











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
The period between 10 and 19 years, referred to as adolescence, constitutes the transition from childhood to adulthood and entails a range of opportunities and challenges. The current generation of adolescents, the largest in history, comprises one sixth of the world population (Organización Mundial de la Salud [OMS], 2025). Students grapple with enormous complexities, ranging from climate change, poverty, and pandemics to unprecedented levels of armed conflict, technological development, and migratory movements (OMS, 2024a).
Adolescence is often marked by situations affecting life and health, with traffic injuries, interpersonal violence, and suicide representing the three principal causes of death during this period (OMS, 2024a).
According to the World Health Organization (WHO), deaths by suicide have diminished globally in recent years, falling from 762,000 in 2000 to 717,000 in 2021. In the Americas, however, their incidence has risen from 7.2 per 100,000 population in 2000 to 9.8 in 2021 (World Health Organization [WHO], 2024). Suicide in this region is the third leading cause of death for people aged 15 to 29 (OMS, 2024b).
According to the National Institute of Statistics, Geography and Informatics of Mexico (Spanish acronym INEGI), deaths from suicide have increased nationwide from 5.3 per 100,000 population (6,494) in 2017, to 6.3 (8,123) in 2022 and 6.8 in 2023 (Instituto Nacional de Estadística y Geografía [INEGI], 2023; 2024). In 2018 and 2021, suicide was the third leading cause of death within the groups aged 10-14 and 15-24 (INEGI, 2021).
Suicidal behavior (SB) represents a continuum encompassing ideation, planning, attempt, and actual suicide (Salvo & Melipillán, 2008), with attempted suicide being the main predictor of suicide (WHO, 2014). According to the 2022 National Health and Nutrition Survey, 7.6% of adolescents in Mexico have contemplated suicide at some point in their lives, with the prevalence of lifetime suicide attempts reaching 6.5%. Females report higher rates of suicidal ideation and attempts than males (Valdez-Santiago et al., 2023).
Given the challenges facing adolescents, the WHO has encouraged schools to adopt the life skills (LS) approach in their facilities, so that teachers can use this strategy with students in this age group (WHO, 2003). The Live Life Guide, published by the WHO in 2021, recommends incorporating LS with students as an evidence-based intervention for suicide prevention. A key feature of this approach is that it provides a positive perspective on mental health rather than focusing on suicide (Organización Panamericana de la Salud, 2021).
Within this framework, LS are defined as “…abilities for adaptive and positive behavior that enable individuals to deal effectively with the demands and challenges of everyday life” (WHO, 2003, 2020). These skills fall into social, cognitive and emotion-control categories, which in turn are subdivided into 10 groups: self-awareness, effective communication, decision-making, creative thinking, managing feelings and emotions, interpersonal relationships, empathy, problem-solving and conflict resolution, critical thinking, and stress management (Mangrulkar et al., 2001). Systematic reviews of this issue suggest that implementing the LS approach in schools enhances the mental health of the adolescent population (Fenwick-Smith et al., 2018; Singla et al., 2020). Although efforts have been made to promote LS in school contexts, there is a dearth of published studies in Mexico. Research on LS has not focused on suicide prevention (SP) (López et al., 2022; Morales Rodríguez et al., 2013), but rather on other topics such as addiction prevention (Fuentes et al., 2023; Mojarro, 2020). Only one LS study on SB was identified, conducted on 26 students at a high school (González-Cruz, et al., 2023).
This article analyzes the specific LS and degree of familiarity with SB middle-school adolescents in three Mexican states had acquired prior to the implementation of a suicide prevention initiative.
METHOD
Study design
This study is part of a larger project entitled Educational Interventions for Preventing Suicidal Behavior among Adolescents in Mexico. The study using mixed methods was conducted between 2022 and 2024. Three interventions for the prevention of SB were implemented and evaluated with middle school adolescents in urban settings. The qualitative component of this research included pre-intervention FGs with teachers and students.
