











 nova página do texto(beta)
nova página do texto(beta) Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkIntroduction
Postpartum care is an essential component of women’s reproductive health1. A fundamental part of this care is provided after hospital discharge or home delivery in comprehensive health centers, and by health care providers, especially midwives2. Mothers’ perception of the quality and quantity of care they have received and their relationship with healthcare providers significantly impact continuity of care and future referrals for care3. Every woman referred to a healthcare center has the right to compassionate care, including dignity, respect for her independence and feelings, and respect for her cultural and family preferences1.
Unfair, distant, and disrespectful care during and after pregnancy has been reported worldwide in health centers4. Mothers’ satisfaction with postpartum care closely depends on how they are treated by health care professionals2. Unsatisfactory experiences and negative perceptions of health care are significant barriers to accessing care5. Some studies have examined women’s negative experiences with care during and after pregnancy6,7. Unacceptable behavior, misconduct in care management, and communication breakdown between mothers and nurses are significant challenges in antenatal care and aftercare, especially in developing countries, where high maternal mortality rates are observed8. Therefore, it is necessary to use appropriate and reliable instruments to measure any subject of study accurately9. The questionnaires available to measure mothers’ perceptions of postpartum care are designed and used to evaluate postpartum nursing care in the hospital only2,5,10, whereas most postpartum and infant care is provided in health centers. Patient-centered reproductive care has been recognized as essential in improving overall reproductive health. However, the number of studies on how to implement it is scarce11. A valid and reliable tool is needed to assess mothers’ perception of health care and encourage them to use existing care services. In addition, such a tool would help care management teams better evaluate their patients’ satisfaction and make the necessary changes to meet their needs8. It is essential to encourage women to use these services and have a reliable and valid tool to design and evaluate mothers’ perceptions of postpartum care to evaluate postpartum services in comprehensive health centers adequately. The overall purpose of this study was to create an instrument and assess its validity and reliability in determining mothers’ perceptions of postpartum health care.
Methods
Study design
This cross-sectional study was conducted in 2018 to assess the validity and reliability of the Persian version of the Mothers’ Perception of Postpartum Health Care questionnaire in comprehensive health centers in Shiraz, southwestern Iran.
Translation
The questionnaire items were initially in English. The questionnaire was translated into Persian and then translated back into English by two persons fluent in both languages. Another expert (independent of these two individuals) reviewed the translation to validate the questionnaire. Finally, two English and Persian experts compared the questionnaire and confirmed the accuracy of the translation.
Questionnaire description
This questionnaire is a part of the 100-item Goldberg Five-Factor Model12 questionnaire, which was improved based on the characteristics of the original questionnaire. The Goldberg questionnaire is valid and reliable worldwide. The satisfaction scale of this questionnaire was based on the scale designed by Hall et al.13 Although the scale was created for the elderly population, it has been modified by DiMatteo and Hays and is used to assess physician satisfaction14. Due to the nature of the items in these questionnaires and their validity15, a part of the questionnaires was selected and psychometrically designed in this study to have a valid and reliable instrument to assess mothers’ perception of the care provided in comprehensive health centers. The mothers’ perception questionnaire (MPQ) consists of 18 main items and two subscales:
1) The first section includes six questions on psychological support to mothers and the information they received from midwives, participation in decisions, feeling of freedom to talk with midwives, follow-up of problems, and obtaining sufficient maternal and neonatal care training.
2) The second section includes 12 statements on mothers’ satisfaction with the care provided, caregiver interactions, communication, behavior, and professional competence in educating patients about anxiety management.
Validity
The validity of the MPQ was evaluated by assessing face validity, content validity, and construct validity (exploratory factor analysis). Quantitative and qualitative methods were used to determine the face validity of the MPQ. To assess the face validity of the Persian version of the MPQ using the qualitative approach, we initially selected some employees of the sampled health centers and mothers attending these centers (n = 10) to comment on the questionnaire. Their opinions on the appropriateness and clarity of the items were applied to the questionnaire items. It is essential to consider the judgment of the target group on the relevance and comprehensiveness of the questionnaire items and that these items should assess the areas critical to the target group16. The impact score was used to determine quantitative face validity. Comprehensive health center staff and reproductive health professionals (n = 10) evaluated the importance of each item using the following formula:
Impact score = frequency (%) × importance
A coefficient of 1.5 or more was acceptable13. At this stage, the importance of each item was measured using the 5-point Likert scale: fairly important (5 points), somewhat important (4 points), moderately important (3 points), slightly important (2 points), and not at all important (1 point). Items with an effect size of < 1.5 points were modified. In addition to the opinion of several staff members working in comprehensive health centers, the opinions of literature experts on the wording, phrasing, and appearance of the questionnaire items were used.
