












 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
Permalink
Introduction
Prostate cancer (PCa) is one of the leading causes of cancer-related death in men worldwide.1 PCa is the second most commonly diagnosed cancer in men, with an estimated 1.4 million diagnoses worldwide in 2020.2 Despite careful patient selection before treatment for PCa, post-treatment relapse with curative intent is frequent, partly due to the insufficient sensitivity and specificity of existing standard imaging modalities such as computed tomography (CT) and bone scintigraphy (BS) in detecting non-localized disease.3
Prostate-specific membrane antigen (PSMA) is a transmembrane glycoprotein that is highly overexpressed in almost all PCa cases, with expression levels increasing with higher tumor grade and stage. PSMA ligands are small molecules that bind to the active site of the extracellular domain of PSMA.4
Currently, studies have reported the use of PSMA PET in both primary staging and evaluation of biochemical recurrence; however, most published data focus on biochemical recurrence of prostate cancer, which is currently the main indication for PSMA PET use.
The proPSMA study conducted in men with PCa undergoing staging prior to curative-intent therapy found that PET PSMA outperformed conventional imaging in detecting distant disease in high-risk patients.
The objective of our study was to evaluate if there were changes in the staging of CaP using PSMA PET compared to standard diagnostic methods. Additionally, if changes occurred, we aimed to understand how these modifications impacted the treatment of patients with an initial diagnosis of CaP, particularly in relation to the D'Amico risk score.
Material and methods
A prospective observational study was conducted in patients with an initial diagnosis of PCa who underwent standard staging studies (CT and BS) and PSMA PET. Patients were eligible if they had histopathologically confirmed PCa by transrectal prostate biopsy and were being considered for curative-intent radiotherapy following staging with conventional diagnostic methods and PSMA PET. Patients were excluded if they had contraindications for PSMA PET. A focal increase in tracer uptake greater than the background and not associated with physiological uptake was considered a positive result for PSMA PET. The evaluated qyevariables included age, International Society of Uropathology (ISUP) grade, clinical stage (TNM), prostate-specific antigen (PSA) level, D'Amico risk score,5 results of CT, BS, PSMA PET, and treatment change. Intensity-modulated radiotherapy (IMRT) was administered, delivering 60 Gy to the prostate gland and 40 Gy to regional lymph nodes (Figure 1).
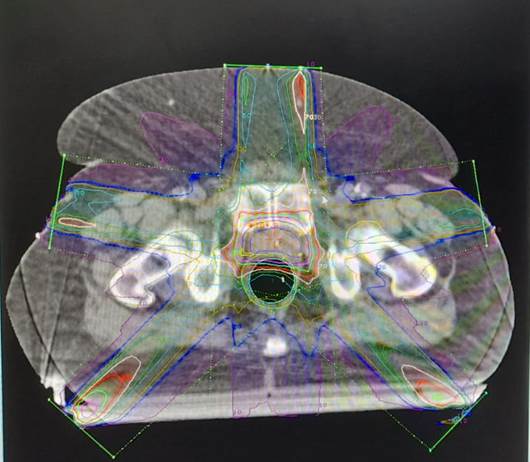
Treatment change was defined as an increase in the radiation dose (boost) by focal delivery of 60 Gy to suspected lesions of extraprostatic disease localized in the iliac chain (N1). Risk groups were defined according to D'Amico scores as low, intermediate, and high risk, respectively. Statistical analyses were performed using SPSS 28 software. Descriptive measures for quantitative variables included mean and standard deviation or median and quartiles 1 and 3. Absolute frequencies and percentages were used to describe qualitative variables. 95% confidence intervals (95% CI) were calculated. Proportions were compared using Pearson's chi-square test. The selected significance level was α = 0.05.
Results
From October 2019 to August 2020, 40 patients diagnosed with PCa were staged using standard diagnostic methods and PSMA PET. Table 1 presents descriptive characteristics of the patients.
