











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Pancreatic cancers are known for having an aggressive evolution and a high mortality rate. The disease accounts for approximately 3% of all cancers, being the eighth and tenth most common cancer in women and men, respectively1. Major risk factors are smoking, obesity, diabetes, chronic pancreatitis, and occupational exposure.
The following case demonstrates a 63-year-old Mexican woman who presented with undifferentiated pancreatic carcinoma with osteoclast-like cells mimicking a cystic tumor with a successful surgical treatment and disease-free survival of more than 3 years.
Methods
This manuscript was prepared in accordance with the CARE guidelines (CAse REport guidelines) which are part of the EQUATOR international network. The aim of following these recommendations is to ensure the transparency, completeness, and methodological quality of this clinical report.
All patients data were collected ensuring at all times the confidentiality of the information and the anonymity of the patient.
The patient gave verbal and written informed consent for the use of her clinical information for academic and scientific publication purposes.
Case presentation
Our patient, a 63-year-old female, with a personal history of type 2 diabetes mellitus and systemic arterial hypertension for 10 years, stopped occasional smoking 15 years ago.
Onset 1 year before diagnosis with intermittent abdominal pain, abdominal distension, early satiety, nausea and vomiting, weight loss of 8 kg in 2 months, reason for which she attends to receive medical attention in a private setting where a CT scan is performed finding a pancreatic giant septate cyst heterogeneous lesion being referred to our institution where it was studied and scheduled for surgery (Fig. 1).
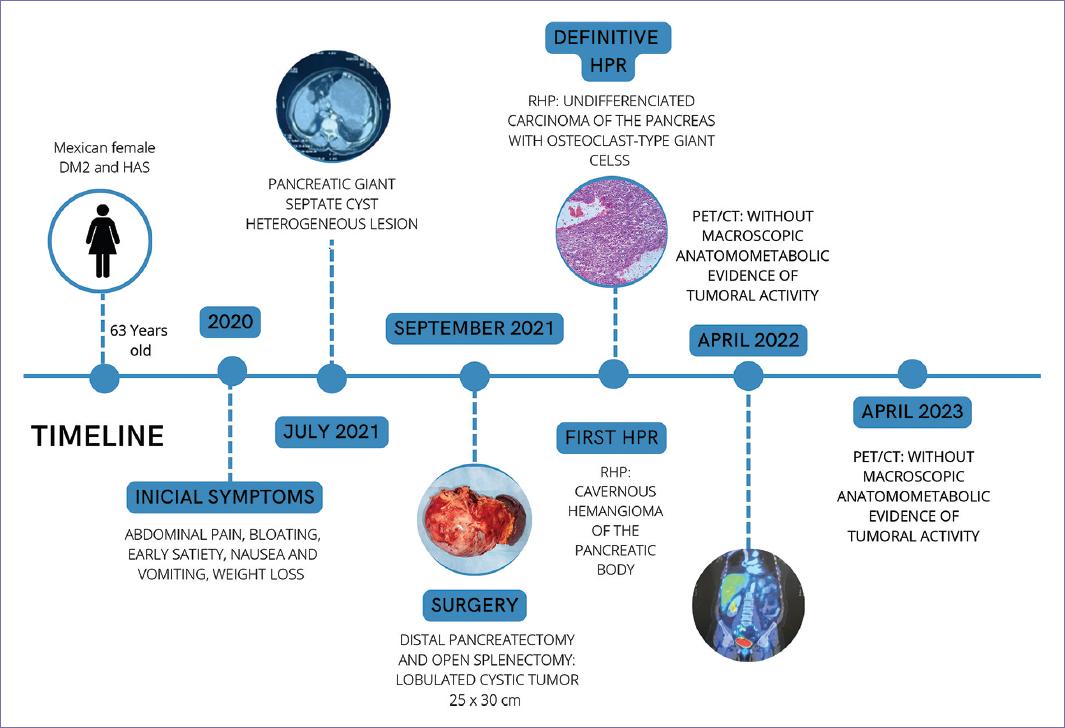
Surgery 09/25/2021: The procedure was performed with mixed epidural anesthesia in addition to balanced general anesthesia, requiring low-dose vasopressor (norepinephrine) during the procedure. Distal pancreatectomy and open splenectomy were performed, finding a lobulated cystic tumor of the pancreas measuring 25 × 30 cm, adhered to the transverse colon and posterior wall of the stomach, bleeding during surgery: 800 cc, with no complications reported (Fig. 2).