A quantitative method was used to determine the content validity of the MPQ. For this purpose, the opinions of some faculty members who specialized in maternal care and reproductive health (10 individuals) were used. We performed a content validity index (CVI) based on that of Waltz and Strickland17. This index evaluates the relevance, clarity, and simplicity of the questions in the questionnaire on a four-point Likert scale.
The CVI score for each sentence was calculated by dividing the number of experts who agreed with rankings 3 and 4 by the total number of experts. CVI greater than 0.79 was considered adequate16. Exploratory factor analysis (EFA) was used to determine to construct validity. A total of 250 women referred to comprehensive health centers after childbirth were selected by purposive sampling. The results were analyzed using SPSS version 22.0 software.
Reliability
Reliability shows the reproducibility and accuracy of the instrument14. The reliability of the Persian version of the MPQ was calculated by determining Cronbach’s alpha (internal consistency) of the entire questionnaire and its sub-items.
Results
Demographic characteristics
After referral to comprehensive health centers, 250 women participated in this study. The mean age was 30 ± 5.54 years, and most were homemakers (90.4%, 226). Most participants had planned their pregnancy (86%, 215 individuals) and used comprehensive health services during and after pregnancy. Table 1 shows the demographic characteristics of the participants.
Table 1 Demographic and characteristics of the study participants
| Variable | Characteristic | Frequency (n) | Percentage (%) |
|---|---|---|---|
| Age | Minimum 18 years old | 3 | 1.2 |
| Maximum 46 years old | 2 | 0.8 | |
| Occupation | Housewife | 226 | 90.4 |
| Government employee | 23 | 9.2 | |
| Worker | 1 | 0.4 | |
| Spouse occupation | Self-employed | 129 | 65.9 |
| Government employee | 57 | 22.8 | |
| Laborer | 29 | 11.6 | |
| Education | Illiterate | 4 | 1.6 |
| Up to high school | 62 | 24.8 | |
| Bachelor’s degree | 175 | 70 | |
| Masters or above | 9 | 30.6 | |
| Spouse education | Illiterate | 5 | 2 |
| Up to high school | 62 | 24.8 | |
| Bachelor’s degree | 167 | 66.8 | |
| Masters or above | 16 | 6.4 | |
| Pregnancy | Planned | 215 | 86 |
| Unplanned | 34 | 13.6 | |
| Delivery method | Normal delivery | 111 | 44.4 |
| Cesarean section | 138 | 55.2 | |
| Assisted | 1 | 4 | |
| Type of gestation | Single | 246 | 98.4 |
| Twins | 4 | 1.6 | |
| Weeks of gestation | < 37 weeks | 41 | 16.4 |
| > 37 weeks | 209 | 83.6 | |
| Delivery location | Health center | 148 | 59.2 |
| Gynecologist clinic | 98 | 39.2 | |
| Others | 4 | 1.6 | |
| Center for health care post delivery | Health center | 201 | 80.4 |
| Gynecologist | 43 | 17.2 | |
| Others | 24 | 6 |
Face and content validity
The impact coefficient of all the items was higher than 1.5, and the questionnaire presented adequate and acceptable face validity. The minimum CVI value accepted was 0.79, which was higher than all the items in this questionnaire. The results showed that the CVI of all the items was 0.8-0.9, with a scale level index (S-CVI) of 0.73. The questionnaire items had an S-CVI of 0.73, and the content validity ratio (CVR) ranged from 0.62 to 0.9. The CVR value of the two items was < 0.62, so these items were modified and reevaluated. After revising the CVR values, they reached an acceptable level. To refine the writing and wording of each sentence, a literary expert edited the items.
Construct validity
EFA was performed with 250 completed questionnaires. The Kaiser-Meyer-Olkin (KMO) index value at the first output was 0.825. Both the positive and negative skewness of the data were within an acceptable range. Therefore, the sample size selected was sufficient for factor analysis. According to Bartlett’s test, the factor analysis was significant in identifying the structure of the factor model at p < 0.001, indicating detectable relationships among the variables analyzed.