Table 1 Age distribution and urological profile of the patients
| Variable | |
| Age (Mean ± SD ) [years] | 68.6 ± 7.6 |
| ISUP % (N) | |
| 1 | 7.5 (3) |
| 2 | 15 (6) |
| 3 | 37.5 (15) |
| 4 | 30 (12) |
| 5 | 10 (4) |
| D’amico Score % (N) | |
| Low risk | 7.5 (3) |
| intermediate risk | 40 (16) |
| High risk | 52.5 (21) |
| PSA (Median (Q1-Q3)) [ng/ml] | 10.2 (6.5-21.2) |
In the 40 patients, 40% (n=16) of the initial stagings changed according to the results obtained.
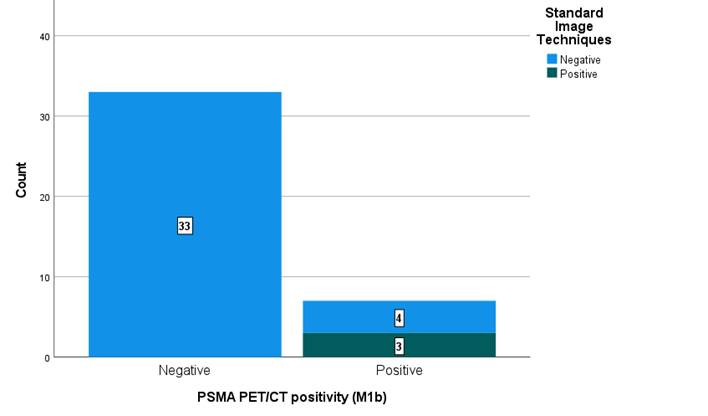
In the TNM classification, it was observed that, in the detection of bone metastases (M1b), out of 7 cases where the PET PSMA gave positive results, the standard methods were negative in 57% (n=4) of them (Figure 2).
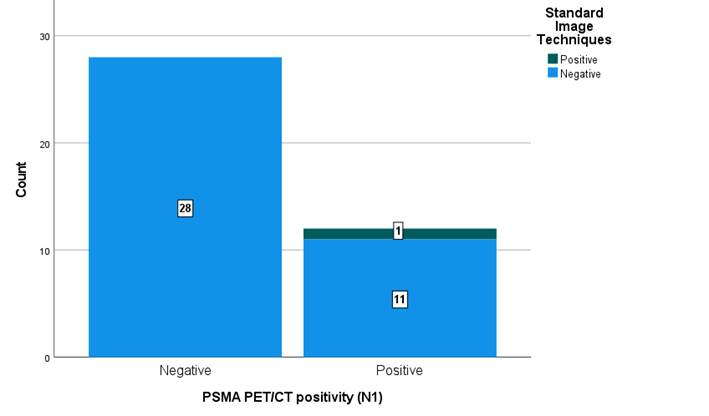
In addition, in the detection of locoregional adenopathies (N1), out of 12 cases where PET PSMA gave positive results, standard methods were negative in 92% (n=11) of them. (Figure 3).
In the detection of non- locoregional adenopathies (M1a), out of 4 cases where the PET PSMA gave positive results, the standard methods were negative in 100% (n=4). Finally, the evaluation of visceral metastases (M1c) did not present positivity neither in PET PSMA nor in standard methods.
Following the PSMA PET, the uro-oncology committee decided that 27.5% (n=11) of the initial treatment plans should be modified based on the captured extra-prostatic images from the PSMA PET, leading to a radiation boost.
