











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
The WHO life skills (LS) model focuses on health protection and the prevention of risky behavior (Darlington-Bernard et al., 2023). LS are positive, adaptive psychosocial and interpersonal abilities enabling adolescents to make assertive decisions, solve problems, develop critical thinking, communicate effectively, and manage their lives in a healthy way to cope with everyday events (United Nations Children’s Fund [UNICEF], 2000; World Health Organization [WHO], 2021). This approach considers: 1) the importance of cognitive, interpersonal, and coping skills in psychosocial development; 2) the role of these skills in protecting health, adopting positive behaviors, and fostering healthy social relationships; 3) the reinforcement of protective factors to prevent risky behavior (Darlington-Bernard et al., 2023; WHO, 2020); 4) the strengthening of protective factors, such as self-knowledge, self-confidence, and self-esteem; 5) the improvement of academic performance (Rai & Vandana, 2022); and 6) the mastery and application of these skills to enhance self-efficacy and promote well-being during adolescence (Ross et al., 2020; WHO, 2003, 2020).
Life Skills Training (LST) is a universal, school-based preventive approach for adolescent students to cope with risk behaviors. With its multiple components, it has generated ten skills sets to support the training method (Alfaro et al., 2010; Mangrulkar et al., 2001; WHO, 2003, 2020). This approach was developed in the United States in 1979 and has since spread throughout the world (Botvin & Griffin, 2007; Botvin et al., 2015; Espada et al., 2015; Velasco et al., 2015).
Since certain risk behaviors and mental health problems have their onset during childhood and adolescence, it is essential to strengthen LS through community interventions, psychoeducation campaigns, and curricular content to impact mental health problems. Interpersonal skills, assertiveness, and problem-solving are active components consistently associated with the effectiveness of interventions. These LS contribute to achieving positive mental health and preventing undesirable outcomes (Skeen et al., 2019).
Despite the evidence supporting the effectiveness of LS-based interventions in areas such as drug use reduction, with significant improvements in process and outcome evaluation, tools for its measurement remain limited. A systematic review of longitudinal evaluation studies on the effectiveness of LS programs found that most focus on adolescents and have limited evidence on the effectiveness of specific program components. Additionally, most studies are developed in Western societies, particularly the United States and Europe, limiting the generalizability of their findings to other cultural contexts (Kirchhoff & Keller, 2021). However, evidence indicates the positive long-term effects of LST on adolescent drug use, attributed to improvements in resistance to peer pressure and assertiveness (Weichold & Blumenthal, 2016). Another systematic review of drug use prevention programs for children and adolescents has reported positive results for LST in several domains, suggesting that there is evidence to support its effectiveness. The results of ten studies using this approach revealed a reduction in drug use, together with improvements in people skills, self-esteem, assertiveness, coping, and anxiety reduction. It is important to note, however, that the quality of the studies varied due to the methodological approaches used for their evaluation (Tremblay et al., 2020).
The WHO has adopted the LST approach for health promotion in schools (Alfaro et al., 2010; Botvin & Griffin, 2005, 2007; Mantilla & Chahín, 2012; Organización Panamericana de la Salud [OPS], 2001; Velasco et al., 2015; WHO, 1993, 2003, 2020). Data show that LST is effective in dealing with drug use. Nonetheless, conceptualizations, longitudinal studies, and standardized, validated instruments are still required to evaluate interventions, compare the impact of LST-based programs, and develop best practices (Duerden et al., 2012; Faggiano et al., 2014; Hoskins & Liu, 2019; Tremblay et al., 2020;UNICEF, 2020).
