












 (pdf)
(pdf)




 SciELO
SciELO  SciELO
SciELO 
 Permalink
PermalinkIntroduction
According with the World Health Organization (WHO) odontogenic keratocysts (OKCs), earlier known as keratocystic odontogenic tumors, is defined as «benign uni-or multicystic, intraosseous tumor of odontogenic origin, with a characteristic lining of parakeratinized stratified, has slow growth at the beginning, but with potential for aggressive, infiltrative behavior».1-4 There has been cases reports of OKCs in other nonosseous locations,which involve the gingiva, but mucosal, epidermal and even intramuscular sites.3 OKCs presents as swelling with or without painand occasionally paresthesia of the lower lip3,4 The cyst may reabsorb bone and cause a secondary teeth displacement with consequent malocclusion. The current literature cites a broad range of recurrence (0-62%), with most recurrences presenting within 5 years on average after a surgical treatment, if not removed completely.3),5 It affects the mandible in a greater proportion than maxilla (60-75%). It is more common in the posterior ramus of the mandible, whereas in maxillae is in the third molar and cuspid region.3,4,6-8 The frequency varies from 11 to 21% and it can appear at any age (8-82 years), but shows predominance in patients between 20 and 40 years with higher male prevalence (1.6:1).3,4,6,8 It is one of the rare and distinctive developmental odontogenic cyst which from the dental lamina, it is named this way because keratin is produced by the cystic lining.4 A Cyst is an abnormal cavity, lined with 6 to 10 cell layer parakeratinized stratified squamous epithelium, and athin walled within the bone. It contains clear liquid or semi-liquid fluid with a cheesy material representing parakeratin produced by the luminal epithelium, mesenchymal and/or ectomesenchymal that are or were part of the odontogenesis process.4,6 Under the microscope OKCs exhibits a wavy, corrugated surface with a prominent, palisaded and hyperchromatic basal cell layer, with epithelium that has a flat interface with the adjacent connective tissue.4,6 Treatment with marsupialization «decom-pression or cystotomy» also results in the loss of classic features, with the lining becoming reminiscent of the normal adjacent mucosa. The epithelium may strip away from the connective tissue in these cysts, therefore close examination of the biopsy container for material is recommended.1,4), (8,9 Treatment options range from a conservative approach to extensive surgery that include enucleation with cryotherapy, marsupialization, decompression and segmental resection.4,6,9
Clinical case
72 years old male was referred to the Facultad de Odontologia, Universidad Autónoma de Guadalajara for routine evaluation. On physical examination there was an asymptomatic patientwith preserved oral cavity, normochromic mucosa, and symmetric bone structure (Figure 1). Routine orthopantomography was requested and it demonstrated a radiolucent left maxilla region, molars and pre-molars (Figure 2). By to computed tomography (CT) with 3D reconstructionshe showedhypodense circular area (1.9 × 2.5 × 2.0 cm) with defined edges (Figure 3A) communicated with the nasal cavity, osteolysis in the palatine region and the anterior wall of the left maxilla (Figure 3B).
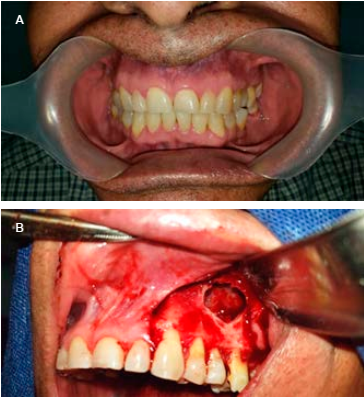
Figure 1 Intraoral of view. A) Mucosa coloration normal and bone structures are symmetric. B) Surgical resection of the Keratocyst, was confirmed bone lysis in the palatal region and communication with the ipsilateral nostril.
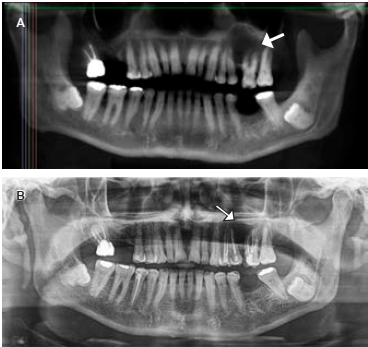
Figure 2 Orthopantomography. A) The arrow shows radiolucent area with a defined edge defined, B) Control orthopantomography at 6 months. The area occupied by the Keratocyst is in frank recovery.
