











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
Permalink
INTRODUCTION
In 2021, approximately 1.1 billion deaths were reported worldwide, of which nearly 100,000 (8%) were due to cancer. In Mexico, cancer is the third leading cause of death. In addition, cancer mortality increased from 6.09 per ten thousand population in 2010 to 7.06 in 2021 (National Institute of Statistics, Geography and Informatics; Spanish acronym INEGI, 2023).
Although the incidence of cancer cases has risen in recent years, survivorship has also risen due to early detection and medical advances. There are currently over 16.9 million survivors in the United States, as opposed to just three million in 1971 (American Society of Clinical Oncology [ASCO], 2021). A survivor is defined as a patient who had a cancer diagnosis and is currently in remission. Some of the literature describes survivorship from the moment of diagnosis without specifying the stage of the patient (American Cancer Society [ACS], 2021). Three survivorship phases are described: the acute phase, from diagnosis until completion of initial treatment, the extended phase. after initial treatment and in the subsequent months, and permanent survivorship, when years have passed after treatment. However, survivorship vaies depending on the type of cancer. Those with the highest survival rates are breast cancer, prostate cancer, and colorectal cancer (ASCO, 2021).
Receiving a cancer diagnosis can trigger emotional responses with a direct impact on people’s lives, causing discomfort in the biopsychosocial-spiritual spheres. However, even when there is a diagnosis indicating that patients are free of disease, it has been observed that the psycho-emotional consequences do not disappear quickly. They often persist over time, negatively impacting the quality of life of patients who experienced it. At least 50% of survivors suffer physical and emotional consequences after completion of their treatment (Martínez Arroyo et al., 2019).
Instruments measuring the needs of surviving patients in various oncological populations include the following: The Spanish Questionnaire to Detect Unmet Needs of Cancer Survivors (CESC), comprising 25 items with three factors, physical, emotional and financial/work-related. It has a Cronbach’s Alpha of .77 for the first, .71 for the second and .63 for the third component (Arrighi et al., 2014).
The Fear of Cancer Recurrence Inventory, developed by Sébastien Simard and Josée Savard, was designed to evaluate the fear of cancer recurrence in a multidimensional way. It consists of 42 items with seven dimensions: triggers, severity, distress, coping, functional alterations, perception and detection behaviors. It has a Cronbach’s Alpha of .95 (Simard & Savard, 2009).
The Supportive Care Needs Survey has two versions, a long and a short one. The long one has 59 items, the short one 34 and both cover five domains: psychological, health system, physical and daily activities, patient care and support, and sexuality. It has internal consistency, measured with Cronbach’s Alpha, greater than .85 in all subscales (Boyes et al., 2012).
The Cancer Survivors’ Unmet Needs (CaSUN) measure scale is the original version. It consists of 35 items measuring the needs of surviving patients, six items concerning positive changes that have arisen as a result of the disease (41 items in total), and an open question about experienced needs. It has five domains: existential survival, comprehensive care, information, quality of life and interpersonal relationships. The questionnaire shows internal consistency, with a Cronbach’s Alpha value of .96. Three hundred and fifty-three surviving patients participated in the creation of the questionnaire (Hodgkinson et al., 2007). It has been adapted for the oncology population of several countries, described in Table 1.
Table 1 Different versions of CaSUN
| Version | Number of items | Factors | Cronbach’s alpha |
|---|---|---|---|
| CaSUN (original) (Hodgkinson et al., 2007) |
42 | Exploratory Factor Analysis yielded five factors: existential survival, quality of life, relationships, comprehensive care, information. |
.96 |
| CaSun-S (Spanish population) (Martínez et al., 2021) |
35 | Confirmatory Factor Analysis: 5-factor model the same as the original showed adequate goodness-of-fit properties. |
.95 |
| T-CaSUN (Thai cholangiocarcino- ma population) (Summart et al., 2022) |
20 | Four factors: Intensive care, information, relationships, and medical care. Exploratory factor analysis was performed on one half of the sample and confirmatory factor analysis on the other. |
.79 |
| CaSUN-NL (Keeman et al., 2018) |
37 | Exploratory Factor Analysis yielded a total of seven factors. Five original ones: Existential survival, comprehensive onco logical care, information, quality of life, personal relationships Two domains were added: lifestyle and return to work. |
.94 |
| Slovenian population (CaSUN-SL) (Miroševič et al., 2022) |
40 items and one open question |
Exploratory factor analysis was performed on one half of the sample and confirmatory factor analysis on the other. The quality-of-life factor was replaced by an emotional and psychological support one. |
.94 |
| Chinese population (CaSun-C) (Fang et al., 2018) |
20 items | Exploratory factor analysis was performed on one half of the sample and confirmatory factor analysis on the other. Four factors: physical/psychological needs, information, med- ical care and communication needs. |
.87 |
| Japanese population (Casun-J) (Komatsu et al., 2020) |
41 items and one open |
Confirmatory factor analysis: Five factors, including existen- tial survival, comprehensive cancer care, information, quality of life and relationships. |
.96 |
Since the questionnaire has not been validated for use in the Mexican population, the objective of this study is to obtain the validity and reliability of the instrument so that it can be used in this population.