This article analyzes the FGs conducted with students who subsequently participated in the educational interventions designed to enhance their life skills.
The methodology of these FGs, described below, is based on the three dimensions of the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Tong et al., 2007).
Research and reflexivity team
The authors formed part of a larger multidisciplinary research team. Four women and one man with experience in qualitative methodology and conducting FGs participated in the analytical phase: two psychologists (one with experience in clinical psychological clinical), a doctor, a nurse, and an anthropologist. Three held doctorates and two master’s degrees in health systems, medical anthropology, and public health and they were all aged between 30 and 65.
Given the topic of our research, we adopted a phenomenological perspective, with content analysis (Gibbs, 2012).
Participants
Participants were selected by convenience, or non-randomly, using the inclusion criteria of the broader project mentioned above. Selection was performed sequentially: first the participating states, then the schools, and finally the students. Five states were selected for the broader project: Baja California Sur, Campeche, State of Mexico, Querétaro, and Morelos. They were selected by convenience, seeking collaboration with health authorities committed to participating in all the project activities for three years. The only inclusion criterion was signing a collaboration agreement.
Three public middle schools fulfilling the following inclusion criteria were subsequently selected in each of these states: 1) being located in urban areas, 2) having the required infrastructure for the project activities.
Finally, participants, including adolescents, were selected. The study was presented to the school authorities, who, in turn, explained the objective of the study and its activities, including the FGs, to the parents. Parental consent and informed consent from the adolescents were obtained from those who agreed to participate. For the FGs, those who had participated in the activities prior to the FGs and were in the groups that would participate in the educational interventions were selected.
The FGs were held at the school facilities and scheduled in June 2023 as suggested by the academic authorities to facilitate student attendance. Since it was decided that one FG would be conducted per school, the theoretical saturation criterion was not followed. Six FGs were held in three states: one in Baja California Sur, two in Campeche, and three in Morelos. Two research team members traveled to each state for this purpose. A total of 53 students from public middle schools participated, 28 in second grade and 25 in third grade. Twenty-four of the students were female and 29 male, with an age range of 12 to 15 years, and an average age of 14.
Procedure
Prior to conducting the FGs, we screened the selected schools to determine the prevalence of SB. During this initial contact, students were informed about the study. Throughout the research process, the team assumed an ethical position toward students in the FGs and the school authorities. We prioritized delivering reports to the state authorities as the basis for formulating public policies.
A question guide was prepared for data collection, emphasizing LS in relation to SB in adolescent students.To this end, the research team held meetings to delimit the sections by topic of interest and design the questions. Team members selected to conduct the FG workshops participated in this task to ensure that everyone fully understood the guide during data collection. Although pilot tests were not conducted, the first FG fulfilled that purpose. The research team subsequently adapted the guide based on students’ understanding and reactions to the questions. The FG guide included three LS-focused sections exploring perceptions and experiences regarding decision-making, negotiation, and emotion management. Another section focused on identifying knowledge of SB and attention seeking, while the final section addressed reflections on the importance of developing LS for adolescents.
Only the selected students and two research team members were present at each FG. One researcher moderated the session while the other took notes. All the FGs, lasting approximately 30 to 90 minutes, were audio-recorded. Audios were transcribed verbatim using a word processor and confidentiality was always maintained. Transcripts were not shown to the students for comments and/or corrections.
Analysis
The research team audio-recorded the FGs, transcribing them verbatim into a word processor. They then read the transcripts and performed qualitative content analysis.
The research team drafted a codebook based on the revised question guide, defining three central phenomena of interest: students’ LS, SB, and perceptions of the LS workshops as reference for future initiatives. Five analytical categories emerged from these variables: (1) decision-making, (2) problem-solving and conflict resolution (negotiation), (3) managing emotions, (4) knowledge of SB, and (5) perceptions of the LS workshops. The resulting 30 codes served to conduct an initial deductive analysis of the data obtained.