The second EFA output, consisting of two parts, the initial eigenvalue and the extraction sums of squared or rotation loadings, are listed in table 2. The rotational correlation matrix showed that 18 items related to maternal perception of postpartum care measured two main factors. The first factor consisted of six items whose factor loadings ranged from a minimum of 0.254 to a maximum of 0.698. The second factor consisted of 12 items that were investigated in three dimensions. The first dimension consisted of seven items with a loading factor ranging from 0.626 to 0.732. The second dimension consisted of three items with a minimum operational load of 0.612 and a maximum of 0.675. Lastly, the third dimension consisted of two items with a minimum operational loading of 0.532 and a maximum of 0.637. Figure 1 describes the factor analysis to determine the correlation between items. The first factor had six items, one of which had a weak correlation coefficient concerning the other items, and its reliability was low; thus, the item was eliminated, and Cronbach’s alpha reliability coefficient increased from 0.717 to 0.84. Other items with sufficient correlation coefficients for the final 17-question model are listed in table 3. The estimate of all factor loadings was significant. The internal consistency coefficient was used to determine the internal validity of the questionnaire.
Table 2 Primary and extractive sharing of exploratory factor analysis of mothers’ perceptions of postpartum care
| Total variance explained | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Component | Initial eigenvalues | Extraction sums of squared loadings | Rotation sums of squared loadings | ||||||
| Total | Percentage of variance (%) | Cumulative (%) | Total | Percentage of variance (%) | Cumulative (%) | Total | Percentage of variance (%) | Cumulative (%) | |
| < 1 | 5.174 | 28.747 | 28.747 | 5.174 | 28.747 | 28.747 | 3.643 | 20.237 | 20.237 |
| 2 | 1.981 | 11.006 | 39.753 | 1.981 | 11.006 | 39.753 | 3.202 | 17.791 | 38.028 |
| 3 | 1.910 | 10.614 | 50.367 | 1.910 | 10.614 | 50.367 | 2.166 | 12.032 | 50.060 |
| 4 | 1.112 | 6.176 | 56.543 | 1.112 | 6.176 | 56.543 | 1.167 | 6.482 | 56.543 |
| 5 | 0.983 | 5.462 | 62.005 | ||||||
| 6 | 0.930 | 5.167 | 67.172 | ||||||
| 7 | 0.891 | 4.952 | 72.124 | ||||||
| 8 | 0.775 | 4.308 | 76.432 | ||||||
| 9 | 0.672 | 3.736 | 80.168 | ||||||
| 10 | 0.567 | 3.149 | 83.317 | ||||||
| 11 | 0.527 | 2.929 | 86.246 | ||||||
| 12 | 0.465 | 2.585 | 88.831 | ||||||
| 13 | 0.427 | 2.371 | 91.203 | ||||||
| 14 | 0.404 | 2.245 | 93.447 | ||||||
| 15 | 0.396 | 2.200 | 95.648 | ||||||
| 16 | 0.322 | 1.788 | 97.436 | ||||||
| 17 | 0.256 | 1.424 | 98.860 | ||||||
| 18 | 0.205 | 1.140 | 100.000 | ||||||
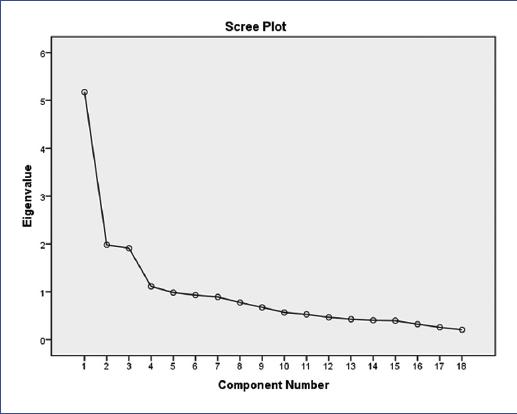
Table 3 Rotated matrix factor analysis of components of mothers’ perception
| Maternal perception questionnaire in the postpartum period | Load factor |
|---|---|
| Factor one: Mothers’ perception in post-delivery by midwives’ period | |
| 1. Did you get enough psychological support ? | 0.824 |
| 2. Did you receive the necessary information from the staff? | 0.883 |
| 3. Did you participate in meetings and communicating with your midwife? | 0.812 |
| 4. Did you feel comfortable talking to your midwife about your problems? | 0.805 |
| 5. Have you received enough education about caring for yourself and your baby after delivery? | 0.578 |
| Factor two: Understanding postpartum care | |
| First dimension: Positive understanding of care | |
| 6. I am completely satisfied with the care received | 0.68 |
| 7. The time spent with the health staff was adequate | 0.626 |
| 8. The health staff thoroughly and reasonably explained all the care, medications, and work they did for me | 0.634 |
| 9. The health workers listened carefully to what I was saying | 0.708 |
| 10. Health workers provided care for me with the utmost respect | 0.732 |
| 11. The health workers were kind and attentive to my feelings | 0.628 |
| 12. The health care that I received eliminated all the uncertainty and worry | 0.798 |
| Second dimension: Negative perception of care | |
| 13. I think the time spent with the health staff was not adequate | 0.675 |
| 14. I had some doubts about the ability of the health workers | 0.66 |
| 15. I feel that in some aspects, the health workers were not paying enough attention to me | 0.612 |
| Third dimension: | |
| 16. There were some areas in the care I received that could have been better | 0.842 |
| 17. I noticed some healthcare staff were arrogant | 0.533 |
Reliability
Cronbach’s alpha values for each item and the entire questionnaire after factor analysis are presented in table 4. The intraclass correlation coefficient (ICC) was 0.688, confirming divergent validity. The cross-correlations of the structures were lower than the mean square of the variances extracted, indicating a divergent validity model. The results showed sufficient reliability of the questionnaire (Table 4).