METHOD
Study design
The type of research conducted was an observational, prospective, cross-sectional, descriptive study with a non-experimental quantitative research design.
Participants
The sample size was determined by the proportion of the number of items presented in the questionnaire, with five responses for each item (Vallejo, 2011). An initial sample of 294 participants was obtained, of which 114 were ruled out for failing to meet the inclusion criteria. The eligible population comprised a total of 180 cancer survivors, who had received care at hospitals and institutions in both the public and private sector, and members of support groups for cancer survivors. The inclusion criteria were being of either sex, with a minimum age of 18, having Mexican nationality, having received a cancer diagnosis, being in the follow-up phase (survivorship) from the extended phase onwards, and participating, with a signed informed consent form. The exclusion criterion was having difficulty understanding the questionnaire. The elimination criterion was withdrawing their informed consent. The average age was 55.5 years (SD = 11.85). One hundred and fifty-seven participants were women (87.2%), 80 participants had completed a bachelor’s degree (44.4%), the majority of the participants were married (60.6%) and the most frequent types of cancer were breast (56.7%), head and neck (7.2%), gastric (6.7%), gynecological (6.1%) and hematological cancer (6.1%). The average length of time since diagnosis was 51.63 months (SD = 50), and the average length of time since end of treatment was 30.86 (SD = 45.47). In regard to length of survivorship, 60 participants had survived for fewer than six months (33.5%), 90 had survived for between 6.1 and 60 months (50.3%) and 24 had survived for over 60.1 months (13.4). Table 2 shows the sociodemographic data of the eligible population.
Table 2 Sociodemographic data, related to cancer and survival
| Variable | n | % |
|---|---|---|
| Age (X̅ = 55.50; SD = 11.85) | ||
| Time since diagnosis (X̅ = 51.63; SD = 50) | ||
| Time since end of treatment (X̅ = 30.86; SD = 45.47) | ||
| Survivorship ≤ 6 months | 60 | 33.5 |
| Survivorship ≤ 6 months | 90 | 50.3 |
| Survivorship ≥ 60.1 | 24 | 13.4 |
| Sex (n = 180) | ||
| Woman | 157 | 87.2 |
| Man | 23 | 12.8 |
| Education (n = 179) | ||
| Elementary school | 3 | 1.7 |
| Junior high school | 13 | 7.2 |
| Senior high school | 17 | 9.4 |
| Technical degree | 35 | 19.4 |
| Degree | 80 | 44.4 |
| Postgraduate degree | 31 | 17.2 |
| Marital status (n = 180) | ||
| Married | 109 | 60.6 |
| Single | 31 | 17.2 |
| Divorced | 25 | 13.9 |
| Living together | 9 | 5.0 |
| Widowed | 6 | 3.3 |
| Cancer diagnosis (n = 180) | ||
| Breast | 102 | 56.7 |
| Head and neck | 13 | 7.2 |
| Lung | 5 | 2.8 |
| Gastric | 12 | 6.7 |
| Gynecological | 11 | 6.1 |
| Hematological | 11 | 6.1 |
| Kidney | 4 | 2.2 |
| Thyroid | 8 | 4.4 |
| Prostate | 7 | 3.9 |
| Testicular | 2 | 1.1 |
| Other | 5 | 2.8 |
Procedure
Questionnaires were administered at centers, hospitals, and institutions and among support groups. An electronic version of the questionnaire was designed using Google Forms so that they could be shared by the participating centers. The study was explained to the oncologists and doctors responsible for monitoring patients. During the follow-up consultations, they invited patients to participate, by signing the informed consent form (included in the same form) and answering the questionnaire. A text message was sent to cancer survivors registered with the participating centers. They were invited to participate and if they agreed, the study was explained to them, and they subsequently signed the informed consent form and filled out the questionnaires.
