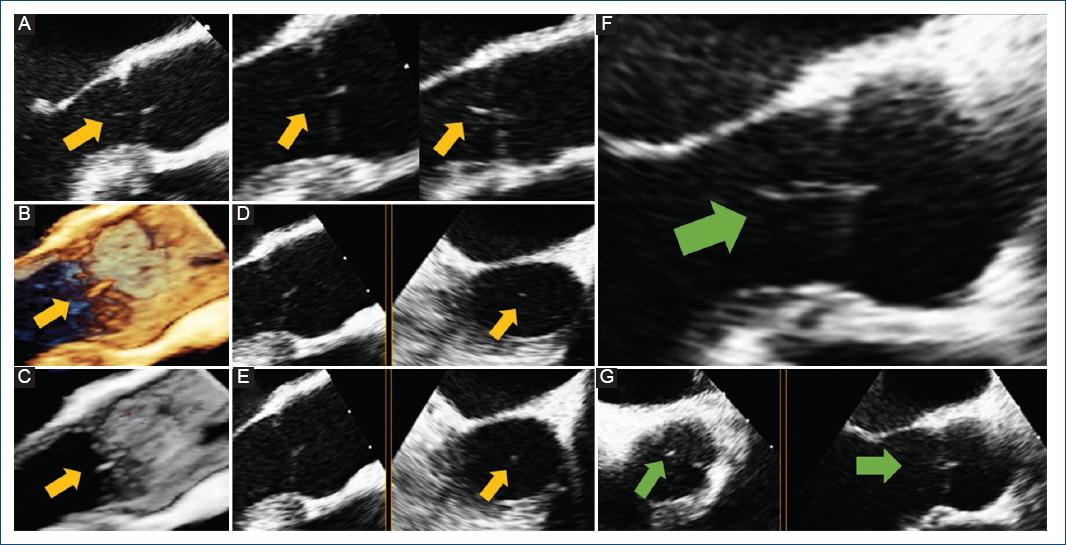
Figure 1 TEE shows Lambl’s excrescence on the aortic valve. Initial TEE (yellow arrow): A: mid-esophageal long axis view depicting a filamentous structure attached to the ventricle surface of the aortic valve; B and C: 3-D reconstruction; D and E: mid-esophageal long axis view in X-plane mode demonstrating the mobile structure in the left ventricular outflow tract. Follow-up TEE, 6 months later, showing no change in the linear mobile structure (green arrow): F: mid-esophageal long-axis view and G: mid-esophageal aortic valve short-axis view in X-plane mode. TEE: transesophageal echocardiogram.
Dr. Vilém Dušan Lambl first described LEs in 1856. Usually located at the Arantius nodules, these filiform structures (≤ 2mm thick and ≥ 3mm long), with hypermobility, originate at the closure margins of valve leaflets1,2. LEs are most common on the atrial surface of the mitral valve (68-76%) and the ventricular surface of the aortic valve (38-50%), and are rarely seen on native right-sided valves and prosthetic valves1,3. Endothelial injury caused by valvular wear and tear contributes to excrescence development1,2. The majority of LEs are asymptomatic and are found incidentally during echocardiography or autopsy2,3. Nevertheless, they are considered rare causes of thromboembolism, usually due to fragmentation or microthrombus formation on top of the lesions, more often in the excrescences of the aortic valve. TEE remains the gold standard for diagnosis, with greater sensitivity and specificity than TTE1,2. In light of the rarity of LEs, there is no standard management guideline2,3; asymptomatic patients should be closely monitored and followed up with TEE3, while patients with embolic events should be managed individually, considering antiplatelets, anticoagulants or surgery2,3. LEs should be considered in the differential diagnosis of infective endocarditis and other cardiac masses, with close monitoring and follow-up TEE in asymptomatic patients.