The LS work model has been implemented in various intervention strategies across Latin America. An analysis of the literature shows that Mexico has published the most articles (six), followed by Chile, Colombia, and Costa Rica with two each, and Ecuador, Peru, and Spain with one each (Solís, 2022). There is, however, a need to improve the methodological quality of interventions in the region (Santana-Campas et al., 2021) as well as the measurement instruments used (Solís, 2022). The development of reliable, valid instruments to measure SL in Latin America has recently seen significant growth, with various questionnaires demonstrating acceptable psychometric values (Cronbach’s alpha .63-.90) (Alfaro et al., 2010; Díaz-Posada et al., 2013; Fernández & Castro, 2020; Niño-Bautista et al., 2017; Pérez de la Barrera, 2012Pérez de la Barrera, 2012; Reyes & González, 2020; Santana-Campas et al., 2018; Santana-Campas et al., 2024). Three of these studies provide the reliability index for the global scale (Fernández & Castro, 2020; Reyes & González, 2020; Santana-Campas et al., 2018). Four studies have assessed the ten skills of the WHO model (Díaz-Posada et al., 2013; Fernández & Castro, 2020; Reyes & González, 2020; Santana-Campas et al., 2018); three have undergone an EFA (Alfaro et al., 2010; Fernández & Castro, 2020; Santana-Campas et al., 2018) and one a CFA (Santana-Campas et al., 2018). Most of the questionnaires are long, with the number of items ranging from 70 (Pérez de la Barrera, 2012Pérez de la Barrera, 2012Pérez de la Barrera, 2012) to 80 (Díaz-Posada et al., 2013; Fernández and Castro, 2020; Reyes & González, 2020; Santana-Campas et al., 2018). This can make respondents lose interest and find the questionnaire tedious. Although Alfaro et al. (2010) and Niño-Bautista et al. (2017) have analyzed questionnaires with 36 to 37 items, they do not report reliability values. One of the brief questionnaires includes the ten LS in the WHO model (Santana-Campas et al., 2024). The original version has 80 items (Santana-Campas et al., 2018), reduced to 40 in the brief version.
However, it reports internal structure values, CFA data, invariance analysis, and reliability coefficients (with Cronbach’s alpha, ordinal alpha, and McDonald’s omega equal to or greater than .90). However, the authors recommend exercising caution when using this brief test, as four of the dimensions failed to meet the reliability criteria (empathy, effective, assertive communication, interpersonal relations and problem solving and conflict resolution).
There are a limited number of psychometrically acceptable LS scales (Hoskins & Liu, 2019; UNICEF, 2020). Some are too extensive (Díaz-Posada, 2013), and require special training (Haug et al., 2021), meaning that it is necessary to develop brief, robust, cost-effective scales to test specific interventions for drug use prevention in the Mexican context where drug use is a critical issue in adolescents.
LS education in developing countries tends to produce short-term results. There is usually no systematic implementation, follow-up, or long-term evaluation (Nasheeda et al., 2018), or they lack standardized, culturally appropriate instruments (Kirchhoff & Keller, 2021; Nasheeda et al., 2018).
Appropriate tools are therefore required to measure LS effectiveness and evaluate their potential (Ross et al., 2020).
The limited number of instruments for measuring LS underscores the need to develop brief, valid, reliable, and culturally appropriate tools to use in prevention programs (Hoskins & Liu, 2019; UNICEF, 2020). These instruments could also serve as screening tools to identify problematic areas in adolescents, obtain evidence to support strategies for their psychosocial development, and evaluate the effectiveness of interventions.
The aim of this study is to measure construct validity through the implementation of the exploratory and confirmatory factor analysis of the EHV-A, designed according to the WHO LS model for health protection and the prevention of risk behaviors (Darlington-Bernard et al., 2023; WHO, 2003). We also seek to prove the reliability and concurrent validity of the scale in Mexican adolescents. Concurrent validity was estimated through the relationships between Life Skills (LS) and Self-esteem (SE). The following hypotheses were proposed : 1) The psychometric properties of the EHV-A scale are adjusted to a sample of Mexican adolescents. 2) LS and Self-esteem constructs, measured through the EHV-A instrument and the Rosenberg Scale (RSE) have statistically significant relationships.
METHOD
Study Design and Participants
We conducted a quasi-experimental pre-post and follow-up study comparing groups that received preventive intervention and control groups, using non-probabilistic convenience sampling. The study evaluated LS and other variables. The sample included Mexican male and female junior and senior high school students and was divided into an experimental group and a control group. Once we had obtained the final sample, we randomly assigned whole school groups to either the experimental or the control group. A random sample was drawn from each group (n = 500) to avoid the sample size problem in confirmatory factor analysis (CFA). Exploratory factor analysis (EFA) was performed with the control group sample and CFA was performed with the experimental group sample, which included participants living in different states. The evaluation was conducted from 2017 to 2019.
