Artículos
Family planning as a solution for climate change. Bioethical dilemmas in the context of sustainable development


-
Publication dates-
September 10, 2024
Jul-Sep , 2024
- Article in PDF
- Article in XML
- Automatic translation
- Send this article by e-mail
- Share this article +
Abstract
Climate change crisis is a global concern for the humanity and for achieving Sustainable Development Goals (SDG). One of the solutions proposed is family planning which plays a dual role. Firstly, family planning must ensure gender equality (SDG 5) and good health (SDG 3) that “strengthen resilience and adaptive capacity to climate-related hazards and natural disasters in all countries” (SDG 13.1). Secondly, it would make it possible to contribute to the reduction in population growth, which will turn lead to a reduction in the levels of greenhouse gas emissions. This article analyzes this dual role to determine whether family planning could be an ethical solution for climate change and for contributing to sustainable development for a better future of humanity.
Keywords::
family planning, climate change, gender equality, public health
1. Introduction
Family planning, as part of Sexual & Reproductive Health & Rights (SRHR) (1), and climate change are both of the 17 Sustainable development goals1 (SDG 3, 5 and 13) (2). Family planning refers to two main methods. On the one hand, it includes Modern contraception2 to avoid unintended pregnancy and infectious diseases, to choose the spacing of children (whether, when, what means and how many to have) and to increase educational and economic benefits (spacing children gives women the opportunity to continue higher studies and to be engaged in the market). On the other hand, family planning includes the possibility to end an abortion with all the medical attention to avoid unsafe ones.
-
(1)Defining sexual health, 2002
-
(2)Transforming our world: the 2030 Agenda for Sustainable Development. Resolution adopted by the General Assembly, 2015
In addition, the Intergovernmental Panel on Climate Change (IPCC), the United Nations Framework Convention on Climate Change (UNFCCC) and the Conference of the Parties (COP) do not mention family planning as a method to fight climate change. However, one of the cross-chapter of the IPCC 2022’s report, based on Gender’s study, suggested that “increased access to reproductive health and family planning services, […] contributes to climate change resilience and socioeconomic development through improved health and well-being of women and their children” (3, p. 2702). In the same context, some organizations claim that family planning must be a condition, or rather a solution for fighting the climate crisis. This is the case, for example, of one of the reports of who. The authors conclude by calling to increase family planning services in developing countries (4). The same applies to the International Planned Parenthood Federation (IPPF), supported by the United Nations. IPPF claims that family planning is necessary to reduce population growth and to facilitate climate adaptation and resilience (5,6). As for the NGO Project Drawdown, founded by Paul Hawken and led by more than 200 researchers, it presents family planning as one of the 93 different climate solutions (7). It is also the case of the United Nations Fund for Population (UNFPA) claiming that family planning, as part of SRHR, is “essential and a matter of human rights” for women and girls during climate crisis (8, p. 92), which echoes the SDG 13.1.
-
(3, p. 2702)Climate Change 2022: Impacts, Adaptation and Vulnerability, 2022
-
(4)Climate change and family planning: least-developed countries define the agendaBull World Health Organ, 2009
-
(5Population & Sustainability Network. Climate change: “Time to Think Family Planning”, 2016
-
6)The climate crisis and sexual and reproductive health and rights, 2021
-
(7)Project Drawdown, 2020
-
(8, p. 92)The State of World Population 2015: Shelter from the storm - A transformative agenda for women and girls in a crisis-prone world, 2015
In this context, it is pertinent to ask these two main questions: does fighting against climate change and global warming justify the use of family planning as a solution to strengthen women’s sexual and maternal health [1] and as a solution to environmental pollution [2]? What are the bioethical dilemmas [3] that arise from such proposition of a solution? To the respond to these questions, three categories of bibliographical sources form the basis of this reflection. First of all, there are certain UN texts and related studies. Then there is the extensive scientific literature, articles and books, on medical and environmental studies. Finally, the bioethical approach is based on Elio Sgreccia’s personalist model.
