











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Cardiomyopathies have historically been subject to confusion and descriptive-nominative controversy, mainly due to the difficulty in clearly and precisely distinguishing the etiological cause in many of them. This led to the inclusion, often inaccurately, of various entities exhibiting similar clinical and pathophysiological behaviors within their classification1-4. Today, we classify as cardiomyopathies those entities in which there is a structural and functional alteration of the myocardium, not explainable by the presence of coronary artery disease, valvular disease, or any form of abnormal volume or pressure overload5. In countries like Mexico, the significant incidence of these diseases necessitates strengthening the clinical knowledge of these entities to assess their social impact. They are capable of significantly limiting the quality and quantity of life for patients and, on the other hand, pose a substantial economic burden on healthcare, particularly in advanced stages of these diseases.
The Mexican Registry of Cardiomyopathies (REMEMI) is a program conceived by a group of Mexican cardiologists with the endorsement of the Mexican Society of Cardiology (SMC), driven by the need for clinical data on Mexican patients diagnosed with any type of cardiomyopathy. In our country, there is a lack of clinical, morphological, management, and prognostic data on cardiomyopathies. The primary objectives of the registry are: (a) to collect contemporary information on the clinical characteristics and management of these patients in Mexico, (b) to understand the demographics and incidence of the four most common forms of cardiomyopathies (hypertrophic cardiomyopathy [HCM], dilated cardiomyopathy [DCM], restrictive cardiomyopathy [RCM], and arrhythmogenic right ventricular cardiomyopathy [ARVC]), (c) to understand the most commonly used imaging and laboratory diagnostic methods for diagnosis and monitoring of these patients in Mexico, (d) to understand the therapeutic options used in these patients in our country, (e) to maintain a database that can be collected prospectively (active registry) to obtain information on clinical evolution, new diagnostic methods, or therapeutic procedures, as well as survival-related information for these patients, and (f) to compare the information obtained from our patients with that obtained in registries from other countries6-22. This knowledge allows us to conduct a detailed analysis of how to diagnose and treat patients with cardiomyopathy in Mexico and provide guidelines to enhance their care.
In this article, we are presenting the results of the first phase of REMEMI, where 1026 patients were included in the study, and the registration was completed by June 15, 2023. The integration of REMEMI-2 is currently underway, aiming to reach a total of 3000 patients and provide follow-up for the initially included patients.
Materials and methods
Design
The REMEMI was conceived as a multicenter observational registry of consecutive patients diagnosed with any form of cardiomyopathy in cardiology care centers in Mexico. Participating centers were invited to contribute the highest number of patients possible over a period of 3 years (initially planned for 1.5 years, but extended to double the time due to the COVID-19 health contingency). The study was presented and approved by the ethics and research committee of the Cardiological Hospital of Aguascalientes in accordance with local regulations. A consent form was provided to each patient included in the Registry system (http://www.rememi.mx/Inicia.aspx) before data collection. The registration system included demographic data of patients, which were divided into four groups according to the type of cardiomyopathy present. All clinical, laboratory, and imaging data, as well as the medications used with their doses and the therapeutic procedures implemented, were collected in the registration and data reporting format based on an electronic web system, where each researcher had their username and individualized password. The quality and accuracy of the data for each patient were reviewed and authenticated by an institutional committee, emphasizing data quality control, and statistical analysis was conducted by another auxiliary committee. The executive committee of REMEMI held regular meetings to analyze the progression of the number of included patients, as well as the quality and accuracy of the information, and the SMC participated as an endorsement for the invitation to participating centers.
Cardiomyopathy subgroups
It was decided to include patients with the four classifiable cardiomyopathies according to the European Society of Cardiology Guidelines23. Thus, patients with DCM, HCM, RCM, and ARVC were included. Patients with non-compacted left ventricle were included in the DCM group. Patients with genetic and/or acquired forms of each group were included in the study. The essential criteria for patient inclusion were: (a) patients over 18 years old, (b) authorization of informed consent, and (c) meeting clinical and diagnostic method criteria necessary to support the diagnosis of each type of cardiomyopathy.