Measures
The Brief Life Skills Scale for Adolescents (EHV-A) was designed using items from other more extensive scales with 6 to 36 items each assessing skills separately, which have been validated for Mexican adolescents (Alfaro et al., 2010; Betancourt et al., 2018; Betancourt et al., 2019; Pérez de la Barrera, 2012; Sánchez-Xicoténcatl et al., 2013). The items included in the EHV-A had the highest factor loadings and the original 4-point Likert scale was maintained for each item. The responses for the 24 items in the EHV-A are 1 = never, 2 = rarely, 3 = often, and 4 = always.
The skills include planning for the future, assertiveness, expression of emotions, taking responsibility, decision making and resistance to peer pressure. We included these six specific LS in the EHV-A because they have proven to be effective in preventing drug use and maintaining emotional wellbeing in adolescents (Alfaro et al., 2010; Andrade Palos et al., 2009; Betancourt et al., 2018; Betancourt et al., 2019; Pérez de la Barrera, 2012; Sánchez-Xicoténcatl et al., 2013; UNICEF, 2020).
Conceptual Definitions of LS Included
Planning for the future involves the ability to set goals linked to the results one wishes to achieve (Alfaro et al., 2010; Pérez de la Barrera, 2012). Assertiveness is the ability to express feelings, thoughts, or desires and to communicate them in an open, respectful manner (Alfaro et al., 2010; Pérez de la Barrera, 2012). Expression of emotions consists of the ability to recognize one’s emotions and express them (Alfaro et al., 2010; Pérez de la Barrera, 2012).
Taking responsibility is the ability to make conscientious choices based on the positive and negative consequences of a behavior before acting (Betancourt et al., 2019). Decision making is the ability to evaluate an action and its possible consequences to make a responsible decision (Betancourt et al., 2019). Resistance to peer pressure is the ability to refuse to use alcohol, tobacco, or other drugs even if friends insist (Aguilar-Kubli, 1987; Sánchez-Xicoténcatl et al., 2013).
A brief version of the Rosenberg Self-Esteem Scale (RSE) (Rosenberg, 1965) was included to evaluate concurrent validity of the EHV-A. Data on improving self-esteem using LST make it an acceptable parameter for testing the external validity of LS measurements (UNICEF, 2020). The original scale comprises ten items, and we used the five positive statements with equivalent meanings across several cultures (Benish-Weisman et al., 2020). These items are grouped into a single factor with internal consistency values above .75, with the following Likert responses: 0 = strongly disagree, 1 = disagree, 2 = agree, and 3 = strongly agree. The higher the score, the higher the respondent’s self-esteem (Jiménez et al., 2007).
Procedure
Prior to initiating the data collection process, briefing meetings were arranged with school authorities and parents from the respective educational institutions. The objectives and activities to be conducted were thoroughly explained. The authorities approved the presence of the research team at the schools. Parents were advised that they would receive an informed consent form with all the information on the study and that their children would receive an assent form, and would make the final decision to participate. A team of trainee psychologists was taught to supervise the self-administered paper and pencil questionnaires. Average response time was 50 minutes, with a 100% response rate.
Data Analysis
Data analysis was performed with the SPSS 26 and IBM SPSS Amos 26 packages (IBM Corp., 2019). The internal structure of the scale was analyzed using two techniques. The first was an exploratory factor analysis (EFA) with oblique rotation to estimate the internal consistency of the subscales and the entire scale. This is the most widely used analysis for developing and validating scales because it explores a set of latent variables explaining the responses to the items. EFA assumes that the measures reflect the underlying constructs (Bollen & Lennox, 1991; Edwards, 2011; Edwards, 2011; Kim & Mueller, 1978) and that part of the variability of an item will be produced by communality.