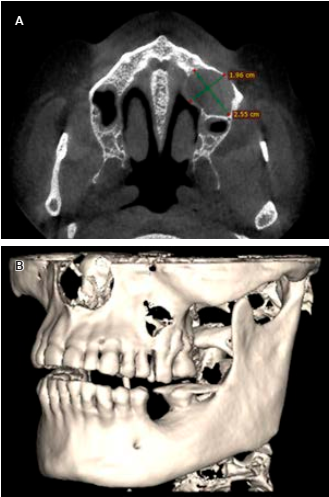
Figure 3 Computed tomography scan cut axial facial (CT) shows. A) Radiolucent circular area in left maxillary sinus of 1.96 × 2.55 cm. B) Bone destruction in the anterior wall of the left maxillary sinus.
Treatment: the enucleation was done under local anesthesia with a combination of a peripheral osteotomy using the rotary instrument through a canine triangular mucoperiostic flap in the second molar of the left maxillary. Osteolysis was found in the palatal region communicated with the ipsilateral nostril, previously observed on the 3D reconstruction (Figure 1B). Removal was performed and a sample was placed in 10% formaldehyde for laboratory histopathology examination. This technique was used since the complete removal of the cyst possessed no risks of complications from a dental and/or anatomical point of view. Furthermore, this method facilitated the comprehensive analysis of the lesion including its clinical, histopathological, and radiological aspects.
Presumptive diagnosis: due to location, clinical characteristics, radiography, absence relation between the retained tooth and patient’s age, it is set a presumptive diagnosis of Giant Cell Central Granuloma or OKC.
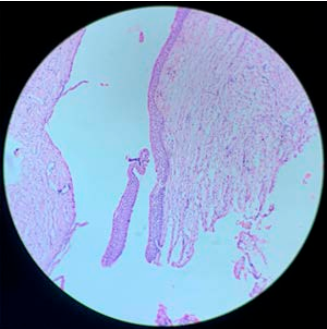
Definitive diagnosis: the histopathology reports a cavity without apparent content, thin odontogenic epithelium lining without projections towards its capsule and detached in most sections of its fibro-connective capsule. Flat stratified epithelium of 6 to 8 cell strata, hyperchromatic basal layer and para-keratinized surface were identified, with all these pathological features allow the diagnosis of OKC (Figure 4).1,6,7
Discussion
The database patient records of the Department of Maxillofacial Surgery of the Facultad de Odontología de la Universidad Autónoma de Guadalajara from June 2014 to November 2019 was reviewed. Recognition of 132 biopsies was found, two of them wereodontogenic cysts (2.3%), one dentigerous and oneradiquar. However, as it shown in Table 1, four articles were located in the review of works analyzing odontogenic cyst cases in Mexican population(tree carried out in Mexico City and one in San Luis Potosi City). Of the total Biopsies 9,673,of which 1,266 (13.1%) were diagnosed as odontogenic cysts and 306 cases (24.2%) were OKCs.10-13 In Mexican data base (Table 1), both percentage of odontogenic cysts (Table 2) and the slight preponderance of OKCs in menwere similar to those described in the literature.3,4,6,8 On the other hand, the percentage of OKC was different in the Mexican population (24.2%) than the other population, in which the percentage varies from 1.69 to 18.6%. It is mostly probable that the difference in the percentage of OKC between the review of the other population, Mexican and our database, could be due to the difference in years analyzed or the number of cases treated per year. Also, it could even be due to diagnostic methods, even if it is not described, it could have involved some genetic component, since the variability between one study and the another is quite wide (Table 1). Therefore, this represents a rare case, if the whole clinical picture is considered as a whole, since OKC according to the literature occurs at all ages with peak incidence in the 2nd and 4th decade of life, but is more frequent in the second decade of life,4 even in Mexican population.21 Nevertheless in our clinical case, the patient was 75 years old and the oldest person of the all cases we knowledge with OKC in the maxilla, further OKC in maxillary region are rare with a low frequency in the left region (Table 2),4,6,7 as Cadena-Anguiano described it in Mexican population study.14 However, the maxillary involvement owns a greater and increased threat, due to proximity to vital structures such as maxillary sinus, orbital floor, and infratemporal fossa.15 Medline, Google Scholar and Google search was performed using the MeSH term «keratocyst», combined with the word «maxilla» and «case report». We detected 32 cases of maxilla OKCs, includes our case (Table 2), and it is noted that 34.4% of all cases described were from India, 15.6% from Brazil and 9.4% (three cases, including ours) from Mexico. In these studies, 46.9% were in the left maxilla, 65.6% without pain, 43.7% without retention of dental organ and 53.1 % without bone lysis. Of the 32 cases, only 3 cases (9.4%) (Including ours) did not show any symptoms, however, they developed bone lysis (Table 2).