The type of sampling used was non-probabilistic, with chain case study assignment. In other words, key participants were identified and asked to tell other participants with similar characteristics about the questionnaire (Hernández-Sampieri et al., 2014).
Instruments
The Spanish version of the Cancer Survivors’ Unmet Needs (CaSUN-S) measure, validated for the Spanish population through its administration to 566 breast cancer survivors, was used as a basis. Five factors were identified: information and medical care needs, physical effects, psychological effects, interpersonal relationships and practical issues, yielding a total Cronbach’s Alpha of .95 (Martínez Arroyo et al., 2019). Other instruments used to conduct the present study were an informed consent form and an expert review form, designed for this study.
Data analysis
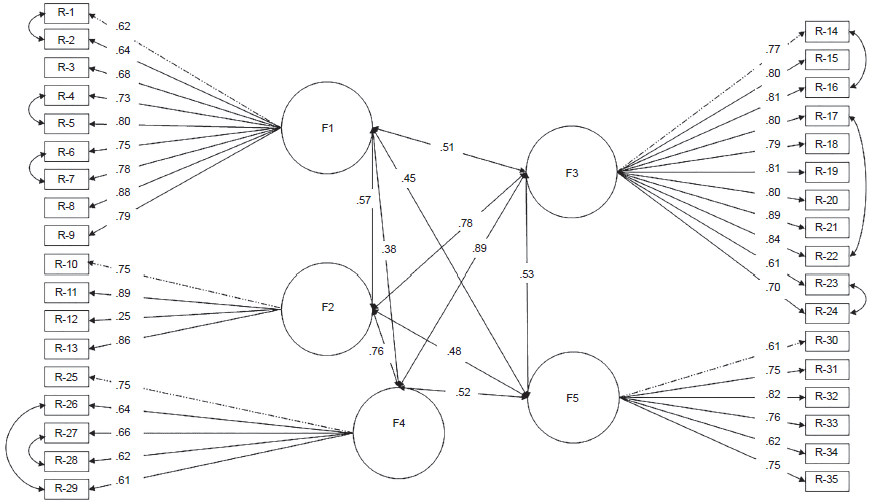
The study analyzed three aspects: content validity through the Aiken index, construct validity through factor analysis, and reliability through an internal consistency analysis. The following statistical programs were used: SPSS for internal consistency analysis, SPSS Amos (IBM) for confirmatory factor analysis (Figure 1), and the Spanish version of JASP .14.1. (Robalino et al., 2021) for exploratory factor analysis.
Procedure
Phase 1. Content validity
After adapting the base format, the adapted instrument (CaSUN-Mx) was submitted to a panel of expert judges to obtain content validity. Five experts specializing in oncology and psycho-oncology were asked to fill in the review form. In this form, they were asked to rate the wording and relevance of each of the items from 0-5. After the experts had answered, the data were analyzed with the formula to obtain the Validity V coefficient (Aiken, 1980). The criterion was the modification of items obtaining an index of less than .80 in the Aiken index.
Phase 2. Internal Consistency
The JASP statistical program (Robalino et al., 2021) was used for internal consistency analysis and exploratory factor analysis.
An internal consistency analysis was conducted to obtain reliability and the Cronbach’s Alpha coefficient. The Cronbach’s Alpha coefficient of the base questionnaire (CaSUN-S) was obtained so that it could subsequently be compared with the coefficient resulting from the internal consistency analysis of the adapted questionnaire (CaSUN-Mx). The total coefficient of the questionnaire and the coefficients per factor were obtained.
Phase 3. Construct validity
To evaluate construct validity, confirmatory factor analysis (CFA) was conducted before exploratory factor analysis on the grounds that the instrument used as a base is an existing instrument that has been validated for use in a Spanish population. For this analysis, AMOS and maximum likelihood were used, an analysis of covariance was undertaken and the goodness-of-fit indices of the base questionnaire were searched to test it. The following statistical indices: Chi square (Doral-Fábregas et al., 2018); degrees of freedom x²/df; values of the root mean square error rate (RMR) (Escobedo-Portillo et al., 2016); the goodness-of-fit index (GFI); the comparative fit index (CFI) (Hooper et al., 2008); the parsimony ratio index (PRATIO) and the parsimony comparative fit index (PCFI) (Sánchez et al., 2020); the noncentrality parameter (NCP); the root mean square error of approximation (RMSEA) value; the Akaike information criterion (AIC); the expected cross validation index (ECVI) (Escobedo-Portillo et al., 2016) and the HOELTER index to determine sample size adequacy (García Veiga, 2011) were used.