The second technique was confirmatory factor analysis (CFA). This analysis seeks to determine whether the number of factors obtained in EFA, and their loadings correspond to what is theorized about the data. The initial hypothesis is that there are several factors, each of which is associated with a certain number of variables. CFA yields a confidence level to determine the hypothesis. In this analysis, we consider the following most common fit indicators. CMIN is the minimum discrepancy value (X2), p > .05, which is the probability of a large discrepancy with the current sample, CMIN/df, which should have a value of close to 1 for models that fit adequately, although an index close to .5 or less has been suggested as a reasonable value (Wheaton et al., 1977). Comparative fit index (CFI) is the probability of a large discrepancy with the current sample (Tanaka, 1993), which also ranges between 0 and 1, with .9 being the minimum required to defend the model (Bentler & Bonett, 1980). The normed fit index (NFI) measures the decrease in the chi-square statistic of the model adopted with respect to the base model, whose minimum value is .9. The root mean square error of approximation (RMSEA) is used to measure the model error, with values of between .05 and .08 indicating an acceptable fit (Browne & Cudeck, 1993).
The scale was constructed with the assumption of the existence of six factors: planning for the future, assertiveness, expression of emotions, resistance to peer pressure, decision making, and taking responsibility. In the analyses, membership for each factor was defined as a loading ≥ .30. Reliability was estimated by calculating Cronbach’s alpha, where the desired value was > .70. Concurrent validity was estimated using RSE as a parameter, the expected values for strong effects being > .50. EFA was performed with principal axis extraction, oblique rotation, and Kaiser normalization. Two approaches were used in this analysis, one in which the eigenvalue was greater than one and another in which the solution was adjusted to six factors.
Ethical considerations
The Research Ethics Committee of the Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz (Approval No. CEI/C/003/2016) approved the study. The objectives of the research, and the risks and benefits of participating in the study were explained to students. They were informed that their participation was voluntary, that their answers would be anonymous, and that the results would not affect their activities or grades. All the participants’ parents signed an informed consent form, and all the participants provided written informed assent, as required by Mexican law (Diario Oficial de la Federación, 2014). Due to the confidentiality agreement established with the participants, the data used in the current research (database, questionnaires, informed consent and assent) are not available in a public repository. All the procedures adopted the ethical standards of the committee responsible for institutional human experimentation and the Declaration of Helsinki 2000. Informed consent was obtained from all the participants in the study.
RESULTS
The sample included 3,787 Mexican junior (60%) and senior high school students (40%) and balanced in terms of sex (49% were female and 51% male). The age range was 11 to 19 years (M = 14, SD = 1.7). School groups were randomly assigned to the experimental (n = 2397) and control groups (n = 1390).
EFA and CFA in the Solution Adjusted to Six Factors.
The six-factor model explained 76% of total variance, obtaining a global eigenvalue of 18.232. The variance explained by each factor ranged from 3% to 52%, while eigenvalues ranged from .72 to 12.47. The factor structure (Table 1) was as follows: 1) planning for the future (three items); 2) resistance to peer pressure (six items); 3) decision making (six items); 4) expression of emotions (three items); 5) assertiveness (three items); and 6) taking responsibility (three items).