Table 1 Odontogenic cysts in Mexican and other countries population.
| Year period | Per year | Biopsies | Odontogenic cysts type | City, ref. | ||||
|---|---|---|---|---|---|---|---|---|
| Total | O. cysts | OKCs | Dentigerous | Radiquar | Other | |||
| n (%) | n (%) | n (%) | n (%) | n (%) | ||||
| 5 | 26 | 132 | 3 (2.3) | 1* | 1 | 1 | 0 | Gdl. City, Mex. 2020* |
| 18 | 70 | 1,266 | 103 (8.1) | 34 (33) M (50) | 58 (56) | 5 (4.9) | 6 (5.9) | SLP City, Mex.10 |
| 6 | 116 | 700 | 75 (10.7) | 30 (40) M 13 (43.3) | 21(28) | ND | 24 (32) | Mex. City, Mex.11 |
| 21 | 210 | 4,410 | 856 (19.4) | 184 (21.5) M 108 (58.7) | 283 (33) | 342 (39.9) | 47 (5.6) | Mex. City, Mex.12 |
| 10 | 386 | 3,865 | 304 (7.9) | 57 (18.7) M 34 (59.6) | 108 (35.5) | ND | 139 (45.7) | Mex. City, Mex.13 |
| 9,673 | 1,266 (13.1) | 306 (24.2) M 155 (50.5) | 45.7 (37.2) | 348 (27.5) | 216 (17) | Mexican10-13 | ||
| 11 | 2,370 | -- (10.7) | --- | 122 (5.2) | --- | 93 (3.9) | American 19 | |
| 04 | --- | 475 | 340 (71.6) | 23 (6.8) | 77 (22.6) | 216 (63.5) | 24 (7.1) | Turkey 20 |
| 10 | 8,563 | 1,518 (17.7) | 282 (18.6) | 366 (24) | 506 (33.2) | 126 (8.4) | Iranian 21 | |
| 58 | 1,305 | -- (18.5) | 22 (1.69) | 123 (9.4) | 68 (5.2) | --- | Australian 22 | |
| 10 | --- | 125 (---) | 17 (13.6) | 28 (22.4) | 76 (60.8) | 4 (3.2) | Indian23 | |
| 12 | --- | 406 (11.26) | 61 (15.02) | 57 (14.04) | 186 (46.06) | 102 (24.9) | Brazilian24 | |
M = male, O. cysts = odontogenic cysts, OKCs = keratocysts, SLP = San Luis Potosí.
* This case.
Table 2 Odontogenic keratocys no syndrome in the maxillary region.
