











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkWe present the case of a 25-year-old female with hypertrophic obstructive cardiomyopathy (HOCM) who was successfully treated with endocardial radiofrequency ablation of septal hypertrophy (ERASH), achieving an excellent clinical outcome over 4 years. Hypertrophic cardiomyopathy is an inherited cardiac disease with a variable clinical course influenced by genetic mutations, familial patterns, and the severity of hypertrophy1. Clinical manifestations are dyspnea, heart failure, atrial fibrillation, and sudden cardiac death due to ventricular arrhythmias2. The left ventricular outflow tract (LVOT) obstruction is a significant cause of symptoms, mainly with gradients ≥ 50 mmHg3. ERASH is a novel procedure that offers advantages over septal alcohol ablation or surgical myectomy, such as independence of the coronary tree, targeted ablation at the obstruction site, less bloody technique since it does not cause an acute myocardial infarction or open heart surgery, and fewer complication rates4. Recent findings support the efficacy of ERASH in relieving symptoms by reducing LVOT obstruction gradient causing dysregulation of local contraction through radiofrequency (RF) ablation, documented by effective ablation points (index ablation) and hyperechoic image in the intracardiac echocardiogram, which represents the effectiveness of the acute lesion that furthermore become a fibrotic tissue.
A 21-year-old female who was diagnosed at 10 years old with HOCM underwent ERASH treatment. The clinical examination revealed a systolic 3/6 murmur in the third left intercostal space and signs of left ventricular hypertrophy on the electrocardiogram. Transthoracic echocardiography showed an ejection fraction (EF) of 61%, with LVOT peak gradients of 93 mmHg at rest and 122 mmHg during the Valsalva maneuver. TTE also indicated severe posterior wall/septum thickness (17/30 mm), septal, anterior movement (SAM) with moderate mitral regurgitation, and papillary muscle displacement. Cardiac magnetic resonance imaging revealed an EF of 72% and significant late gadolinium enhancement in the basal inferoseptal, mid anteroseptal, mid inferoseptal, mid inferior, and apical inferior left ventricle (LV) segments, comprising 29% of the myocardial mass, which is why a dual-chamber Medtronic ICD implanted for primary prevention. The patient underwent an ERASH procedure guided by intracardiac echocardiography (ICE) and 3-D electroanatomic mapping – the ERASH procedure performed under general anesthesia – ICE used for real-time visualization and guidance. Access to the LV septum was retrograde. Electroanatomic mapping (CARTO, Biosense Webster) was integrated with ICE to accurately localize the ablation targets and tag his bundle to prevent further injuries (Fig. 1). Ablation was performed using an irrigated RF catheter (Thermo-cool, Biosense Webster). Each session was done at 50 W for 30 s, with a force of 10-40 g/lesion. Ablation targeted the obstructive part of the septum to reduce the LVOT gradient. Initial LV hemodynamics revealed 125/20 mmHg, with an LVOT gradient of 100 mmHg preoperatively. The patient's final gradient was 76 mmHg at the end of the RF ablations. A surgical exploration needed to be done once the procedure finished due to persistent pericardial effusion. Surgical findings showed a right ventricular lesson, likely associated with the ICE catheter and not for the RF points since this procedure was done in a different localization than the perforation showed. No perforation of the LV was observed during the surgical revision.
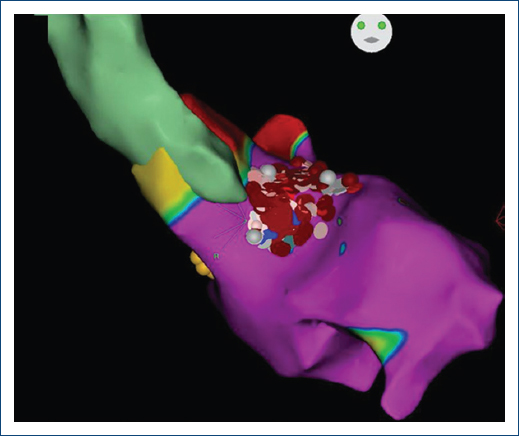
Figure 1 3D guided anatomical map of the left ventricle and radiofrequency ablation lesions (gray and red dots) His bundle in yellow dots. Anteroposterior view.