2. Strengthening women’s sexual and maternal health
According to the United Nations Human Rights Special Procedures’ report, climate change represents a challenge for the enjoyment of human rights. It is about the right to life, the right to health, the right to food, the right to water and sanitation, the rights of the child and the right to a healthy environment (9, pp. 17-23). As a result, three potential impacts of climate change on SRHR can be identified in the context of SDGs: access de sexual reproductive health services [1.1], inequalities, sexual and gender-based violence [1.2] and maternal health [1.3]. Nonetheless, several factors play a fundamental role in these impacts.
-
(9, pp. 17-23)Safe Climate. A Report of the Special Rapporteur on Human Rights and the Environment, 2019
2.1. Access to sexual reproductive health services
The access to sexual reproductive health services is a double target in SDGs 3.7 and 5.6. it can be threatened by climate change [1.1.1] and, also by medical and socio-cultural reasons [1.1.2].
2.1.1. Climate change as factor
On the one hand, some authors argue climate change threatens this access on two levels.
-
As indicated by O. Leyser-Whalen et al. (10) and by the Human Rights Council (11, §13), extreme weather events, due to climate change, can destroy infrastructure of family planning services. Thus, this leads to a reduction of the quality, the accessibility and the availability.
-
S. Barot, from the Guttmacher Institute, notes that during climate crisis, Sexual and Reproductive Health Needs of Women in Humanitarian Situations are unmet. In effect, destructed sexual reproductive health’s infrastructures are under-prioritized and unfunded compared to other infrastructures. Even it exists, in such conditions, a reproductive health kits containing supplies, contraceptives and equipment, the service delivery faces some serious gaps such as cultural norms, lack of security’s and logistical research and financial barriers (12).
-
(10)Another disaster: Access to abortion after Hurricane HarveyHealth Care Women Int, 2020
-
(11, §13)Analytical study on gender-responsive climate action for the full and effective enjoyment of the rights of women, 2019
-
(12)In a State of Crisis: Meeting the Sexual and Reproductive Health Needs of Women in Humanitarian SituationsGuttmacher Policy Rev, 2017
2.1.2. Medical and socio-structural factors
On the other hand, it would be a huge error to limit the lack of accessing the SRHR services only on the climate change crisis for two reasons.
-
It is a fact that in some countries where there are no climate disasters, girls and women still have difficulties to access sexual reproductive health services. It is the case, for example, of Malta and Poland concerning abortion, or the case of Iceland, Switzerland, Czech Republic, Greece, etc. concerning contraception as revealed by the Contraception Policy Atlas Europe (13).
-
A lot of women would not or could not access to these services for many reasons such as the contraception failure due to the age, or economic and medical factors as indicated by S. E. K. Bradley et al.(14), or socio-economic reasons as indicated by J. Sachs (15, pp. 188-189).
-
(13)Contraception Policy Atlas 2023, 2023
-
(14)Global Contraceptive Failure Rates: Who Is Most at Risk?Stud Fam Plann, 2019
-
(15, pp. 188-189)Common Wealth. Economics for a Crowded Planet, 2009
2.2. Inequalities, sexual and gender-based violence
SDG targets 3.3, 5.2, 5.3, 8.5 and 10.2 aim to protect women against violence and gender inequality. These inequalities and violence may be increased during climate change events [1.2.1], but they are also perpetrated by political and socio-structural factors [1.2.2].
2.2.1. Climate change as a factor
The Human Rights Council affirms that climate change is a challenge for the advancement of gender equality since women and girls are at higher risk during crisis such as weather events (11, § 5, 17 and 54).
-
(11, § 5, 17 and 54)Analytical study on gender-responsive climate action for the full and effective enjoyment of the rights of women, 2019
Indeed, A. M. Thurston et al. demonstrated that sexual assault and violence against women and girls increase during and after disasters (84 % climate related) (16)severity and duration worldwide. Disasters disproportionately impact women and girls, with some evidence suggesting that violence against women and girls (VAWG. In the same context C. Rousseau affirms that since climate disasters can lead to “disruption the daily life” (losing job and home), women and young girls may engage unprotected sex for pay or food to insure their survival (17). These events and the lack of accessing family planning lead to unintended pregnancies causing maternal and child health issues that “hampers national economic development” (5, pp. 5-6). In addition, these unintended pregnancies and their complications can widen the gender inequality gap by limiting access to social, economic and political life opportunities (6, p. 9).