Table 4 Correlation, validity, and homogeneity of perceptions
| Variables | Cronbach’s alpha | Intraclass correlation | 95% CI | Questions (n) |
|---|---|---|---|---|
| Factor one | 0.690 | 0.680 | 0.614-0.738 | 5 |
| Factor two | ||||
| First dimension | 0.740 | 0.737 | 0.684-0.784 | 7 |
| Second dimension | 0.758 | 0.757 | 0.699-0.805 | 3 |
| Third dimension | 0.162 | 0.144 | 0.098-0.332 | 2 |
95% CI: 95% confidence interval.
Discussion
In this study, we evaluated the psychometric properties of mothers’ perception of postpartum care in comprehensive health centers in Iran. The validity and reliability of each questionnaire instrument ensured its accuracy and precision. Based on the findings of this study, the MPQ has adequate face, content, and construct validity. The factor loading of all questionnaire items was significant at α = 0.05. Since this questionnaire was designed and validated for the first time, no similar study was found. All other published studies have assessed satisfaction, perception, or misconduct of postpartum care in hospitals. All items in this questionnaire have an impact coefficient over 1.5, CVI over 0.79, and the questionnaire has face and content validity.
The study by Taavoni et al. aimed to design and test a Respectful Maternity Care Questionnaire. The results of their research showed that all items had an impact coefficient over 1.5 and that the CVR of the questionnaire was 0.74, which was acceptable6. Their results were similar to those of the present study. The CVI, CVR, and S-CVR were all acceptable items for the MPQ. Another study by Sheferaw et al. in Ethiopia to validate a 15-item questionnaire assessing mothers’ perception of respectful antenatal care in health centers showed that the questionnaire items had a construct validity of 0.76 to 0.82, and the entire questionnaire had acceptable construct validity. The findings of this study confirmed the structural validity of the two factors of perception of postpartum midwifery care and postpartum care11. In addition, the study published by Afulani et al. aimed to develop a person-based maternal care assessment tool. This questionnaire has four factors and 38 items. The results of the EFA confirmed the validity of 30 items in three factors for urban and rural communities18.
Confirmatory factor analysis of the study by Taavoni et al. revealed that the Respectful Maternity Care Questionnaire related to mothers’ satisfaction with postpartum nursing care had a good relationship between items and an acceptable value6. This research is similar to the present one, but as the questionnaire is already available in some languages, including English, and has been validated, confirmatory factor analysis was used. Cronbach’s alpha for the questionnaire is 0.668, and the internal consistency and reliability of this questionnaire are adequate and demonstrate its high reliability. In the study by Afulani et al., Cronbach’s alpha was 0.8, and all factors had a good value for reliability and applicability18. Overall, the modified 12 main items and two subitems questionnaire of mothers’ perception of postpartum care in comprehensive health centers is a valid and reliable questionnaire to measure mothers’ perceptions of these vital and valuable services.
This questionnaire can identify strengths and weaknesses in the care provided by midwives and health care providers. Many studies on maternal satisfaction, maternal perception, and malnutrition in prenatal or postnatal care have been conducted in different hospitals around the world, leading to the development of reliable and valid tools, especially in developing countries where health care is poorer. The development of these tools has conducted to the design or confirmation of their validity and reliability8,10, providing essential inputs to care teams and healthcare providers.
Relevance to clinical practice
This study was designed to prepare a unique tool to assess the maternal perception of the care provided at comprehensive outpatient health centers. The limited number of factors and the total number of items in this questionnaire, considering the little time mothers spend in health centers, would allow participants to concentrate and avoid fatigue while answering the questions. The low number of sub-items (two factors) may cause some aspects mothers need to understand for better continuity of care to go unnoticed. Moreover, according to our review, this questionnaire has been designed for the first time. However, considering other aspects that may not have been well addressed in this tool, if validated in other countries, it can be used as a universal tool to investigate possible harmful effects on maternal perception of postpartum care.