Atlas Ti version 9 was used in the analysis because of its suitability for information management (Cisneros, 2002). We began by reading each transcript and segmenting the text according to the pre-established codes. We then reread the codes to differentiate their contents and ensure compliance with the concepts in the codebook. We subsequently identified units of meaning in each segment and, by constantly comparing the codes, established our initial findings regarding the relationship between selected LS and students’ knowledge of SB.
We read each transcript again using inductive analysis.New fragments of the students’ discourse (“open codes”) emerged, revealing two new categories of experience related to suicide and distrust.
Although we did not corroborate the findings with the students, we recorded the characteristics of their interaction during the FGs.
Ethical considerations
This study was part of a larger project entitled Educational Interventions for the Prevention of Suicidal Behavior among Students in Mexico, approved by the Research Ethics Committee of the National Institute of Public Health (CI:1742, Folio I07). The FGs described in this article were conducted after we had obtained informed assent from the participating students and informed consent from their parents or guardians.
RESULTS
The main findings are given below, organized by the analytical axes of our work. First, the status of participants is described with respect to the development of each LS explored: decision-making, problem-solving and conflict resolution (negotiation) and managing emotions. Students’ knowledge of SB is then addressed, followed by an examination of the categories that emerged from their discourse with respect to experiences concerning suicide and lack of trust in their teachers and caregivers. Finally, we present our findings on participant perceptions and suggestions regarding the workshops. The testimonials from the FGs are shown in tables as an analytical-narrative resource summarizing the fragments of discourse exemplifying the content of the categories and brief testimonials are given in one of the sections.
Decision-making
Students reported that adults made most decisions for them at school and in their families. At school, these decisions largely involved the discipline exercised by teachers. They also concerned matters students felt they should be responsible for deciding themselves. Decisions they were allowed to make mainly concerned dichotomous choices regarding everyday actions yielding immediate perceived benefits (Table 1).
Table 1 Characterization of life skills among adolescents participating in focus groups
| Analytical axes | Sample quote |
|---|---|
| Decision-making | |
|
Decision-making
contexts |
Interv: Ok. And at school, do adults also decide for you? I-F: Yes, about coming to school. Interv: Coming to school. What else? Your teachers, the prefects, the directors? I-M: How we should dress. Interv: How you have to dress? I-M: How we have to cut our hair. I-F: Or where we have to sit, sometimes. (GF-CAM-04) I-F: Unfortunately, not me. They say, “Either you wear these clothes, or you don’t go out, you stay home.” So, in other words, if I say an outfit, unfortunately my mom tells me yes, well, yes, that she doesn’t want me to wear those clothes. Sometimes she gets upset with me and starts saying, “Oh, you’re going to wear this again?” or something like that, and then she grabs my clothes, and I put them on. (GF-CAM-02) |
|
Dichotomous
decisions |
I-F: Like, for example, hm, what to do: go and train, yes, yes or no, like in any type of problem that I may have, I always choose something that makes me feel good, that doesn’t make me feel uncomfortable in a problem or another kind of thing. (GF-CAM-04) Interv: Well, yes, they’re decisions. And what other decisions do they make? I-M: Whether to get up. (GF-BCS-02) |
| Problem-Solving and Conflict Resolution (negotiation) | |
| As a bribe |
Interv: How would you define what negotiating is? I-F: It’s like, well, I had a kind of confusion with my sister who said, “If you don’t buy this for me, I’m going to tell my [our] parents.” Interv: And did you buy it for her? I-F: Well, yes, I had to buy it for her, but she told my parents anyway. (GF-MOR-05) |
|
Offering some-
thing in return |