Table 1 Exploratory Factor Analysis and Internal Consistency Measures for the Brief Life Skills Scale for Adolescents (EHV-A) (Six-Factor Structure)
| Factor/items |
Factor
loadings |
M(SD) | Asymmetry | Kurtosis |
Item-total
correlation |
Cronbach’s
alpha |
|---|---|---|---|---|---|---|
| 1. Planning for the future | .916 | |||||
| I try to achieve the goals I set for myself. | .551 | 2.41(1.170) | .155 | -1.451 | .858 | .858 |
| I strive to achieve what I really want. | .536 | 2.31(1.209) | .251 | -1.503 | .83 | .88 |
| I have defined goals in life. | .45 | 2.35(1.218) | .205 | -1.537 | .806 | .90 |
| 2. Resistance to peer pressure | .919 | |||||
| I refuse to drink alcohol at parties or gatherings with my friends when I don’t want to. |
-.882 | 2.40(1.274) | .104 | -1.67 | .768 | .904 |
| I tell my friends not to insist when they push me to drink alcohol. |
-.871 | 2.30(1.273) | .274 | -1.613 | .809 | .899 |
| I would say no if my best friend asked me to get drunk and I didn’t want to. |
-.853 | 2.31(1.301) | .24 | -1.678 | .814 | .898 |
| I would drink soda at a party even if most people were drinking alcohol. |
-.752 | 2.32(1.275) | .229 | -1.637 | .826 | .896 |
| I can refuse a drink when I don’t want one. | -.629 | 2.27(1.347) | .302 | -1.725 | .828 | .896 |
| I wouldn’t drink if I didn’t want to even if my friends were drinking alcohol. |
-.341 | 2.34(1.321) | .219 | -1.716 | .579 | .93 |
| 3. Decision making | .893 | |||||
| I think about the possible consequences before deciding | .859 | 2.33(1.057) | .192 | -1.185 | .791 | .863 |
| I look for as much information as possible to decide. | .773 | 2.37(1.037) | .13 | -1.149 | .711 | .875 |
| I think carefully about what I am going to do when I must decide. |
.72 | 2.34(1.115) | .176 | -1.332 | .739 | .871 |
| I think about different ways to solve a problem. | .621 | 2.32(1.077) | .213 | -1.229 | .755 | .868 |
| I think about the advantages and disadvantages of my decisions. |
.61 | 2.35(1.048) | .164 | -1.17 | .751 | .869 |
| When I decide I evaluate the results. | .381 | 2.55(1.022) | -.028 | -1.121 | .544 | .9 |
| 4. Expression of emotions | .841 | |||||
| I express what I feel. | .791 | 2.36(1.08) | .177 | -1.241 | .694 | .791 |
| I am a person who shows affection. | .77 | 2.41(1.061) | .16 | -1.192 | .733 | .756 |
| I show my happiness. | .563 | 2.33(1.231) | .22 | -1.559 | .7 | .792 |
| 5. Assertiveness | .853 | |||||
| I can express my ideas clearly and openly. | .698 | 2.43(1.036) | .083 | -1.149 | .731 | .788 |
| I give my point of view, even if it is different from that of other people. |
.604 | 2.41(1.08) | .102 | -1.259 | .729 | .789 |
| I defend my opinions to my friends. | .453 | 2.34(1.122) | .186 | -1.345 | .712 | .806 |
| 6. Taking responsibility | .824 | |||||
| I arrive at appointments on time. | .742 | 2.42(1.048) | .096 | -1.178 | .647 | .789 |
| I arrive at classes on time. | .619 | 2.35(1.179) | .217 | -1.45 | .731 | .706 |
| I fulfill my commitments. | .379 | 2.43(1.038) | .13 | -1.142 | .67 | .769 |
Note: M(SD): Mean (standard deviation)
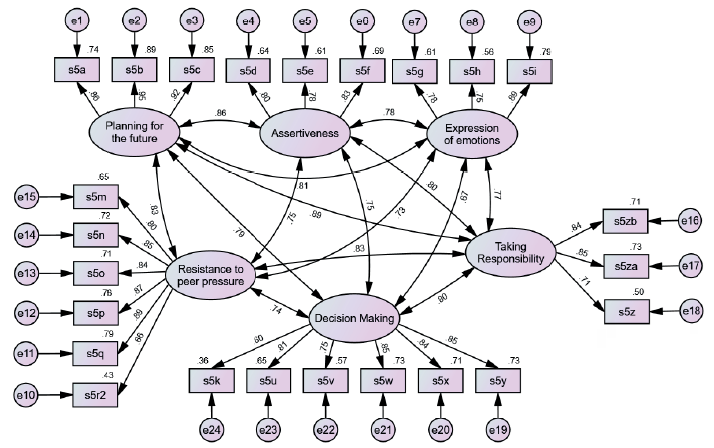
The six-component factor structure yielded by EFA was corroborated by CFA. The CFA model showed good fit indices (X2 = 697.27, p < .001; CFI = .963; NFI = .952; RMSEA = .055; AIC = 787.99) (Figure 1).
Reliability and Concurrent Validity
Table 2 shows the reliability data calculated in EFA, which were excellent for each factor (with Cronbach’s alpha ranging from .82 to .92), and for the entire scale (Cronbach’s alpha = .96). The item-total correlations of the variables in the model were also satisfactory (.54-.86). The concurrent validity of each factor was calculated with RSE and the correlations were acceptable and theoretically consistent. The fit indices for each of the models were adequate.