Since the indices failed to yield a good fit, the modifications suggested by the program were undertaken, such as conducting an analysis of covariances. Even though it had a better fit, it was decided to conduct an exploratory factor analysis to explore latent constructs.
In regard to exploratory factor analysis (EFA), the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of sphericity were obtained. Once the expected results had been obtained, it was possible to continue with the analysis. A principal axis analysis was performed as an extraction method to obtain communalities, in other words, the variance in each variable. The matrix of rotated components was analyzed, using the Oblimin rotation. Items correlating with more than one factor or with insufficient saturation in any factor were discriminated.
The adjustments suggested by the EFA were made, the final edition of the questionnaire was obtained and lastly internal consistency analysis was conducted again to obtain the Cronbach’s Alpha coefficient of the five subscales of the CaSUN-Mx survey and the total coefficient.
RESULTS
Phase 1. Content validity
The Aiken index yielded a coefficient of .98 for linguistic adaptation and a coefficient of .99 for cultural adaptation. Since all the coefficients were above the minimum threshold to be considered suitable (.80), so no modifications were made to the items (Table 3).
Table 3 ItemAiken validation
| Item |
Aiken language
index |
Aiken cultural
index |
|
|---|---|---|---|
| 1. | I need updated information | 1 | 1 |
| 2. | My partner and/or family needs relevant information | 1 | 1 |
| 3. | I need you to provide me with information in such a way that I can understand it | 1 | 1 |
| 4. | I need the best medical care | 1 | 1 |
| 5. | I need health care services that are available whenever I need them | 1 | 1 |
| 6. | I need to feel that I also participate, together with the medical team, in taking care of my health | 1 | 1 |
| 7. | I need to know that all my doctors talk to each other to coordinate the care I receive | 1 | 1 |
| 8. | I need any complaints I make about my medical care to be appropriately addressed | 1 | 1 |
| 9. | I need to have access to complementary services (such as physiotherapists and nutritionists) | .8 | 1 |
| 10. | I need help with managing the side effects and/or complications of my illness | 1 | 1 |
| 11. | I need help with adapting to the consequences of my illness on my quality of life | 1 | 1 |
| 12. | I need help with my fertility problems | 1 | 1 |
| 13. | I need help with adapting to the changes I have experienced in my physical appearance | 1 | 1 |
| 14. | I need help with reducing the stress levels in my life | 1 | 1 |
| 15. | I need help with coping with worry about my future because of my illness | 1 | 1 |
| 16. | I need emotional support | 1 | 1 |
| 17. | I need to talk to other people suffering from the same illness as me | .8 | 1 |
| 18. | I need help with moving forward with my life | 1 | 1 |
| 19. | I need help with coping with the changes in my thinking that nothing bad will happen in my life | 1 | 1 |
| 20. | I need help with knowing how to deal with people who don’t understand the impact my illness has on my life |
1 | 1 |
| 21. | I need help with managing both my own expectations and those of others regarding my illness | 1 | 1 |
| 22. | I need help with trying to make decisions about my life despite the uncertainty | 1 | 1 |
| 23. | I need help with exploring or analyzing my spiritual beliefs | 1 | 1 |
| 24. | I need help with finding a purpose my life | 1 | 1 |
| 25. | I need help with knowing how to support my partner and/or family | 1 | 1 |
| 26. | I need help with managing the impact of my illness on my relationship | 1 | 1 |
| 27. | I need help with establishing new social relationships due to my illness | 1 | 1 |
| 28. | I need help with knowing how to deal with the issue of my illness in social and/or work situations | 1 | 1 |
| 29. | I need help with addressing problems in my/our sex life | 1 | 1 |
| 30. | I need help with getting and/or keeping a job | 1 | 1 |
| 31. | I need help with finding out the possible financial benefits and/or subsidies to which I am entitled | 1 | .8 |
| 32. | I need help with arranging for life insurance and/or travel assistance due to my illness | 1 | 1 |
| 33. | I need help with getting legal advice due to my illness | 1 | 1 |
| 34. | I need more accessible parking at the hospital | 1 | 1 |
| 35. | I need someone such as a social worker who I can contact whenever I need information about available services |
1 | 1 |
| 36. | Please note any other needs you have experienced during the last month that you have not been previously asked about |
1 | 1 |
| Total | .98 | .99 |
Note: Review format to obtain content validity. Source: compiled by the authors.