I-F:Once, I negotiated with a friend. I didn’t do my homework, and I had to, for example, give him some bills for doing my homework... (GF-MOR-03) I-M: Well, it’s when I want to go out, yes, go out. Then, hm, I start doing things around the house. I wash the car, and I’ve already done this type of negotiation... (GF-BCS-02) |
| Managing emotions | |
|
Emotions accord-
ing to context |
I-F: No, at school, mostly, I feel good because here I can be myself. At home, sometimes, if I see something I like, some- times, if my mom tells me not to do it because that’s supposed to be bad, and the truth is, yes, a little more. (GF-BCS-02) I-F: For example, here at school, I feel, like, I don’t know, very happy, or things like that, or sometimes discouraged because I don’t want to come. (GF-MOR-03) I-F: For me, well, when it comes to school, when it comes to school, my emotions get nervous, anxious and calm, and a little happy. (GF-MOR-03) |
|
Difficulty naming
emotions |
Interv: What emotions do you think you often feel? I-M: Hm, happiness and anger Interv: Another other emotion? I-M: Sadness I-M: Is despair an emotion? (GF-MOR-06) I-M: Well, yes, that “I don’t care” thing happens when you’re angry or sad or think about a situation that’s happened to you and you say that you don’t care anymore or that it’s already in the past. But I feel that’s only to let go of how bad you feel that moment or what you experienced, and the best thing is to forget it or do new things to let go, let go of all that past. (GF- CAM-02) |
Note:Interv: Interviewer; I-M: Intervention-male; I-F: Intervention-female; FG-CAM: Focus Group-Campeche; FG-BCS: Focus Group-Baja California Sur; FG-MOR: Focus Group–Morelos.
Participating students were beginning to improve their decision-making skills, since adults made most of the latter in their school and family settings. Respondents did not feel that they or others, apart from teachers and primary caregivers, could make decisions in the community.
Problem-solving and conflict resolution (negotiation)
The experiences reported by students suggest that they begin to develop this skill within the family. There, they learn and experience an asymmetric form of negotiation in which permissions and pardons were requested from parents and favors were asked of siblings in return for performing activities or giving them something. At school, they learn to solve problems and resolve conflicts through making requests of their classmates, often offering money in exchange, which shapes their negotiating style.
Notably, students equated the term “negotiation” with giving bribes, or buying or selling items. “I-M: I once negotiated with a friend. I hadn’t done my homework and I had to do it and now I have to pay him for example a few bills for doing my homework,” FG-MOR-03. Participants from all three states regarded negotiating as an activity in which they were obliged to offer something in exchange for what they needed or wanted. “I-M: Maybe I want something and I’ll tell them that if they buy it off me, I’ll do something to help, or something like that” FG-MOR-05 (Table 1).
Managing emotions
The family was the context with the greatest density and diversity of emotions. However, there was a link between family and school environments, in that emotions that occurred in one were channeled towards the other and vice versa.
The most frequently reported emotions in the family setting were anger and frustration, related to family dynamics within the family and the nature of the interaction between adults and youths. Other crucial factors included the socioeconomic status of the students, often linked to alcoholism and/or domestic violence.
A conversational pattern observed during the sessions enabled us to identify a behavioral mechanism called “emotional regulation,” which included a series of behaviors students engaged in to help manage their emotions. Figure 1 shows the specific emotions reported and related attempts at emotional regulation, illustrating the coping strategies students used to manage them. Figure 1 shows the emotion that triggers the most mechanisms and the type of emotion.The left column shows the emotions identified in the adolescents while the right one shows the main mechanisms for emotional regulation.
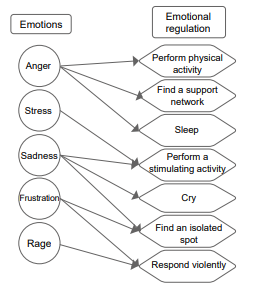
Figure 1 Frequent emotions and emotional regulation among adolescents participating in focus groups.