Figure 2 Surgical piece result from distal pancreatectomy and open splenectomy: lobulated cystic tumor of the pancreas measuring 25 × 30 cm.
Preliminary histopathological result showed a pancreatic cystic tumor in the body and tale. Spleen congestive, micronodular. Pancreas measuring 16 × 10 × 10 cm with 8 cm lesion with hemorrhagic content, multilobulated, negative for malignancy. Morphologically compatible with cavernous pancreas hemangioma.
Definitive HPR showed Undifferentiated pancreas carcinoma with osteoclast-type giant cells with patent vascular permeation, non-assessable edges, splenic parenchyma with congestion signs, and focal peri-splenitis without evidence of tumor activity; The Immunohistochemistry showed: CD31 negative, CD68 positive in osteoclast-like giant cells and macrophages, weak EMA positive, Ki67 positive nuclear in 15% and weak CKC positive in neoplastic cells concluding the diagnosis (Fig. 3).
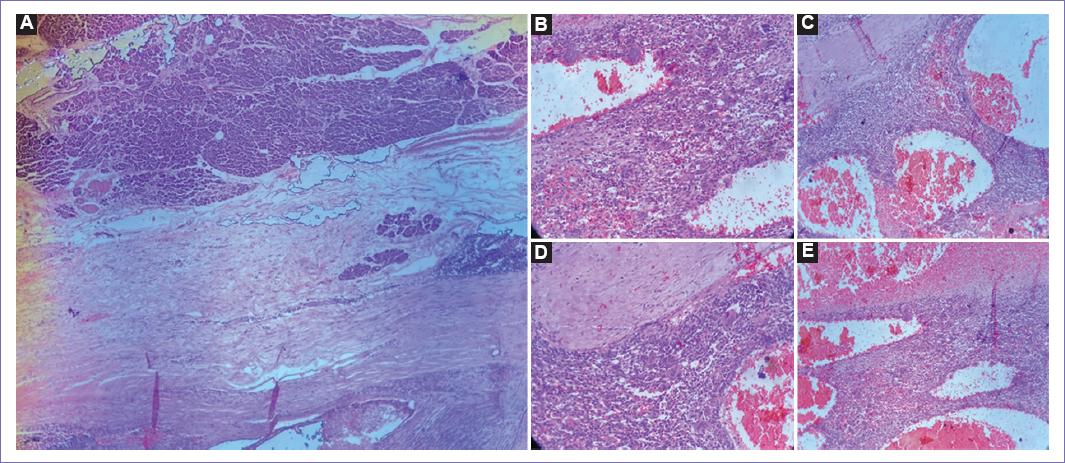
Figure 3 Paraffin blocks and slides stained with hematoxylin and eosin, reported as pancreas body and tail tumors. A: microscopic images showing neoplastic proliferation with nodular pattern displacing pancreatic parenchyma and stroma. B: osteoclast-type giant cells. C: congestive ectatic vascular lumina with hemorrhagic degeneration. D: fibroblasts proliferation with endocrine pancreatic tissue. E: splenic tissue with red and white pulp. Congestive periarteriolar capillary network.
After showing improvement and being discharged, she was referred to the outpatient medical oncology clinic, which requested the following studies.
18FDG PET/CT: 26.04.22: Study without macroscopic morphometabolic evidence of tumoral activity. Post-surgical changes due to subtotal pancreatectomy, splenectomy, and hysterectomy. Hepatic steatosis. Signs of spinal degenerative osteoarticular pathology (Fig. 4).