Phase 2. Internal consistency
According to the analysis of the internal consistency of the base questionnaire (CaSUN-S), a coefficient of .95 Cronbach’s Alpha was obtained. After the item discrimination and exploratory factor analysis (EFA), the reliability coefficient was .87 for factor 1; .91 for factor 2; .87 for factor 3; .95 for factor 4 and .86 for factor 5.
Phase 3. Content validity
CFA yielded low values in CFI, TLI and RMSEA. The analysis of covariance undertaken by the modification indices shown indicated covariance between the errors of items 1 and 2, 4 and 5, 6 and 7, 14 and 16, 17 and 22, 23 and 24, 26 and 29, and 27 and 28 as well as a better fit.
After the adjustment of modification indices, the Chi-square value (x²) was 943.859 with 542 df. Table 4 shows the result of the statistical values produced by the CFA. The first column shows the name of the statistical value, the second the acceptable fit levels proposed by various bibliographic sources, and the third and fourth columns the results of the CFA values of the questionnaire used.
Table 4 Goodness-of-fit Indices of the CaSUN-S Survey in the Original Version
| Statistical index | Acceptable level of fit | Values obtained | Adjustment |
|---|---|---|---|
| x2/gl | Values 2-3, up to 51 | 1.741 | Not acceptable |
| RMR | About 01 | .083 | Acceptable |
| GFI | 1 = Perfect fit )( .95 Excellent fit |
.776 | Acceptable |
| CFI | Acceptable level of fit 0 = bad fit2 |
.909 | Acceptable |
| PRATIO | 0-1 perfect fit3 | .911 | Acceptable |
| PCFI | .828 | Acceptable | |
| NCP | < 2 = acceptable fit1 | 401.859 | Unacceptable |
| RMSEA | < .05 = aceptable fit1 | .064 | Unacceptable |
| AIC | Nearly 01 | 1119.859 | Unacceptable |
| ECVI | Nearly 11 | 6.256 | Acceptable |
| HOELTER | Greater than sample size4 | 114/118 | Acceptable |
Source: compiled by the authors.
Note:
1Escobedo-Portillo et al. (20166), p. 20;
In the exploratory factor analysis, a score of .916 was obtained on the Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy, indicating an adequate degree of relationship between the items. Bartlett’s sphericity test yielded an x² (Chi-square) = 4642.195, df = 595 and significance = .001, showing that it was appropriate to conduct exploratory factor analysis.
A distribution of variance was obtained in five components, distributed percentagewise as follows. The first component, “Psychological care needs” (16 items), accounted for 22.5% of total variance, the second, “Comprehensive care needs” (six items), accounted for 11.6%, the third, “Practical needs” (six items), accounted for 10.4%, the fourth, “Information needs” (three items) accounted for 7.9% and the fifth, “Needs related to side effects” (3 items), accounted for 7.5%. Together, the five factors accounted for 59.9% of total variance.
Table 5 shows the distribution of total explained variance in the five factors.
A factorial division into five components was identified. Table 6 shows the saturations of the items in the version with the corresponding adaptations of the questionnaire; values greater than .40 were considered in a single factor. Item 26, “I need help with managing the impact of my illness on my relationship,” was eliminated since it did not significantly correlate with any factor.