| Age (yr)/ gender | Side | Symptom | Tumor | Tooth | Bone lysis | Country, ref. | |||
|---|---|---|---|---|---|---|---|---|---|
| Time | Swelling | Pain | |||||||
| 1 | 6/F | Left | -- | + | - | - | - | Japan 24 | |
| 2 | 7/M | Right | 60 d | + | Continuous non radiating | + | - | India 25 | |
| 3 | 8/M | Right | 1 yr | + | - | + | + | India 26 | |
| 4 | 9/F | Both | --- | + | - | Solid | + | - | USA 27 |
| 5 | 14/F | Left | --- | - | - | - | + | Brazil 28 | |
| 6 | 14/M | Right | 14, yr | + | - | Purulent fistula | + | - | Brazil 29 |
| 7 | 15/M | Right | 60 d | - | Tooth painon | - | + | India 30 | |
| 8 | 15/F | Left | 90 d | + | Moderate, radiating | + | + | India 31 | |
| 9 | 15/M | Right | 3 yr | + | + | Pus discharge | + | + | India 32 |
| 10 | 17/M | Left | 7 d | - | Persistent headache | Milky White Liquid | + | - | Brazil 30 |
| 11 | 18/F | Right | 4 yr | + | Light recurring | Cheesy fluid | - | - | Mexico 34 |
| 12 | 18/F | Left | - | - | - | - | - | Korea 35 | |
| 13 | 19/M | Right | - | - | - | + | - | Mexico 36 | |
| 14 | 21/M | Both | 7 d | + | Continuous, non-radiating | - | + | India 37 | |
| 15 | 22/F | Left | 6 m | + | Intermittent | - | - | - | UK38 |
| 16 | 22/F | Left | - | - | - | - | + | India 39 | |
| 17 | 23/M | Left | 90 d | + | - | + | - | Spain 40 | |
| 18 | 26/F | Right | 1 yr | + | - | + | - | Iran 41 | |
| 19 | 27/F | Right | - | - | + | + | + | Brazil 42 | |
| 20 | 28/F | Right | 30 d | + | - | + | - | Brazil 43 | |
| 21 | 32/M | Left | 90 d | + | - | + | + | Spain 44 | |
| 22 | 32/M | Left | 60 d | + | - | + | + | India 45 | |
| 23 | 34/M | Left | -- | + | + | Green, cheesy Fluid discharge | - | - | USA 46 |
| 24 | 36/F | Right | 30 d | - | - | Tumefaction, straw colored Fluid | + | + | Kosovo 47 |
| 25 | 39/F | Right | 0.5 yr | + | + | No fluid | + | - | Japan 48 |
| 26 | 45/F | Right | 0.5 yr | + | - | - | + | India 15 | |
| 27 | 46/F | Left | 30 d | + | - | - | - | India 49 | |
| 28 | 54/M | Left | ND | - | -- | - | + | Korea 50 | |
| 29 | 57/M | Left | ND | - | - | + | + | Korea 50 | |
| 30 | 64/F | Right | 30 d | - | Intermittent non radiating | + | - | India 51 | |
| 31 | 72/M | Right | Several months | + | - | - | - | - | Israel 52 |
| 32 | 75/M | Left | - | - | - | Solid | - | + | Our case, Mexico |
| n = 32 M n = 16 50% | Left n = 15 46.9% | Min.- max. 7 d-4 yr | (-) n = 12 37.5% | (-) n = 21 65.6% | (-) n = 14 43.7% | (-) n = 17 53.1% | |||
F = female, M = male, MS = maxillary sinus, yr = year, m = months, d = days, RE = recurrence after surgery, ND = no data.
On the other hand, odontogenic cysts constitute a group of maxillary lesions, which cause their destruction and due to its aggressive potential, as well as its high recurrence rate, surgical treatment has been controversial challenge. The decision will depend on multiple factors, mainly anatomical location, size and compromised anatomical structures with the objective of eradicating the lesion and decrease complications as small as possible.16-18 Considering our patient OKC, it caused bone lysis in the mouth palatine region as well as communication with the nostril, conservative treatment decision was made, in order to avoid damage to the nostril, as well as the palatine region. Based on the fact that the OKC is a lesion that has a high recurrence rate3,4,6,8 and to reduce this risk, it was decided to perform peripheral osteotomy with a rotary instrument after enucleation in order to decrease the recurrence rate. After resection of the lesion, taking into account the OKC as a presumptive diagnosis, it is decided to carry out adjuvant therapy discarding the Carnoy solution and Cryotherapy to avoid damage to the soft tissues of the palatine region and nasal fossa, in addition a radiographic surveillance is established every 6 months, the first one (Figure 4) shows adequate bone healing and decreased defect, and no evidence of recurrence. The cause of recurrence is not entirely clear, but it is attributed to the thin and friable layer of connective tissue of the cyst which results in incomplete removal or the presence of satellite cysts.9, 53
Conclusion
Although the OKC is an entity with a high recurrence, it should be considered that aggressive treatment is not advisable in all cases, due to factors such as commitment to anatomical structures and possible complications should be considered, however radiographic controls are advised periodically.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patients have given their consent for their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.