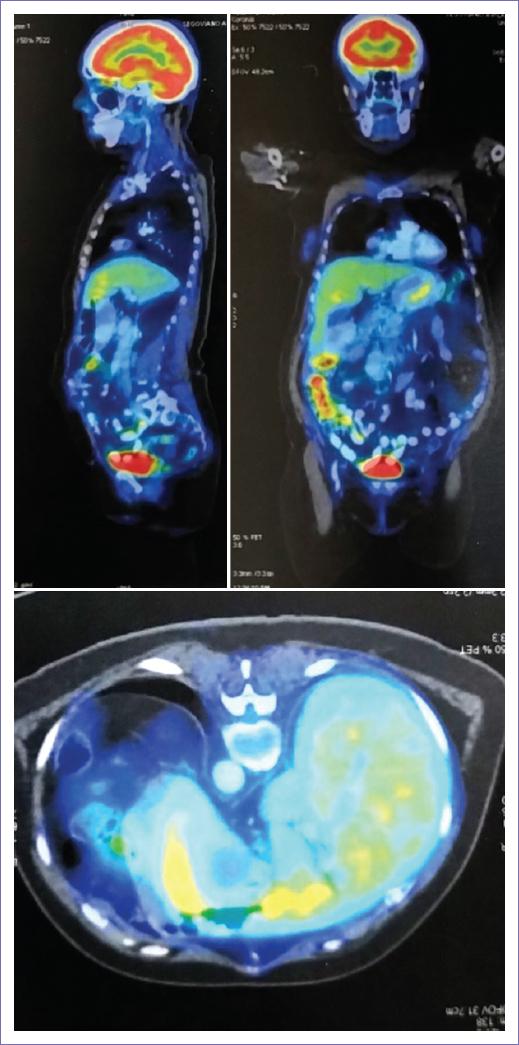
Figure 4 April 26, 2022. F-FDG PET/Whole body CT: no macroscopic anatomical-metabolic evidence of tumor activity. Post-surgical changes due to subtotal pancreatectomy, splenectomy, and hysterectomy.
CT April 2023: Post-surgical changes at the pancreas level with absence of the body and tail, without lesions or masses in the surgical bed. Changes due to splenectomy without obvious lesions, but with residual fatty striation. This study shows no evidence of recurrence or new lesions in the surgical bed of the known primary tumor (Fig. 5).
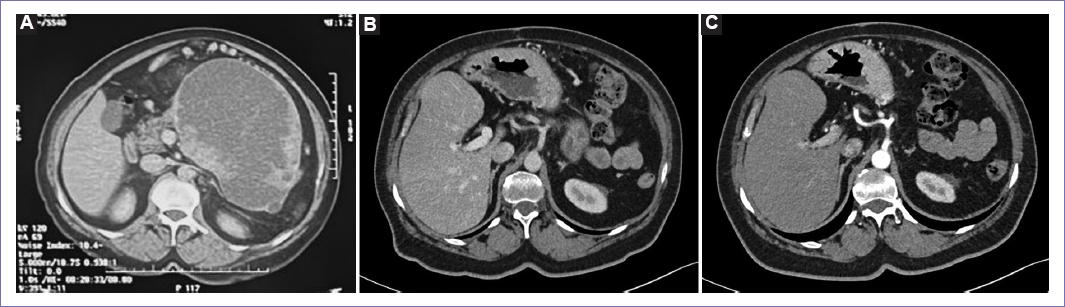
Figure 5 Tac scan: A: previous to surgery, May 2021. B: two-years after surgery, August 2023. C: three-years after surgery, May 2024.
CT AUGUST 2023: No changes. Shows no evidence of recurrence or new lesions. Laboratory results 12.08.23: Normal, CA 19-9: 3.0.