-
(16)Natural hazards, disasters and violence against women and girls: a global mixed-methods systematic reviewBMJ Glob Health, 2021
-
(17)Climate change and sexual and reproductive health: what implications for future research?Sex Reprod Health Matters, 2023
-
(5, pp. 5-6)Population & Sustainability Network. Climate change: “Time to Think Family Planning”, 2016
-
(6, p. 9)The climate crisis and sexual and reproductive health and rights, 2021
2.2.2. Political and socio-structural factors
However, inequalities, sexual and gender-based violence are not just a climate change issue. Less economic opportunities are due to social and political systems regarding maternity. It is the case of France.3 Despite the easy access to family planning services (18, p. 25), the pay gap between men and women persists, even though it has narrowed (19, p. 4) between 2000 (18.6 %) and 2019 (16.1 %). Some authors argue that this inequality is a consequence of maternity (20; 21, pp. 125-130). Nevertheless, despite the efforts made for realization of gender economic and gender equalities (SDGs 8.5 and 10.2), such as economic aid through maternity leave and maternity allowance, the gap always exists due to various factors, such as the work sector, positions of responsibility, discrimination at the time of hiring or in terms of bonuses.
-
(18, p. 25)Sustainable Development Report 2023. Implementing the SDG Stimulus, 2023
-
(19, p. 4)Vers l’égalité réelle entre les femmes et les hommes. Chiffres-clés, 2022
-
(20Femmes et hommes sur le marché du travail : des écarts moins marqués en début de vie active, 2019
-
21, pp. 125-130)Égalité professionnelle entre les femmes et les hommes en France : une lente convergence freinée par les maternitésEcon Stat Econ Stat, 2019
In addition, sexual and gender-based violence, to be banned according to SDGs 5.2 and 5.3, is not fundamentally, but occasionally, a climate change problem. Such violence takes many forms, and legal authorities sometimes perpetrate it. Several categories of women and girls are subjected to sexual violence, such as coercive contraception and sterilization. It is the case of HIV positive women especially in Africa (22- 24) and women with mental disabilities in United States (25) and in European Union (26) as noted by the United Nations (27, § 29). It is also the case of women belonging to ethnic minorities (indigenous peoples) such as the Romani in Slovakia (28,29) or to different ethnic groups such as the Ethiopians in Israel (30- 33) between 2004 and 2005. In addition, it was also the case of women with social problems, such as drug addicts, in the United States, mainly in California, Nebraska and Texas (34,35), between 1991 and 1993.
-
(22-The Price of Failure of Informed Consent Law: Coercive Sterilizations of HIV-Positive Women in South AfricaLaw Inequal, 2014
-
24)Government of the Republic of Namibia v LM and Others, 2014
-
(25)Female Sterilization and Cognitive Disability in the United States, 2011-2015Obstet Gynecol, 2018
-
(26)Forced sterilization of persons with disabilities in the European Union, 2022
-
(27, § 29)Santé et droits des filles et des jeunes femmes handicapées en matière de sexualité et de procréation, 2017
-
(28ECHR. N.B. v. Slovakia. No. 29518/10,
-
29)ECHR. V.C v. Slovakia. No. 18968/07, 2011
-
(30-Why Is the Birth Rate in Israel’s Ethiopian Community Declining?Haaretz, 2012
-
33)Israel Admits Ethiopian Women Were Given Birth Control ShotsHaaretz, 2013
-
(34Implanted Birth Control Device Renews Debate Over Forced ContraceptionThe New York Times, 1991
-
35)The constitutionality of the use of the Norplant contraceptive device as a condition of probationHastings Const Law Q, 1992
2.3. Maternal health
Maternal health is a main target of SDGs 3.1, 3.2 and 3.7. If climate change has a role in this domain [1.3.1], it is also important to look into the medical aspect in which several consequences and risks resulting from family planning methods affect the woman’s health. [1.3.2].
