











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Splenic cysts are relatively rare, as their incidence is < 0.07%; however, lately, it has increased with the application of more sensitive imaging techniques in the study of abdominal pathology. However, its diagnosis and treatment remain a difficult challenge for many physicians and surgeons due, in part, to the lack of precise guidelines for action1.
At present, splenic cysts are divided into parasitic, usually caused by Echinococcus granulosus and found in endemic areas, and non-parasitic, which can still be classified based on the presence of epithelial lining in primary cysts, which have an epithelial capsule, or secondary, which do not have a capsule2.
Secondary cysts are usually post-traumatic, due to a failure in the organization of subcapsular or parenchymal hematomas, less frequent, due to necrosis or abscesses2.
When there are symptoms, mild pain usually appears in the epigastric location or in the left hypochondrium; the presence of symptoms due to splenomegaly is rarer. To consider the surgical treatment of the splenic cyst, it is essential to take an adequate medical history, a hydatidosis serology, and imaging studies that help locate the cyst in the splenic parenchyma3.
Abdominal ultrasound is useful as an initial diagnostic examination in splenic cysts and allows a rapid diagnosis, but it is not very useful in delineating the topography of the lesion. Computed tomography (CT) shows the topography, size, probable nature, and anatomical particularities. CT and magnetic resonance imaging are the choice in diagnosis and planning of surgical strategy4.
Case report
A 33-year-old woman presented with abdominal pain of 2 weeks of evolution located in the flank and left hypochondrium, of sudden onset, continuous of an intensity of 5/10, without radiation, accompanied by nausea without vomiting, she went to the emergency department of the Regional High Specialty Hospital of Ixtapaluca, State of Mexico, Mexico. Laboratories were taken with leukocytes of 7 400, hemoglobin 14.3 g/dL, platelet 246 103/μL, absolute neutrophils 6.5 103/μL, absolute lymph 0.56 103/μL, absolute eosinophils 0.02 103/μL, absolute basophils 0.04 103/μL, absolute monocytes 0.28 103/μL. Subsequently, abdominal tomography was performed that reported a splenic complex cyst of 16.5 × 16.7 × 12.4 cm in its major axes with a volume of 1786 mL that it conditions compression and displacement of the spleen, stomach, splenic angle of the colon, pancreas, and elevation of the hemidiaphragm (Fig. 1).
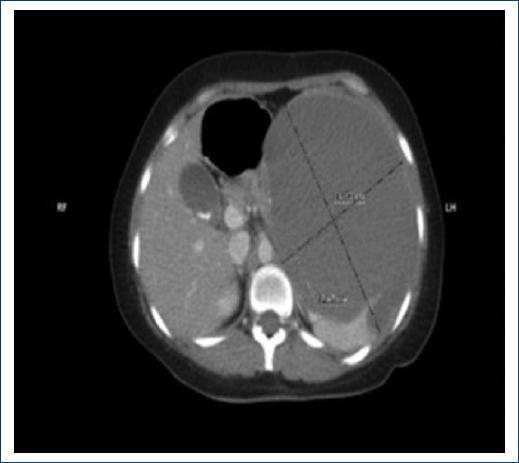
Figure 1 Presence of cystic lesion in the splenic gland with 16.5 × 16.7 × 12.4 cm in its major axes with a volume of 1786 mL.
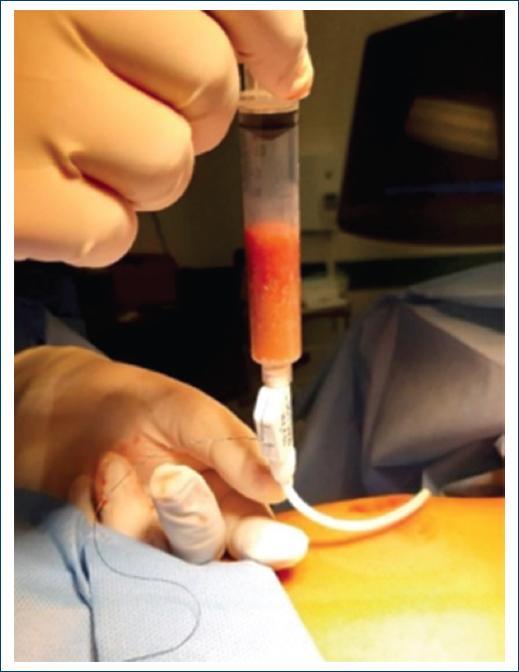
Serological study of hydatidosis was performed with a negative result. Interventional assessment was performed by imaging, which led to ultrasound-guided percutaneous drainage with 14 Fr catheter puncture, obtaining thick, ochre-colored lumpy material (1600 mL) (Fig. 2). Findings compatible with pyogenic inflammatory lesions were reported, and special histochemistry studies were reported to intentionally search for mycobacteria, fungal and parasitic microorganisms, with negative results.
Laparoscopic splenectomy was performed without complications (Fig. 3), and the patient was discharged after 5 days, with antibacterial treatment, and follow-up in 30 days, with a favorable evolution.

Discussion
Primary spleen lesions typically have their pathogenesis of the endothelial and lymphoid components developing cystic or solid lesions, among the solid lesions are mostly neoplasms, malignancies, and metastases, while within cystic lesions parasitic infection by E. granulosus is the first etiology, with non-parasitic cysts being extremely rare5.
This group of lesions can cause elevation of tumor antigens such as carcinoembryonic antigen or CA 19-9 due to their cellular origin. However, these lesions have a very low malignant potential and there are no reports in the literature of malignant true splenic cystic lesions that expand and invade other nearby organs6.
Patients usually have no specific symptoms if the cyst is small, and when the cyst is large, they have non-specific abdominal symptoms such as pain, nausea, or a palpable mass usually in the left upper quadrant7.
With the frequent use of abdominal imaging techniques such as ultrasound and CT scans, the detection of splenic cysts has increased8. Splenic cysts should be treated because of the possibility of complications such as infection, rupture, or malignancy9.
One option for some authors is total splenectomy, either open or laparoscopic, which avoids the recurrence of the lesion, however, with a high risk of developing post-operative complications such as sepsis with high mortality, and alterations in immune function, currently the trend is to offer more conservative treatment alternatives to preserve tissue, in cysts smaller than 4 cm as percutaneous drainage. Partial splenectomy, cystectomy, and marsupialization with the aim of preserving 25% of the splenic parenchyma, this being an optimal amount of tissue to preserve immune function and not increase the risk of developing complications9.
The laparoscopic approach has proven to be an effective technique for the definitive treatment of splenic cysts with minimal bleeding and recurrence with prompt recovery of the patient. It is important to perform percutaneous drainage to identify the etiologic agent and reduce the size of the splenic cyst to have a better surgical approach.
Ethical considerations
The authors declare that this case report does not contain personal information that allows the identification of the patient, so informed consent was not required; however, informed consent was obtained for the publication of this work. In addition, this case report complies with current regulations on bioethics research, and the authorization of the Institution's Ethics Committee was not required, because the patient's health was not compromised.