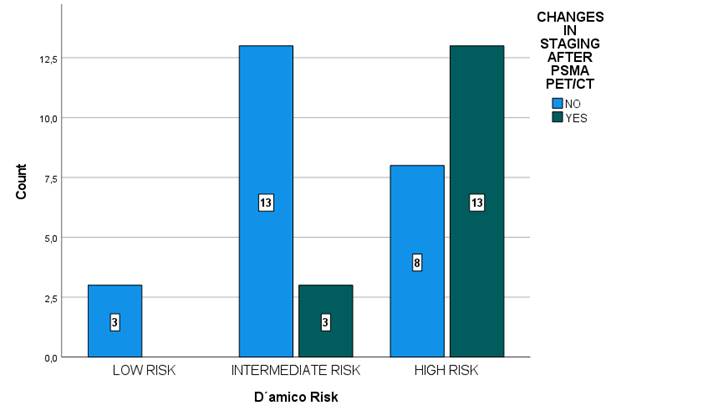
When correlating the change in staging from the PSMA PET with the D'Amico risk score, it was observed that there were no changes in the low-risk group, 19% changes in the intermediate-risk group, and 62% changes in the high-risk group. These differences were statistically significant (χ^2=9.2; df=2; p=0.01) (see Figure 4).
Discussion
The PET-PSMA is widely used for the evaluation of biochemical recurrence of PCa and has recently been employed for initial staging prior to treatment. A multicenter study evaluating the use of PSMA in initial staging of patients with negative bone scintigraphy showed that PET-PSMA yielded positive results in 17 patients, resulting in a sensitivity of 41.5 % (95 % CI: 26.7 %-57.8 %) and specificity of 90.9 % (95% CI: 79.3 %-96.6 %) for bone metastasis assessment.6 A retrospective study utilizing PET-PSMA for initial assessment of 206 PCa patients found a specificity of 93.5 % and a sensitivity of 38.2 % for detecting nodal disease.(7) A multicenter clinical trial assessing the initial staging of PCa using conventional imaging and PET-PSMA demonstrated that PET-PSMA had a 27 % higher diagnostic accuracy than conventional imaging. He also showed lower sensitivity (38 % vs. 85 %) and specificity (91 % vs. 98 %) in favor of PET-PSMA.3 Our analysis was demonstrated the highest diagnostic accuracy of PET-PSMA compared to conventional imaging. Specifically, 57 % of positive bone findings on PET-PSMA (M1b) were negative on standard diagnostic methods. Additionally, in the detection of locoregional lymph nodes (N1), standard methods were negative in 92 % of the 12 cases where PET-PSMA yielded positive results. Similarly, in the detection of non-locoregional lymph nodes (M1a), standard methods were negative in 100 % of the 4 cases where PET-PSMA showed positive results.
The higher diagnostic accuracy of PET-PSMA has prompted the medical community to assess whether the increased positivity of the study changes therapeutic strategies. The proPSMA study found that conventional imaging led to a change in treatment intention or modality in 15 % (95% CI: 10 %-22 %) of patients, compared to 28 % (95 % CI: 21 %-36 %) for those who underwent first-line PET-PSMA (p=0.008).3 In our study, the use of PET-PSMA resulted in a treatment modality change in 27.5 % of cases, supporting previous findings.
The proPSMA clinical trial only evaluated high-risk patients according to the D'Amico risk score and assessed treatment changes in this group. Our analysis not only included patients at high risk of recurrence after treatment but also incorporated those at intermediate and low risk of recurrence according to the D'Amico score. We observed 0 % changes in the low-risk group, 19 % changes in the intermediate-risk group, and 62% changes in the high-risk group (χ^2=9.2; df=2; p=0.01).
The primary function of any imaging diagnostic test is to provide accurate results. Our study continues to demonstrate the unequivocal superiority of PET-PSMA compared to conventional imaging. This finding can be attributed to the high uptake and specificity of the PSMA radiotracer, enabling the identification of small-volume nodal or visceral disease and early bone metastases before lytic or blastic changes occur.
Conclusion
In our study, PET-PSMA demonstrated an initial staging change in 40% of cases. When comparing it with the D'Amico risk score, we observed that higher risk was associated with a higher probability of staging change. Based on our analysis, it can be inferred that PET-PSMA is a useful tool for staging patients at moderate and high risk prior to radiation therapy.