2.3.1. Climate change as a factor
The IPPF argues that climate change has an important impact on maternal health (6, p. 8). Indeed, lack of access to clean and potable water may affect the woman’s health during pregnancy, childbirth and even “the administration of certain contraceptive methods” (6, p. 8). As confirmed by IPCC, clean and safe water is important to strengthen the climate resiliency human health (3, p. 22) especially that “changes in temperature, precipitation and water-related disasters are linked to increased incidences of waterborne diseases” (3, p. 50).
-
(6, p. 8)The climate crisis and sexual and reproductive health and rights, 2021
-
(6, p. 8)The climate crisis and sexual and reproductive health and rights, 2021
-
(3, p. 22)Climate Change 2022: Impacts, Adaptation and Vulnerability, 2022
-
(3, p. 50)Climate Change 2022: Impacts, Adaptation and Vulnerability, 2022
In addition, P. Poursafa et al. affirm that hot or cold weather could lead to many health issues such eclampsia, preeclampsia, 4 cataract, low birth weight, pulmonary tuberculosis, hypertension, sex ratio and length of pregnancy (36, p. 398). Many other studies describe other issues such gestational diabetes (37), threatened/spontaneous abortion, renal diseases, infectious diseases (38), preterm birth and feral growth lag (39).
-
(36, p. 398)Systematic review on adverse birth outcomes of climate changeJ Res Med Sci Off J Isfahan Univ Med Sci, 2015
-
(37)Climate factors and gestational diabetes mellitus risk - a systematic reviewEnviron Health, 2020
-
(38)Ambient extreme heat exposure in summer and transitional months and emergency department visits and hospital admissions due to pregnancy complicationsSci Total Environ, 2021
-
(39)Anticipated impacts of climate change on women’s health: A background primerInt J Gynecol Obstet, 2023
Moreover, the Human Rights Council specifies that climate change can affect the mental health of women such as stress-related disorders and depression (11, § 9 and 12).
-
(11, § 9 and 12)Analytical study on gender-responsive climate action for the full and effective enjoyment of the rights of women, 2019
In this context, to reinforce pregnant women’s ability to adapt to climate change and to avoid/reduce all these health issues, using voluntary spacing children through modern contraceptives or through safe abortion in case of unintended pregnancy is encouraged by family planning’s programs (6, p. 9).
-
(6, p. 9)The climate crisis and sexual and reproductive health and rights, 2021
2.3.2. Medical factors
However, the impact on maternal health cannot be approached solely from this point of view, in which climate change is a major factor in health problems. It is also important to look at this subject from the opposite angle. Numerous scientific studies have highlighted the possible risks, consequences and side effects of family planning, particularly some modern contraceptive methods and abortion, on maternal health.
On the one hand, hormonal contraception can lead to many health consequences and risks such as eclampsia, preeclampsia, hypertension, threatened/spontaneous abortion, preterm birth and fetal growth lag, gestational diabetes (40, pp. 105-111), breast (41)but information on associated risks is limited. We aimed to assess breast cancer risk associated with current or recent use of different types of hormonal contraceptives in premenopausal women, with particular emphasis on progestagen-only preparations. Methods and findings Hormonal contraceptive prescriptions recorded prospectively in a UK primary care database (Clinical Practice Research Datalink [CPRD], uterus cervix and liver’s cancer (42, pp. 283-293, 295-296), liver issues (40; 43, pp. 158-169). The thromboembolic diseases (44) is also frequent and can lead to the death: in the United States, for example, between 136 and 260 young and healthy women dies venous thrombosis because of hormonal contraceptive use (45). In addition, hormonal contraception can lead to autoimmune diseases (46,47), psychological and psychoneuroendocrinological problems such as depression and post-partum depression (48), memory alteration (49- 53) and sexual behavioral changes due to brain malfunction (54, pp. 102-144; 55). As for the copper IUD, it may contribute to anemia, pelvic inflammatory, miscarriage (56, p. 156) and pregnancies with IUD (57).