Statistical analysis
Categorical variables are summarized by frequency and percentage. The distribution of numerical variables was analyzed using the Kolmogorov-Smirnov test. Numeric variables are summarized by mean and standard deviation or median and percentiles 25 and 75, depending on their distribution. Bivariate analysis was performed with the chi-square or Fisher’s exact test for categorical variables and Student’s t-test or MannWhitney U test for numerical variables. Variables with more than two options are analyzed with chi-square for linear trend or the Kruskal-Wallis test, as appropriate. Data are presented in tables and box-and-whisker plots. A two-tailed p < 0.05 is considered significant. IBM SPSS Statistics, version 25, was used for result calculations.
Results
A total of 1026 patients were included in the registry. All included patients were considered alive, with 54% of them having received medical attention within the last year. Seventy-two percent of the patients belonged to a national reference institution (National Institute of Cardiology). The distribution of patients by type of cardiomyopathy was 48% HCM, 48% DCM, 3.4% RCM, and 0.6% ARVC. Fifty-nine percent of the patients were male with a mean age of 57 ± 16 years. Demographic and baseline clinical data, along with their characteristics related to each type of cardiomyopathy, are presented in table 1 (ARVC excluded).
Table 1 Baseline characteristics by cardiomyopathy type
| Characteristics | MCH (n = 490) | MCD (n = 494) | MCR (n = 35) | p |
|---|---|---|---|---|
| Male, n (%) | 271 (55.3) | 310 (62.7) | 20 (57.1) | 0.058 |
| Age (years) | 59 (43, 71) | 59 (47, 71) | 64 (51, 71) | 0.27 |
| Diabetes mellitus, n (%) | 83 (16.9) | 6 (1.2) | 11 (31.4) | < 0.05 |
| Arterial hypertension, n (%) | 194 (39.5) | 104 (21) | 14 (40) | < 0.05 |
| Ischemic heart disease, n (%) | 30 (6.1) | 87 (17.6) | 5 (14.2) | < 0.05 |
| Smoking, n (%) | 135 (27.5) | 38 (7.6) | 10 (28.5) | < 0.05 |
| Alcoholism, n (%) | 96 (19.5) | 137 (27.7) | 7 (20) | 0.02 |
| Genetic study, n (%) | 21 (4.3) | 28 (5.6) | 1 (2.8) | 0.35 |
| Echocardiogram, n (%) | 407 (83) | 407 (82) | 32 (91) | 0.38 |
| Holter monitor, n (%) | 376 (76) | 260 (52) | 27 (77) | < 0.05 |
| Magnetic resonance imaging, n (%) | 294 (60) | 239 (48) | 22 (62) | < 0.05 |
| Exercise stress test, n (%) | 52 (10) | 29 (5) | 2 (5) | 0.02 |
| Syncope, n (%) | 64 (13) | 286 (57) | 6 (17) | < 0.05 |
| Functional class, n (%) | ||||
| NYHA I | 376 (76) | 391 (79) | 11 (31) | < 0.05 |
| NYHA II | 93 (19) | 29 (5) | 18 (51) | |
| NYHA III | 18 (3.7) | 8 (1.6) | 4 (11) | |
| NYHA IV | 2 (0.4) | 1 (0.2) | 2 (5.7) | |
| ACE inhibitor | 87 (17) | 13 (2.6) | 12 (34) | < 0.05 |
| Angiotensin II receptor antagonist | 102 (20) | 183 (37) | 4 (11) | < 0.05 |
| Beta-blocker | 344 (70) | 130 (26) | 22 (62) | < 0.05 |
| Sacubitril/valsartan | 27 (5.5) | 38 (7.6) | 14 (40) | < 0.05 |
| Direct anticoagulant | 61 (12) | 173 (35) | 15 (42) | < 0.05 |
| Vitamin K antagonist anticoagulant | 32 (6.5) | 108 (21) | 2 (5.7) | < 0.05 |
| Antiarrhythmic | 80 (16) | 55 (11) | 14 (40) | < 0.05 |
| Diuretics | 102 (20) | 170 (34) | 24 (68) | < 0.05 |
| Antiplatelets | 95 (19) | 329 (66) | 5 (14) | < 0.05 |
| Implantable cardioverter-defibrillator | 44 (9) | 130 (26) | 4 (11) | < 0.05 |
| Permanent pacemaker | 48 (9.8) | 26 (5.2) | 11 (31) | < 0.05 |
| Mitral insufficiency > mild | 75 (15) | 74 (15) | 9 (25) | 0.52 |
| Late gadolinium enhancement | 281 (95.6) | 210 (87.5) | 20 (90.9) | < 0.05 |
| LV ejection fraction | 65 (58, 70) | 47 (37, 57) | 54 (40, 60) | < 0.05 |
| Atrial fibrillation | 98 (20) | 146 (29) | 13 (37) | < 0.05 |
| Ventricular tachycardia | 37 (7.5) | 64 (13) | 6 (17) | < 0.05 |
HCM: hypertrophic cardiomyopathy; DCM: dilated cardiomyopathy; RCM: restrictive cardiomyopathy; NYHA: New York Heart Association; ACE: angiotensin-converting enzyme; LV: left ventricle.