Emotional regulation was not described as a single event, but rather as a series of consecutive actions. For example, some participants reported that they or a classmate had experienced an emotion such as sadness and had attempted to achieve emotional regulation by going to a secluded place and then crying or engaging in self-inflicted violence. This may have indicated a lack of skills for containing emotions, which would have prevented self-harm. Participants also identified positive emotions such as happiness but did not elaborate on how they had experienced these feelings.
When we examined emotional regulation, it was clear that this process was undertaken individually. Among the range of mechanisms available to students for managing emotions, talking about their feelings with others was not usually their first choice. Another finding was related to the difficulty participants experienced in naming their emotions, either because they could not identify them or because they attempted to find words that conveyed indifference (Table 1).
Knowledge and experiences of suicidal behavior
The meanings of SB varied among students from different states. For example, in Baja California Sur and Morelos, SB was conceived of as a thought, something that suddenly appeared and lodged in the mind, whereas in Campeche, it was considered a way out, something that “happened,” providing a solution (Table 2).
Table 2 Knowledge and experiences of suicidal behavior among adolescents participating in focus groups
| Analytical axes | Sample quote |
|---|---|
| SB as a thought |
I-M: They come up, like thinking about taking your life. (GF-BCS-02) I-F: …and he’s going to start saying that, in his mind he’s going to say, “Well, no one loves me, everyone’s going to hate me. It would be better for me to die so they really see how I feel…” (GF-MOR-03) |
| SB as a “way out” |
I-M: It’s like looking for a way out. They say something like that to other people to solve what they, what they have. It’s a lot like “Oh, it’s just that if I continue in this, if I continue here, I’m no good for anything anymore, nobody cares about me.” Something like that. (GF-CAM-04) I-F: Like, I could tell him [or her] to look for help. It’s like, because, like, they say they all believe that committing suicide is a way out of the problem, but it’s not. (GF-CAM-04) |
|
Experiences
related to suicide |
Interv: Have you had a close experience of someone taking their own life or attempting to do so? I-M: I lost an uncle who committed suicide. (GF-BCS-02) I-F: I tried four times, but no. Interv: You tried it? How did you do it? I-F: Huh? Interv: How did you do it? I-F: Oh, it was several ways, but I never dared because I was afraid of dying. I was afraid of dying, that it would hurt. Interv: So you planned it, but you didn’t go through with it, you stayed there? I-F: Like, I already had the time, the date, everything. I had everything planned, but I didn’t end up doing it because I started to think and said, “It’s going to hurt, no, I’d better not.” (GF-BCS-02) I-F: …in fact, they found me lying there. They took me to the hospital, they treated me. Since I didn’t know about that, I didn’t get to cut my veins. I didn’t cut myself here, I just cut myself here, too. Since I heal quickly, well, you can’t see it any more, you can’t tell, but I always called my parents to get me out of the center because I didn’t want to be there. (GF- CAM-02) |
Note:Interv: Interviewer; I-M: Intervention-male; I-F: Intervention-female; FG-CAM: Focus Group-Campeche; FG-BCS: Focus Group-Baja California Sur; FG-MOR: Focus Group-Morelos; SB: Suicidal behavior.
Students from Campeche did not mention suicidal ideation. They only thought of SB at the time it took place, conceptualizing it as “a way out.” This perception was a recurrent pattern in the six FGs. Students constructed their concept of suicide through their experiences in both family and school contexts. At school, this was sometimes due to knowing a classmate who had said they wanted to take their own life or engaged in self-harm practices. At home, some participants had a close relative who had taken their own life, or had even attempted suicide themselves (Table 2).
However, students generally regarded themselves as being skilled at identifying risk situations related to SB among their peers. These included a classmate declaring that no one understood them, saying that they did not feel like doing anything or that they perceived everything negatively. This skill was mentioned by students in six GFs. However, only those in Campeche and Morelos expressed a willingness to talk, question or give advice to their classmates regarding their behavior. They even mentioned their willingness to provide support if their classmate so required.