-
(40, pp. 105-111)Pilule ou pas pilule ? - Tout savoir sur les différents moyens de contraception y compris masculins, 2022
-
(41)Combined and progestagen-only hormonal contraceptives and breast cancer risk: A UK nested case-control study and meta-analysisPLOS Med, 2023
-
(42, pp. 283-293, 295-296)Pharmaceuticals. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, 2012
-
(40Pilule ou pas pilule ? - Tout savoir sur les différents moyens de contraception y compris masculins, 2022
-
43, pp. 158-169)The effect of multivitamin supplements on continuation rate and side effects of combined oral contraceptives: A randomised controlled trialEur J Contracept Reprod Health Care, 2015
-
(44)Thrombotic Stroke and Myocardial Infarction with Hormonal ContraceptionN Engl J Med, 2012
-
(45)Systematic Review of Hormonal Contraception and Risk of Venous ThrombosisLinacre Q, 2018
-
(46Women and Autoimmune DiseasesEmerg Infect Dis, 2004
-
47)Combined oral contraceptive use and the risk of systemic lupus erythematosusArthritis Care Res, 2009
-
(48)Depression Associated With Hormonal Contraceptive Use as a Risk Indicator for Postpartum DepressionJAMA Psychiatry, 2023
-
(49-Hormonal contraception usage is associated with altered memory for an emotional storyNeurobiol Learn Mem, 2011
-
53)Hormonal contraceptives, menstrual cycle and brain response to facesSoc Cogn Affect Neurosci, 2014
-
(54, pp. 102-144This Is Your Brain on Birth Control: The Surprising Science of Women, Hormones, and the Law of Unintended Consequences, 2019
-
55)Hormonal contraception and sexual desire: A questionnaire-based study of young Swedish womenEur J Contracept Reprod Health Care, 2016
-
(56, p. 156)Family Planning: A Global Handbook for Providers. Evidence-based guidance developed through worldwide collaboration, 2022
-
(57)The prognosis of pregnancy conceived despite the presence of an intrauterine device (IUD)J Perinat Med, 2010
On the other hand, even if this fact is ignored, concealed or taken lightly, safe abortion can have short-or long-term consequences and risks for a woman's health. Surgical abortion may cause bleeding or hemorrhaging, damage to pelvic vessels, bowel, bladder, fallopian tubes and ovaries (58). As for medical abortion (pill), it can cause cramping and severe vaginal bleeding with abortion failure, necessitating surgical intervention (59- 61), placenta accreta (62), hypotension, sinus tachycardia, myocardial infarction, cervical laceration, uterine rupture, uterine infection (63). As for psychological risks, induced abortions can cause anxiety or depression (64,65), suicidal thoughts and posttraumatic stress reactions (66). After Covid-19, abortion by telemedicine has been developed in many countries, such in the United States and in France. This type of abortion has many consequences on maternal and fetal health due to the lack of pre-abortion care (physical examination, ultrasound, checking on medical history screening for genital tract infections, checking for ectopic pregnancy). As a result, several consequences occur such as uterine rupture (67,68), abortion failure and intrauterine fetal demise causing maternal health complications (69).