Table 2 Factor Correlations with Rosenberg Self-Esteem Scale
| CMIN (X 2 ) | p | NFI | F0 (CI) | RMSEA | PCLOSE | r | |
|---|---|---|---|---|---|---|---|
| Six-factor | 613.991 | < .001 | .942 | .720 (.594 - .877) | .055 | .048 | |
| Future | 106.884 | < .001 | .961 | .170 (.114 - .240) | .094 | .000 | .66 |
| Assertiveness | 117.173 | < .001 | .943 | .190 (.131 - .263) | .100 | .000 | .72 |
| Emotions | 98.477 | < .001 | .952 | .153 (.101 - .221) | .090 | .000 | .68 |
| Peer pressure | 174.933 | < .001 | .953 | .255 (.183 - .341) | .077 | .000 | .64 |
| Decision making | 153.553 | < .001 | .954 | .213 (.148 - .294) | .070 | .003 | .66 |
| Responsibility | 94.104 | < .001 | .954 | .145 (.094 - .211) | .087 | .000 | .67 |
Note: CMIN: Minimum Discrepancy Value; NFI: Normed Fit Index; RMSEA: Root Mean Square Error of Approximation; F0: Minimum Discrepancy Function; PCLOSE: p-value associated with RMSEA hypothesis testing
DISCUSSION AND CONCLUSION
The results of this study indicate that the questionnaire demonstrates enhanced psychometric properties and convergent validity in the six-factor solution. These findings align with our objectives to validate the EHV-A scale according to the WHO LS model approach. Moreover, the study examined the associations between the LS and RSE constructs in Mexican adolescents, demonstrating the potential of the questionnaire to serve as a useful tool for assessing LS in this demographic. Since adolescents are prone to mental health challenges, it is essential to have tools to identify limitations in their abilities to interact in a range of contexts. To develop this scale, we used items that were comprehensible, culturally relevant, and psychometrically sound, drawing on other assessments. Using measurement instruments should be easy, acceptable to participants, sensitive, valid, and reliable (Román et al., 2016; Warner, 2004). Their use is therefore more feasible in spaces where the timely identification of skills can lead to the development of programs to strengthen LS. School settings are suitable for the use of these tools, as they offer an ideal context for screening, prevention, and intervention due to the ease of access to large samples in a more controlled environment (WHO, 2020).
In accordance with the initial hypothesis, the psychometric properties of the EHV-A scale, developed according to the WHO approach (2003), have been validated as adequate for Mexican adolescents. The EHV-A scale demonstrates validity at the structural level. The EHV-A scale has two major advantages over other scales developed using the WHO approach (Kennedy et al., 2014; Kobayashi et al., 2013): First, it aligns with the focus proposed by the WHO in terms of health protection and the prevention of risk behaviors. Second, its brief structure with just 24 items makes it particularly well-suited for implementation in fieldwork settings. As mentioned earlier, the creation of this scale could help address the lack of reliable, valid instruments for the Spanish-speaking context. Most available scales are extremely lengthy and designed for English-speaking contexts (Kirchhoff & Keller, 2021). The creation of culturally appropriate instruments allows for the collection of robust, relevant data for drug use prevention based on the strengthening of LS such as resistance to peer pressure, assertiveness, and decision-making (Weichold & Blumenthal, 2016).
The LST approach has proved effective in changing adolescents’ relationship with drugs and strengthening personal skills and self-esteem (Tremblay et al., 2020).
Regarding the second hypothesis, the results confirm a statistically significant relationship between the LS and SE constructs. Structural Equation Modelling (SEM) reveals a close relationship between LS and SE. This finding underlines the close association between adolescent individuals’ perception of their self-esteem and their cognitive, emotional, and social life skills. These findings are consistent with prior scientific knowledge. This outcome also validates the external validity of the EHV-A scale as a brief yet effective instrument in educational settings.
Confirmatory Factor Analysis
Analysis of the internal structure through CFA showed a good fit of the hypothesized six-factor model for the EHV-A: planning for the future, assertiveness, expression of emotions, resistance to peer pressure, decision making, and taking responsibility. These results concur with those reported by the original authors of the scales (Betancourt et al., 2019; Jiménez et al., 2007; Pérez de la Barrera, 2012; Sánchez-Xicoténcatl et al., 2013). The six-factor structure supports the use of a total score representing the cumulative score of LS, as well as the individual score of each skill. The estimation of reliability through internal consistency for the six LS produced satisfactory Cronbach’s coefficients, ranging from .84 to .92. These values also concur with the values for the original versions. Item analysis showed item-total correlations above .60 for most of the items, which is acceptable.