In Morelos, students also declared that they would be willing to help their friends and classmates seek professional care outside school by identifying specialized mental health-care venues they themselves had attended (Table 3).
Table 3 Experiences associated with care for suicidal behavior among the adolescents participating in focus groups
| Analytical axes | Sample quote |
|---|---|
|
Willingness to
support a school- mate |
I-F: So when you feel bad, call me or whatever, tell me. To accompany the person because the person, more than anything, that person has to come out of it herself [or himself]. Nobody can… (MOR-06) I-F: Tell him [or her] that that person, well yes, it does help to lift people’s spirits, or that that person is important, or tell him [or her] encouraging things like that. (GF-CAM-04) I-F: …better still, I would approach him and talk to him and ask him what’s happening to him, and try, try to help him, encourage him, always be with him and always try to accompany him all the time to see that nothing bad happens to him. (GF-MOR-03) I-F: Well, when a person feels like killing himself, it’s better to stay there all the time with him and never leave him alone because, by [not] being attentive, you would leave him in a deep state of depression, and he’ll start to say that, in his mind, he’ll say, “Well, no one loves me, everyone’s going to hate me. It would be better for me to die so they really see how I feel.” It’s better for me to stay with that person to help him.” (GF-MOR-03) |
|
Seeking profes-
sional assistance outside the school environ- ment |
I-M: Me, for example, about my friend, I would try to find a psychologist or my psychologist that I have, to tell him what’s happening to my friend, and that I can tell him, I don't know if I can tell him a little to help me help my friend with what’s happening to him. (GF-MOR-3) Interv: And, let’s say, do you identify an institution in addition to a person? We already know that you go to the hospital when you feel bad. I-F: CAISA Interv: What’s CAISA? I-F: Oh, I don’t remember exactly, but I go there. It’s like a help center for adolescents. (GF- MOR-06) |
|
Teacher-student
bond of trust |
Interv: Here at school, can you identify any teacher that you generally trust? I-M: Yes. I-F: Yes. I-F: Yes. Interv: Who is it? I-M: A teacher [called] L. I-F: A teacher [called] A. I-F: Teacher L. and teacher A. Interv: What subjects do they teach? I-F: Chemistry and Spanish. (GF-MOR-05) Interv: Do you think students would go to them and ask for help? I-F: I think it depends on their problem, you know. I-F: It depends on their problems, and the emotions or problems they have. (GF- MOR-03) |
| Distrust |
I-M: I keep it to myself. Interv: You keep it to yourself, where? I-M: Sometimes I feel strange, but I don’t talk about it. (GF-BCS-02) I-F: Besides, my emotions are because of problems, so, and when I talk about them, it’s very difficult for me because I feel that person can judge me or say something. (GF-CAM-04) I-F: I say that [In my opinion,] asking for help to tell someone, having someone I can talk to about my luck, because, mostly, I keep all my problems to myself, I don’t have anyone I trust to tell something like that to. I don’t know if, if I would need someone to count on. (GF-CAM-04) I-F: I don’t know, the psychologist seems cool to me. I-M: More than anything because of lack of trust. I-F: Because of the trust that can come through… I-F: And because of everything you’re telling her, you don’t know if she tells parents or something like that. She could tell one of your classmates and your parents or someone else, and there you’ll feel that all the information that you gave her, she’s going to know that everything… (GF- MOR-03) |
Note: Interv: Interviewer; I-M: Intervention-male; I-F: Intervention-female; FG-CAM: Focus Group-Campeche; FG-BCS: Focus Group-Baja California Sur; FG-MOR: Focus Group-Morelos; SB: Suicidal behavior; CAISA: Comprehensive Care Center for Adolescent Health.
In Campeche, students did not mention spaces either inside or outside the school environment, where they could ask for help if a classmate displayed SB. However, they did mention certain school figures whom they felt they could approach to talk about SB, such as the school principal and group tutor. They also said that they felt confident talking about SB with certain teachers. This teacher-student bond of trust was also present in Morelos, in specific contexts, even with teachers from areas other than psychology (Table 3). These dynamics of trust between teacher and students were not reported in Baja California Sur.