Laboratory results 05.27.24: Complete blood count normal, comprehensive metabolic panel with glucose 140, liver function tests normal, CA 19-9: 3.3 (Table 1). These studies demonstrated that the patient is free of disease. Remains under observation and monitoring
Table 1 Laboratory results and tumor markers. Mammogram May 27, 2024: BI-RADS 0
| Parameters | July 28, 2021 | December 30, 2021 | April 28, 2022 |
|---|---|---|---|
| HGB (g/dL) | 10.1 | 13.9 | 11.8 |
| HCT (%) | 32.9 | 44.1 | 36.4 |
| WBC (103/μL) | 6.74 | 9.9 | 13 |
| NEUT (%) | 63 | 47.4 | 84 |
| PLT (103/μL) | 92 | 345 | 84 |
| Parameters | July 28, 2021 | September 29, 2021 | April 28, 2022 |
| BILI T (mg/dL) | 0.6 | 0.4 | 0.5 |
| BILI D (mg/dL) | 0.1 | 0.2 | 0 |
| BILI I (mg/dL) | 0.5 | 0.2 | 0.5 |
| AST (U/L) | 49 | 76 | 52 |
| ALT (U/L) | 44 | 140 | 58 |
| ALP (U/L) | 125 | 510 | 187 |
| ALB (g/dL) | 3.8 | 2.4 | 3.7 |
| TP (g/dL) | 7.1 | / | 6.8 |
| Parameters | July 23, 2021 | November 03, 2021 | January 26, 2022 |
| CA 19.9 (U/mL) | 60.6 | 4.6 | 3.9 |
| CEA (ng/mL) | 0.87 | / | 0.6 |
| Parameters | September 25, 2021 | October 03, 2021 | April 28, 2022 |
| Lipase (U/L) | 128 | 324 | 67 |
| Amylase (U/L) | 33 | 39 | 34 |
HGB: hemoglobin; HCT: hematocrit: NEUT: neutrophil count; PLT: platelet count; WBC: white blood cell count; BILI T: total bilirubin; BILI D: direct bilirubin; BILI I: indirect bilirubin; AST: aspartate aminotransferase; ALT: alanine aminotransferase; ALP: alkaline phosphatase; ALB: albumin; TP: total protein; CEA: carcinoembryonic antigen.
Discussion
This case agrees with the literature report. The patient is within the age range described in the literature and has two of the identified risk factors: type 2 diabetes mellitus and a history of tobacco use. The family history is not directly related.
According to literature computed tomography (CT) or magnetic resonance imaging (MRI) and endoscopic ultrasound (EUS) are sufficient to identify the tumor. In this case, we only needed a CT because of the tumor characteristics (size). Tumors found in the pancreas head are more frequent that those found in the tail. In this case, we found a body and tail giant heterogeneous lesion, septate, with a cystic appearance that does not enhance with contrast application2. This is compatible with literature as we know osteoclastic pancreatic tumors usually display a cystic component3. In our patients CT, heterogeneous changes may be compatible with necrosis or hemorrhage inside the tumor. We did not appreciate calcification zones, bile duct dilatation, or venous tumor thrombus.
Our patient experienced a maximum CA-19.9 elevation of 60.6, evidenced 2 months before surgery, and it has remained within normal parameters during follow-up. Carcinoembryonic antigen never showed any elevations. Pancreatic enzymes also did not undergo any changes, even in the immediate post-operative period. The patient did not experience an increase in bilirubin levels or other pancreatic enzymes, just a transient alkaline phosphatase elevation.
Despite there was no evidence of cancer, the surgical approach was to get R0 or resect all the lesion. Surgical findings revealed a lobulated cystic tumor measuring approximately 25 × 30 cm. It was firmly adherent to the transverse colon, posterior stomach wall, splenic vessels, superior mesenteric vein, and portal vein. The surgery was performed through a supra-infraumbilical midline incision. The posterior aspect of the pancreatic neck was dissected and transected using a stapler. The tumor capsule was dissected from the adhered organs using a harmonic scalpel, and a splenectomy was performed. The surgery was classified as a distal pancreatectomy with splenectomy.
In the brief literature research, we made to this case; we found that in 29 case report patients, two of them lose following, and only two where alive after 30 months. According to some literatures, there are only 100 case reports to 2021. Our patient keeps on following 36 months after surgery.
We consider limitations in the diagnostic approach to this patient are that we work in a public hospital with limited access to all diagnostic approach resources. Although all this, our patients evolution was as expected as she remains alive and disease-free at the time.