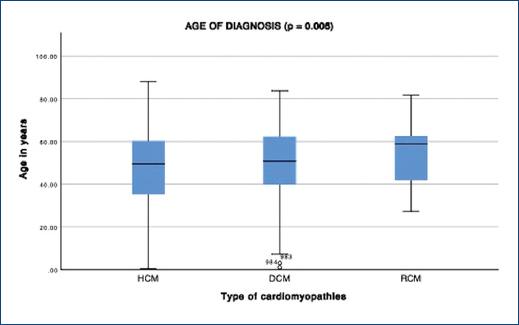
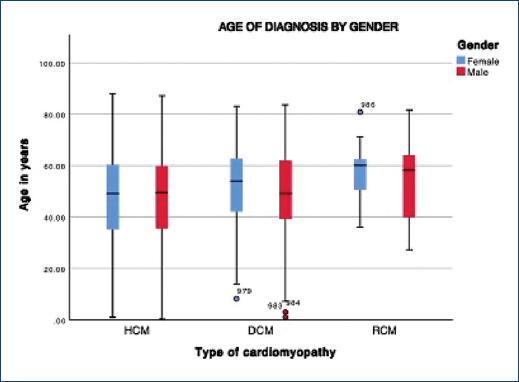
There are no significant differences in age at the time of inclusion in the database. However, differences in the age of diagnosis are evident, with a lower age in patients with HCM and a higher age in patients with RCM (Fig. 1). No differences in the age of diagnosis are observed between men and women in all three groups (Fig. 2).
The prevalence of risk factors is higher in patients with RCM, with hypertension being predominant. Syncope was more frequent in the DCM group, occurring in only 13% of patients with HCM. The RCM group exhibited a worse functional class. The majority of patients were in New York Heart Association (NYHA) class I.
Patients with ARVD are analyzed separately due to their low prevalence. They were predominantly male (85%) with an average age of 41 ± 9 years and had no coexisting risk factors. Three patients had received an implantable cardioverter-defibrillator (ICD).
Five diagnostic studies were considered most frequently. Transthoracic echocardiogram was performed in the majority of patients (82-91%), followed by Holter cardiac monitoring (52-77%). The latter was less frequently reported in patients with DCM (p < 0.05). Cardiac magnetic resonance (CMR) was mainly performed in the HCM and RCM groups (60% and 62%, respectively). Exercise stress testing and genetic testing were conducted in < 10% of patients. Other studies, such as endomyocardial biopsy and cardiac catheterization, were only performed in isolated cases (2 cases). Regarding the results, the presence of mitral insufficiency did not differ among the various types of cardiomyopathies. In patients who underwent CMR, nine out of 10 showed late gadolinium enhancement.
Regarding pharmacological treatments, a higher usage of Angiotensin-Converting Enzyme Inhibitors (ACE inhibitors) was observed in patients with RCM, and Angiotensin II Receptor Antagonists (ARB II) were more commonly used in HCM and DCM. Beta-blockers were frequently used in both HCM and RCM, with a lower prevalence in DCM (p < 0.05). The use of oral anticoagulants was more frequent in DCM and RCM, with a tendency to prefer direct anticoagulants. Diuretics were more commonly used in RCM, and antiplatelet agents in DCM.
The most frequent arrhythmia was atrial fibrillation (AF), observed in 20% of patients with HCM, 29% of DCM, and 37% of RCM (p < 0.05). Ventricular tachycardia (VT) was present in all patients with ARVD, 7% of HCM, 13% of DCM, and 17% of RCM (p < 0.05). The implantation of a defibrillator was more frequent in DCM (p < 0.05), and permanent pacemaker implantation was more common in RCM (p < 0.05). Table 2 presents the characteristics of patients with and without AF among those with HCM, DCM, and RCM. Only one patient with ARVD had AF. Significant differences were observed in age, history of syncope, NYHA functional class, degree of mitral insufficiency, right ventricular systolic function, and left atrial size. On performing multivariate analysis (Table 3), age, syncope, NYHA functional class > I, and left atrial size were identified as independent predictors of AF occurrence.