When asked whether they would feel comfortable approaching the school psychologist, if one were available, students in Morelos replied that this would depend on the degree of trust they had established with them.
Students’ distrust emerged as a category in all six FGs. It was reflected in their limited attempts to seek spaces or situations where they could talk to educational figures or their primary caregivers about their emotions, personal concerns, and SB. Although they admitted that they would like to have a trusting environment at school where they could discuss their experiences and seek help, they were afraid that the information they provided would be shared with their caregivers or that they might be judged for what they expressed (Table 3).
Perceptions and suggestions from students regarding the LS workshops
Students remarked that they had never previously had a space where they could talk about SB or social skills. In their opinion, having these skills would have practical repercussions in their everyday lives including their relationship with their parents and helping their classmates. They also made suggestions about the way they would like to receive information, and what kind of activities, dynamics or games they enjoyed although they added that games could create distractions.
Finally, the participants suggested topics, such as trust and communication with parents, which could be incorporated into the workshops. They highlighted the need to address the establishment of stronger bonds of trust between peers, since communicating with the latter gave them a sense of release (Table 4).
Table 4 Life skill workshops: perceptions and suggestions from adolescents participating in focus groups
| Analytical axes | Sample uote |
|---|---|
| Importance |
I-F: The truth is I do want to have that skill of knowing how to communicate especially with my mother because sometimes I’m afraid of what she’ll think because, yes, there are times when she tells me that “Oh, it’s normal that you feel that way,” so then it’s a little frustrating. (GF-CAM-02) Interv: Do you think that these types of topics help us in our lives in some way? I-M: Yes. Interv: Like in what? I-M: Like in knowing how to act in these situations. I-F: And also, to help people in a situation. Interv: Like in what situation? I-F: Like in knowing if someone is stressed, knowing how they react. (GF-MOR-06) |
| Topic suggestions |
Interv: Like what kind of topics would you like to be discussed in these workshops? I-F: Hmmm, I don’t know, trusting parents. Interv: Another topic? I-F: Understanding parents. I-F: Communicating with your parents. (GF-MOR-05) Interv: What do you think can be done to improve these types of things? I-F: That a person, some person, someone makes my parents understand that maybe I want to talk with them and tell them something and that they understand me and that they listen to me, that they understand me. (GF-CAM-04) |
|
Strengthen the
bond with peers |
I-M: That’s right. Why? Because he feels confident to say “Ah, he’s someone my age, I’m going to joke with him, I’m going to have a talk, and later we're going to talk about what interests me.” That’s what I mean: a guy [that says] “Ah, it’s another guy,” blah blah blah, and in between jokes, the truth appears. That’s what I mean. I think that right now you don’t listen to an adult, you listen to a person you trust [in]. I think that’s what happens. (GF-CAM-02) I-F: I think it would be to sit down [it’s a matter of sitting down] with the person you trust most and, between the two of us, tell each other your problems to let off steam. It could be like that. (GF-MOR-05) |
Note: Interv: Interviewer; I-M: Intervention-male; I-F: Intervention-female; FG-CAM: Focus Group-Campeche; FG-BCS: Focus Group-Baja California Sur; FG-MOR: Focus Group-Morelos.
DISCUSSION AND CONCLUSION
The main contribution of this research is that it presents and interprets the Life Skills (LS) experiences of adolescent students in relation to suicidal behavior (SB). This information will serve as a reference for the forthcoming implementation of an educational initiative based on the LS approach. The results revealed that the students had only marginally developed the skills explored, highlighting the urgent need to implement LS interventions at schools.
Evidence suggests that student mental health improves as a result of educational interventions based on the LS approach in school settings (Fenwick-Smith et al., 2018; Pannebakker et al., 2019; Singla et al., 2020).