With this case, we aim to emphasize that diagnostic and therapeutic approach for patients with pancreatobiliary pathologies, should be conducted at a tertiary care center.
In this case, surgery was curative, the patient did not require cytotoxic treatment. She has remained disease-free for 3 years following surgery.
Undifferentiated osteoclast-like giant cell pancreatic carcinoma UC-OGC it is a very rare tumor, accounting for < 1% of all pancreatic malignancies4. Its first description was published in 1954 as an “unusual carcinoma of the pancreas”.
The onset occurs among the elderly population. There is no significant gender predisposition associated and the youngest reported case in the literature was 26 years old5. This group of pancreatic carcinomas is characterized by a lack of glandular differentiation and prominent histiocyte and osteoclast-like giant cell infiltration6. The WHO categorizes them into undifferentiated osteoclast-like giant cell, Sarcomatoid, and rhabdoid pancreatic carcinomas3 (Table 2).
Table 2 Histopathological characteristics of undifferentiated pancreatic tumors
| UCOGC | Sarcomatoid | Rhabdoid |
|---|---|---|
| Spindle-shaped cells | Spindle-shaped cells | Mimicking rhabdomyosarcoma |
| Giant osteoclast-like cells | Pleomorphic cells | Monomorphic cells |
| Mononuclear cells | Mononuclear and multi-nuclear cells | Prominent Nuclei |
| High mitotic index | Glandular formation Mimics sarcoma Osteoclast-like giant cells usually absent | Cellular and nuclear pleomorphism may be absent Rhabdoid inclusions Loss of SMARCAB1/INI1 |
UCOGC: Undifferentiated osteoclast-like giant cell pancreatic carcinoma. Modified from Mugaanyi et al.3.
Tumors with osteoclast-like giant cells have been reported within a variety of organs including skin, breast, thyroid gland, heart, lung, uterus, and pancreas6. UC-OGC is the most frequently reported subtype of undifferentiated pancreatic carcinoma. They are characterized by the presence of giant cells that resemble the giant cells of the bone; osteoclast-like giant cells. These cells are diffuse, with multiple small and uniform nuclei2. They can be pure or associated with another pancreatic neoplasm, such as intraductal papillary mucinous neoplasm, pancreatic mucinous cystic neoplasm, cystadenocarcinoma, and conventional ductal adenocarcinoma3. Patients with undifferentiated pancreatic carcinoma usually come up with generic and non-specific signs and symptoms, such as jaundice, itchy skin, weight loss, nausea, vomiting, and fever. Patients may report vague abdominal and/or back pain and gastric fullness.
In most cases of undifferentiated pancreatic carcinoma, CT, MRI, and EUS are sufficient to identify the tumor, and confirmation is made by biopsy. The tumors are more frequently located in the pancreas head and less frequently in the tail. Magnetic resonance cholangiopancreatography can better identify any dilation of the biliary tree2. On imaging work-up, UC-OGC appears larger than pancreatic ductal adenocarcinoma and generally displays a cystic component. The serological findings and tumor biomarkers in patients with undifferentiated pancreatic carcinoma are non-specific. Elevated serum levels of carcinoembryonic antigen and CA19.9 are less commonly observed than in pancreatic ductal adenocarcinoma3. The survival of UC-OGC varies from 4 months to 10 years. Shiozawa et al. who summarized the prognosis of cases published until 19977, observed only two long-term survivors in a group of 32 patients while Strobel et al. reported that 80% of the patients who underwent curative surgery survived for at least 2 years8. The ability to achieve a negative surgical margin is a cornerstone in the surgical.
Conclusion
With this case, we aim to emphasize that diagnostic and therapeutic approach for patients with pancreatobiliary pathologies, should be conducted at a tertiary care center. In this case, surgery was curative, the patient did not require cytotoxic treatment. She has remained disease-free for three years following surgery.
It is important to consolidate efforts toward establishing a standardized management approach for this condition. As it has not been possible to develop a guideline or consensus regarding treatment. We present this case to add to the existing literature on UC-OGC of the pancreas.