Table 6 ItemFactor loadings of the 34 items in the five factors
| Item | 1 | 2 | 3 | 4 | 5 | |
|---|---|---|---|---|---|---|
| 1. | I need help with my fertility problems | .434 | ||||
| 2. | I need help with reducing the stress levels in my life | .550 | ||||
| 3. | I need help with coping with worry about my future because of my illness | .560 | ||||
| 4. | I need emotional support | .585 | ||||
| 5. | I need to talk to other people suffering from the same illness as me | .472 | ||||
| 6. | I need help with moving forward with my life | .716 | ||||
| 7. | I need help with coping with changes in my thinking that nothing bad will happen in my life | .673 | ||||
| 8. | I need help with knowing how to deal with people who don’t understand the impact my illness has on my life |
.687 | ||||
| 9. | I need help with managing both my own expectations and those of others regarding hav- ing my illness |
.735 | ||||
| 10. | I need help with trying to make decisions about my life despite the uncertainty | .733 | ||||
| 11. | I need help with exploring or analyzing my spiritual beliefs | .799 | ||||
| 12. | I need help with finding a purpose in my life | .788 | ||||
| 13. | I need help with knowing how to support my partner and/or family | .512 | ||||
| 14. | I need help with establishing new social relationships due to my illness | .697 | ||||
| 15. | I need help with knowing how to deal with the issue of my illness in social and/or work situations |
.664 | ||||
| 16. | I need help with addressing problems in my/our sex life | .443 | ||||
| 17. | I need the best medical care | .537 | ||||
| 18. | I need health care services that are available whenever I need them | .748 | ||||
| 19. | I need to feel that I also participate, together with the medical team, in taking care of my health |
.820 | ||||
| 20. | I need to know that all my doctors talk to each other to coordinate the care I receive | .884 | ||||
| 21. | I need any complaints I make about my medical care to be appropriately addressed | .786 | ||||
| 22. | I need to have access to complementary services (such as physiotherapists and nutri- tionists) |
.623 | ||||
| 23. | I need help with getting and/or keeping a job | .561 | ||||
| 24. | I need help with finding out about the possible financial benefits and/or subsidies to which I am entitled |
.650 | ||||
| 25. | I need help with arranging for life insurance and/or travel assistance due to my illness | .836 | ||||
| 26. | I need help with getting legal advice due to my illness | .747 | ||||
| 27. | I need more accessible parking at the hospital | .635 | ||||
| 28. | I need someone such as a social worker who I can contact whenever I need information about available services |
.700 | ||||
| 29. | I need updated information | .803 | ||||
| 30. | My partner and/or family needs relevant information | .802 | ||||
| 31. | I need you to provide me with information in such a way that I can understand it | .688 | ||||
| 32. | I need help with managing the side effects and/or complications of my illness | .552 | ||||
| 33. | I need help with adapting to the consequences of my illness on my quality of life | .656 | ||||
| 34. | I need help with adapting to the changes I have experienced in my physical appearance | .543 |
Note: Factor loadings on principal components.
DISCUSSION AND CONCLUSION
The objective of the present study was to validate the CaSUN-Mx measure adapted for use in the Mexican population of adult cancer survivors.
Confirmatory factor analysis (CFA) was conducted to analyze how the base questionnaire performed in the eligible population. It was decided to undertake this procedure prior to exploratory factor analysis (EFA) on the grounds that the base questionnaire would have an adequate fit in our population because it already existed. The CFA results indicated that the questionnaire did not have a completely adequate fit. The modification indices indicated covariance between some of the items as a result of which a better overall adjustment was obtained. However, EFA was undertaken to test the questionnaire again and seek possible dimensions or latent constructs after it had been answered by our population (Martínez-Arias et al., 2014).
The results of the EFA pointed to the need to alter the structure of the questionnaire, after modifying the factors and items and having obtained adequate reliability of the final version of the questionnaire. In future research, another CFA should be conducted with a different population to test the fit of the final version of the questionnaire and the new structure obtained in EFA (Martínez-Arias et al., 2014).
In regard to the factors obtained in the final version, Factor 1 of the base questionnaire “Information needs and medical care” was divided into two factors called “Information needs” (three items) and “Comprehensive and collaborative care needs” (six items). The separation of this factor can be explained by the fact that, in our population, the two variables function both independently and significantly. The factor referring to the need for comprehensive, collaborative care was so-called because it refers to the need to have access to complementary services and interprofessional or collaborative care, in other words, between professionals working towards a common goal and sharing a team identity (Körner et al., 2016). Collaborative practice in the field of health refers to the work undertaken by health professionals from different disciplines who provide comprehensive care by working directly with patients, their families, caregivers and communities to provide high-quality service. This is achieved through interprofessional or transdisciplinary education, which occurs when different professionals know what each one does, learn from them and learn together to promote effective collaboration (World Health Organization [WHO], 2010).
One of the limitations of the study was that it failed to include a question on whether respondents had been treated in the public or private sector. It is important to know this for future research and for the generation of intervention programs because answers from the two groups vary considerably. Another limitation was that since the study was conducted during the COVID-19 pandemic, the context and consequences of the latter could have affected results, as well as creating further needs, which were not reported. Hence the importance of analyzing the answers obtained in item 35 “Please write down any other needs you have experienced during the last month and have not been previously asked about.” A qualitative analysis of the answers should also be conducted.