Encouraging results have been reported from several educational interventions promoting LS not only to improve mental health, but also to prevent SB (González-Cruz, et al., 2023; Jegannathan et al., 2014; Yen et al., 2023). Moreover, LaFromboise & Lewis (2008) obtained positive results when implementing the LS approach considering the sociocultural context[s] of adolescents belonging to specific ethnic groups.
The results of this research show that decision-making is usually mediated by adults, with students only being able to make decisions about immediate, everyday situations.This differs from other studies, which have found that adolescent decision-making is influenced by their interaction with others, particularly with friends or peers (Be et al., 2021). As regards problem-solving and conflict resolution, we found that negotiations between adolescents and adults tend to be asymmetrical, with adults usually having the upper hand.
The most frequently reported emotions were negative, such as anger, sadness, and frustration. The range of emotional regulation patterns was limited, with adolescents often isolating themselves, crying, or responding violently.For Di Giunta et al. (2022), these patterns occur in young people who feel neglected at home or whose parents insist their children do exactly as they are told. These patterns lead adolescents to believe they are incapable of dealing with their emotions, representing an area of opportunity for interventions that provide emotional management tools.
Importantly, we found that students consistently reported a lack of spaces in which to talk about their emotions or personal problems and were reluctant to discuss them at school for fear that they might be judged or that their parents could find out. These findings are consistent with the experiences of this age group in another study (Díaz-Alzate & Mejía-Zapata, 2016).
In the context of suicide prevention, LS have a protective effect as they have been associated with increased life satisfaction and healthy family functioning including effective communication (Ram et al., 2020). Regarding knowledge about SB, adolescents generally perceive themselves as skilled at identifying peers at risk of SB.
Efforts to implement the LS approach with adolescents at school must consider involving the entire school community in the process, including parents/caregivers and everyone else who comes into direct contact with the students. It has been reported that adolescents who live with their parents or have a parent with high educational attainment score better in problem-solving and conflict resolution (negotiation), self-esteem, creative thinking, and coping with stress than those who do not (Buch et al., 2021). Likewise, school environments have been found to be spaces of opportunity for working with the adolescent population and contributing to the development and implementation of LS to enhance their mental health. Moreover, operating in the school setting helps reduce barriers often encountered by students and their families, such as travel time and costs, preventing the stigma that commonly emerges when seeking mental health services in the community (Xu et al., 2020). Active participation by teachers and administrative staff in LS efforts is therefore also recommended.
The results obtained in the focus groups highlighted the differences between students at the participating schools. Subsequent studies must endeavor to achieve a deeper understanding of the contexts where adolescents develop. Research has found that factors beyond the individual can influence the development of LS and must be considered to develop relevant initiatives (Díaz-Alzate & Mejía-Zapata, 2016). A recent study of adolescent students observed differences between rural and urban contexts regarding the status of LS development, while the socioeconomic status and sex of participants also exerted an influence (Contini et al., 2013).
It is worth noting that the meaning students from Campeche attributed to SB as a “way out” (solution) rather than a way of thinking differed from that of students from Morelos and Baja California Sur. This divergence can be explained through the socio-cultural context with a profound Maya influence in the Yucatan peninsula, where suicide can be seen as a way out of everyday problems (Hernández, 2010).
Determining students’ degree of LS prior to conducting educational interventions provides valuable information for designing these initiatives. It also makes it possible to incorporate the specific socioeconomic conditions and cultural contexts of students, and their families and schools.
The patterns of emotional regulation commonly displayed by adolescents require intervention programs to enhance their skills for containing emotions and preventing self-harm. They also require information strategies to enable them to conceptualize SB accurately. However, it is essential to take steps to raise awareness of this issue among parents as well.
One limitation of this study was the lack of contact with students prior to the FGs, which limited the establishment of trust between the research team and participants. This restricted the amount of information obtained from certain FGs.