Reliability and Concurrent Validity
The concurrent validity of each life skill with the RSE was highly satisfactory, with correlation coefficients of between .6 and .7. The five items in this brief self-esteem scale constituted a single factor, comprising the sum of the scores, and also had acceptable internal consistency (Cronbach’s alpha > .75).
Our findings indicate that the EHV-A demonstrates excellent reliability and strong concurrent validity and is theoretically congruent with a brief version of the RSE. EFA produced a robust model explaining nearly 70% of the variance, and the six factors comprising it are theoretically congruent with respect to each life skill assessed. CFA corroborated the model, which obtained adequate fit indices.
The EHV-A assesses six skills (planning for the future, assertiveness, expression of emotions, resistance to peer pressure, decision making, and taking responsibility) and includes a brief RSE in a self-administered format. It is therefore a valid, reliable scale, and a cost-effective tool with considerable potential usefulness for monitoring LS and self-esteem in adolescent populations. It is also a potentially useful tool for evaluating interventions designed to improve and develop these skills in groups of adolescents at school. EHV-A makes it possible to generate baseline estimates of each of the six LS and self-esteem in the adolescent population to design evidence-based interventions that will enhance these skills. This scale is a suitable option in comparison with other available options in terms of length and psychometric quality (Solís, 2022). Although there are others with good performance and acceptable quality (Alfaro et al., 2010; Díaz-Posada et al., 2013; Fernández & Castro, 2020; Niño-Bautista et al., 2017; Pérez de la Barrera, 2012; Reyes & González, 2020; Santana-Campas et al., 2018; Santana-Campas et al., 2024), its brevity makes it more practical (Fernández & Castro, 2020; Reyes & González, 2020), and its reliability scores are higher than those in other short versions (Santana-Campas et al., 2024). The use of the EHV-A before and after interventions would also help to measure their impact in strengthening LS and self-esteem.
There is evidence that self-esteem is a protective factor influencing physical and mental health, as well as social behavior, cushioning the impact of the negative influences or risks associated with adolescent development. It is therefore important to consider the potential of self-esteem in promoting mental health (Mann et al., 2004; Moulier et al., 2019).
There are also studies supporting the notion that self-esteem plays an essential role in individual adaptation to the environment, with implications for emotional health and mental well-being during adolescence. These findings highlight the importance of interventions that contribute to self-esteem during this stage of the life cycle (Moksnes & Espnes, 2012; Moulier et al., 2019; Zangirolami et al., 2018).
The development of LS in adolescence promotes mental well-being, good interpersonal relationships, and healthy behaviors. It also increases self-esteem and may constitute a protective factor against risk behaviors. Studies of prevention and intervention programs based on skills training in adolescence have shown that LS promotion has a positive impact on self-esteem as a psychosocial factor contributing to adolescents’ mental health, and a healthy lifestyle (Jafarigiv & Peyman, 2019; Mann et al., 2004; Moulier et al., 2019; Niaraki & Rahimi, 2013; Tremblay et al., 2020; Zangirolami et al., 2018).
The excellent scores obtained here in validating the EHV-A with junior and senior high school students, and the potential of schools to serve as spaces for mental health promotion mean that it is important to conduct studies with children and preadolescents (Moulier et al., 2019; Zangirolami et al., 2018).
The EHV-A has understandable, culturally meaningful, and psychometrically robust items from other tests. It is recommended for use in adolescents up to 17 years of age, and it can be used for fundamental decision making in mental health promotion. This validation provides health, social, and educational professionals and researchers with a cost-effective scale to assess key LS and develop psychological resources. The EHV-A can be used to estimate baselines and evaluate interventions to promote LS and self-esteem in the adolescent student population. We believe that the findings of this study provide evidence that the EHV-A is suitable for use in further research on the functionality and effectiveness of LS-based intervention programs (Nasheeda et al., 2018).