After the procedure, the patient continued standard medication. In 2022, TTE showed an EF of 71%, an LVOT gradient of 9 mmHg, and mild SAM; in 2023, EF was 60%, an LVOT gradient of 7 mmHg, without SAM, and a wall/septum thickness of 9/25 mm on TTE, which indicates that the benefit and effectiveness of the procedure improved months later independently of the septum size (Fig. 2).
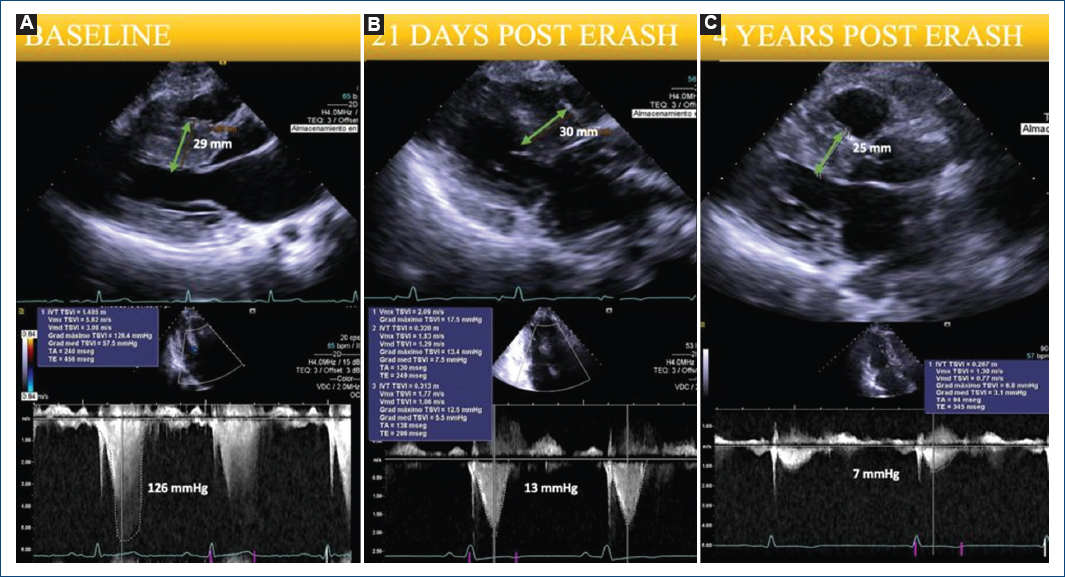
Figure 2 A: echocardiographic measurements of septal thickness and left ventricular outflow tract gradients performed under resting conditions before endocardial radiofrequency ablation of septal hypertrophy (ERASH) B: at 21 days of follow-up C: and 4 years post-ERASH.
HOCM has three invasive treatment methods: (a) Surgical septal myectomy (SM), (b) alcohol septal ablation (ASA), and (c) ERASH. SM is considered the gold standard for treating LVOT obstruction but may not be feasible in some countries, particularly Latin America, because it needs to be realized in specialized centers; otherwise, it can have a high mortality rate5. ASA, involving ethanol injection into the septal perforator artery, causes a basal septal myocardial infarction. However, ASA requires suitable septal arterial anatomy and has higher reoperation rates6.
ERASH, first reported by Lawrence T et al in 2011, emerged as an alternative treatment for HOCM6. RF ablation causes local hypokinesis (rather than reduced septal thickness), which reduces the LVOT gradient. Using a 3D electroanatomic mapping system (CARTO) has the advantage that the ablation is directed at the point of interest where the maximum obstruction is5,6. The patient was not a candidate for SM in this case due to our center's high mortality rate and lack of surgical experience. Furthermore, ASA was unsuitable due to her septal arterial anatomy, which did not provide an appropriate target for ethanol injection due to the absence of septal arteries. These factors justified the choice of ERASH, offering a less risky alternative.
Studies have shown significant symptom improvement and sustained LVOT gradient reduction at a 6-month follow-up with ERASH7. Our patient's LVOT gradient was substantially reduced from 126 mmHg pre-procedure to 7 mmHg at a 4-year follow-up, with a resolution of SAM and symptoms.
Conclusion
The ERASH procedure is an alternative to septal reduction therapies in HOCM patients. Prospective trials with extended follow-up periods must establish their safety and efficacy. The reduction in LVOT gradient and improvement in clinical symptoms in this patient highlights ERASH as a novel therapeutic option.