Table 2 Differences between the group with and without atrial fibrillation
| Characteristics | AF (n = 257) | No AF (n = 762) | p |
|---|---|---|---|
| Male gender, n (%) | 155 (60) | 446 (58) | 0.61 |
| Age (years) | 61 (51, 73) | 59 (44, 70) | < 0.05 |
| Diabetes mellitus, n (%) | 25 (9.9) | 75 (11) | 0.41 |
| Hypertension, n (%) | 78 (30) | 234 (36) | 0.08 |
| Ischemic heart disease, n (%) | 38 (14) | 84 (13) | 0.52 |
| Smoking, n (%) | 53 (20) | 130 (20) | 0.87 |
| Syncope, n (%) | 116 (46) | 240 (37) | 0.02 |
| Functional class, n (%) | |||
| NYHA I | 195 (76) | 583 (83) | < 0.05 |
| NYHA II | 44 (17) | 96 (13) | |
| NYHA III | 14 (5.5) | 16 (2.3) | |
| NYHA IV | 2 (0.8) | 3 (0.4) | |
| Moderate to severe mitral insufficiency | 65 (26) | 93 (15) | < 0.05 |
| Late gadolinium enhancement | 131 (95) | 380 (90) | 0.06 |
| LV ejection fraction | 58 (47, 68) | 62 (50, 68) | 0.44 |
| Ventricular tachycardia | 28 (10) | 78 (10) | 0.84 |
| TAPSE (mm) | 19 (16, 23) | 21 (19, 24) | < 0.05 |
| Left atrium size in millimeters | 49 (40, 61) | 40 (33, 49) | < 0.05 |
NYHA: New York Heart Association; LV: left ventricle; TAPSE: tricuspid annular plane systolic excursion; AF: atrial fibrillation.
Table 3 Logistic regression for atrial fibrillation prediction
| Variable | OR (IC 95%) | p |
|---|---|---|
| Age (years) | 1.05 (1.03-1.08) | < 0.05 |
| Syncope | 3.6 (1.2-10.4) | < 0.05 |
| NYHA class > 1 | 2.4 (1.16-5.09) | < 0.05 |
| Moderate to severe mitral insufficiency | 1.02 (0.39-2.6) | 0.95 |
| Left atrium size (mm) | 1.02 (1.00-1.04) | < 0.05 |
NYHA: New York Heart Association; OR: odds ratio; CI: confidence interval.
Discussion
We are presenting the First REMEMI, initiated in 2019 and, by April 2023, had already included 1026 patients with different phenotypes. The analysis of results shows, among other things, that the presentation of each subtype is entirely different. Furthermore, it allows us to understand the degree of adherence to the use of study methods and treatment regimens currently employed in our country.
DCM was the most frequently recorded in the study (494 patients), closely followed by HCM (490 patients), while RCM (35 patients) and ARVD (seven patients) had lower incidence rates. The differences among the four types of cardiomyopathies can be appreciated in table 1, indicating that the incidence of HCM is very similar to that of DCM in our population. Similar to other registries, RCM and ARVD are infrequent, though it is clear that the registry was not designed to calculate the prevalence of these entities in the general population.
The use of tools such as multinational registries is crucial for developing guidelines in the treatment and management of patients. It provides insights into demographic variables that can modify the impact of therapies for each studied population. Through these registries, the phenotype/genotype relationship has been elucidated for each region, as well as the impact and effect of medications on the studied groups6-22.
Due to the epidemic situation that occurred during the development of REMEMI, it was not possible to reach the majority of the projected patients. Nevertheless, the information contributed to the registry is significant, covering the entire breadth of the Mexican Republic and representing the first national massive registry of this pathology. The registry will continue for a couple more years with the intention of presenting REMEMI II.
Regarding demographic variables, similarities were observed compared to previous multinational studies. However, there was limited use of CMR, almost nonexistent use of genetic studies, and family counseling. This directly impacts the detection of new cases based on a proband. When comparing these results with those published in the global literature, it becomes evident that the study of patients in Mexico does not adhere to international guidelines for the study and management of these patients. This suggests the urgent need for the development of updated guidelines for their study and treatment in Mexico5,23.
Some invasive therapies, such as septal alcohol ablation (ASA), have a higher representation compared to other cohorts19. We have identified patients with asymmetric septal phenotype and a maximum LVOT gradient > 100 mmHg, in whom this type of therapy has not been projected. This suggests a failure in selecting patients who benefit from these methods. Only one patient underwent transaortic septal myectomy, indicating that this method has not been used as the first-line therapy for patients with significant refractory obstruction and important symptoms. This, of course, implies the lack of trained and qualified centers with a sufficient number of cases to ensure that the learning curve has been surpassed. In Mexico, ASA is more commonly used for managing obstruction in these patients.
Similarly, the use of ICD is relatively low, given its high costs and unavailability for the majority of patients, despite clear indications for its installation24,25.
The present study has the following limitations: (1) the observational nature of the study does not allow for drawing conclusions about prognosis or outcomes; (2) the patients do not present similar approaches due to the lack of standardization of diagnostic and therapeutic strategies; (3) although the study was designed with a multicenter character to achieve representativeness, this may be questionable due to the predominance of two centers; (4) although it is the largest number of subjects with these pathologies reported in Latin America, the number of subjects included is limited, which could affect its generalization.
In conclusion, REMEMI is the largest cardiomyopathy registry of Latin American. Understanding the epidemiology of these diseases through observational registries in Mexico is a valuable opportunity to understand the characteristics of the methods used in the study and treatment of diseases such as cardiomyopathies by Mexican physicians. It can provide information for the implementation of management guidelines and strategies to disseminate findings to improve healthcare in our country.
Participants
Special thanks to the doctors and their teams who participated in the inclusion of patients, representing the vital part for the development of national registries, from which this work emerges. Below, we list their names (doctors who participated with more than 15 patients in the registry are included as co-authors of the article):
Dr. Jorge Eduardo Cossio Aranda
Dr. Enrique Alexander Berrios Bárcenas
Dr. Rahab Amisadai Morales Flores
Dr. Sylvia Salmun Nehmad
Dr. Guillermo Antonio Llamas Esperón
Dr. Guillermo Llamas Delgado
Dra. María Cecilia Escalante Seyffert
Dr. Jorge Leal Cavazos
Dr. Eufracino Sandoval Rodríguez
Dr. Eduardo Pamplona Ávila
Dr. Enrique Sánchez Hiza
Dra. Liliana Estefanía Ramos Villalobos
Dra. Luisa Fernanda Aguilera Mora
Dr. Mario Alberto Benavides González
Dr. Carlos Daniel Carrillo
Dr. Norberto Matadamas Hernández
Dr. Aurelio Puentes Puentes
Dr. Rafael Pérez Abreu
Dra. Silvia Guadalupe Cerca
Dr. Julio Iván Farjat Ruiz
Dr. Luis Delgado Leal
Dr. Miguel Ángel Reyes Guzmán
Dr. José Juan Florencio Constancio Lozoya Morales
Dr. Manuel Odín de los Ríos Ibarra
Dr. German Ramon Bautista López
Dr. Sergio Joaquín Rangel Revilla
Dr. Víctor Abraham Navarro López
Dr. Yajaziel Azpeitia Hernández
Dra. Lilia Guadarrama Bustos
Dr. Luis Manuel Vargas Ramírez
Dra. María Isabel Sánchez Ramírez
Dr. Juan Ángel Peraza Zaldívar
Dra. Marianela Rodney Ortega
Dr. Santiago Sandoval Navarrete
Dr. Erick Dávila Zaragoza
Dr. Antonio Sánchez González
Dr. Humberto Azuara Forcelledo
Dr. José Luis Leiva Pons
In the same vein, we express our gratitude to the Research and Informatics Department of Hospital Cardiológica Aguascalientes for their support in conducting the study.
Conclusion
The REMEMI has allowed us to learn about some points of great importance in the way in which patients with various cardiomyopathies are studied and managed in Mexico. From this knowledge and its analysis we can conclude that there is still much to do in our country to strengthen education and on the other hand that it is necessary to develop management guides that offer the possibility of guiding the Mexican cardiologist in these pathologies.