-
(58)Public Health Impact of Legal Termination of Pregnancy in the US: 40 Years LaterScientifica, 2012
-
(59-First-trimester medical abortion with mifepristone 200 mg and misoprostol: a systematic reviewContraception, 2013
-
61)Immediate adverse events after second trimester medical termination of pregnancy: results of a nationwide registry studyHum Reprod, 2011
-
(62)Subsequent placenta accreta after previous mifepristone-induced abortion: A case reportWorld J Clin Cases, 2021
-
(63)Misoprostol, 2022
-
(64The effects of induced abortion on emotional experiences and relationships: A critical review of the literatureClin Psychol Rev, 2003
-
65)Global prevalence of post-abortion depression: systematic review and Meta-analysisBMC Psychiatry, 2023
-
(66)Induced abortion and traumatic stress: a preliminary comParíson of American and Russian womenMed Sci Monit, 2004
-
(67Chemical Abortion: Risks Posed by Changes in SupervisionJ Am Physicians Surg, 2022
-
68)Silent Uterine Rupture with the Use of Misoprostol for Second Trimester Termination of Pregnancy: A Case ReportObstet Gynecol Int, 2011
-
(69)Intrauterine Fetal DemiseStatPearls, 2023
This overview shows that climate change is just one of many factors that can have an impact on women’s sexual and maternal health. Over and above that, family planning methods promoted to avoid the consequences and risks of the impact of climate change may themselves be the cause of those same consequences and risks which is paradoxical for a solution to a problem.
3. Reducing environmental pollution
One of the reasons of climate change is the high level of Greenhouse gases (GHGs) emission, mainly the carbon dioxide (CO2).5 Some authors argue that population growth is responsible for the big amount of these emissions and family planning would be a solution [2.1]. Other studies show that some of family planning methods are a factor of environmental pollution and GHGs emissions [2.2].
3.1. Greenhouse gases emissions and population growth
As the IPPF suggests, family planning is a solution to reduce the GHGs in the atmosphere. Thus, Project Drawdown researchers established a scenario in which family planning, between 2020 and 2050, could reduce the CO2 emissions by 69.90 gigatones (Gt). The estimate that 55 % of this amount (37.9 gt) would be in low- and middle-income countries and 45 % (31 gt) in high-income countries. In this case, some authors suggest that by reducing population growth through family planning, it is possible to reduce GHGs emissions [2.1.1]. However, some studies show that such relation is not accurate [2.1.2].
3.1.1. Family planning and reducing population
B.C. O’Neill et al. assert that “policies that slow population growth would probably also have climate-related benefits” (70); J. Bongaarts and R. Sitruk-ware affirm that “slower future population growth could reduce emissions globally by an estimated 40% or more in the long term” (71, p. 233). R. N. Proctor and L. Schiebinger sustain the idea that “if the world’s total population were eventually reduced by 10 percent, this would reduce carbon emissions by 3.6 billion tons per year, which is more than the total combined emissions of Germany, Japan, Brazil, Turkey, Mexico, and Australia” (72). For some others, banning abortion would lead to a surplus of unwanted children. It is the case of T. Joyce et al who affirm, already in 2012 before overturning Roe v. Wade (June 24, 2022), that “abortion rates would fall “If Roe v. Wade were overturned] abortion rates would fall by 14.9 percent” in the United State, which leads to arising the unintended births to “178,804 additional births or 4.2 percent of the national total” (73, pp. 4 and 22).
-
(70)Demographic change and carbon dioxide emissionsThe Lancet, 2012
-
(71, p. 233)Climate change and contraceptionBMJ Sex Reprod Health, 2019
-
(72)How Preventing Unwanted Pregnancies Can Help on ClimateYale E360, 2022
-
(73, pp. 4 and 22)Back to the Future? Abortion Before & After RoeNational Bureau of Economic Research, 2012
3.1.2. Paradoxical data
However, two points must be taken into consideration. First of all, if banning abortion would lead to a surplus of unwanted children due to unintended pregnancies, two studies of J. Bearak et al. and a report of the Guttmacher Institute show that “unintended pregnancy and abortion occur worldwide, both where abortion is broadly legal and where it is restricted” (74- 76). Between 2015 and 2019, unintended pregnancy rate was 59 % and abortion rate was 41 % in countries where abortion was broadly legal. In countries where there are some restrictions for abortion, unintended pregnancy rate was between 70 and 79 %, and abortion rate was between 36 and 39 %. This means that there will be always unwanted children even abortion is legal.
-
(74-Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990-2019Lancet Glob Health, 2020
-
76)Unintended Pregnancy and Abortion WorldwideGuttmacher Institute, 2020
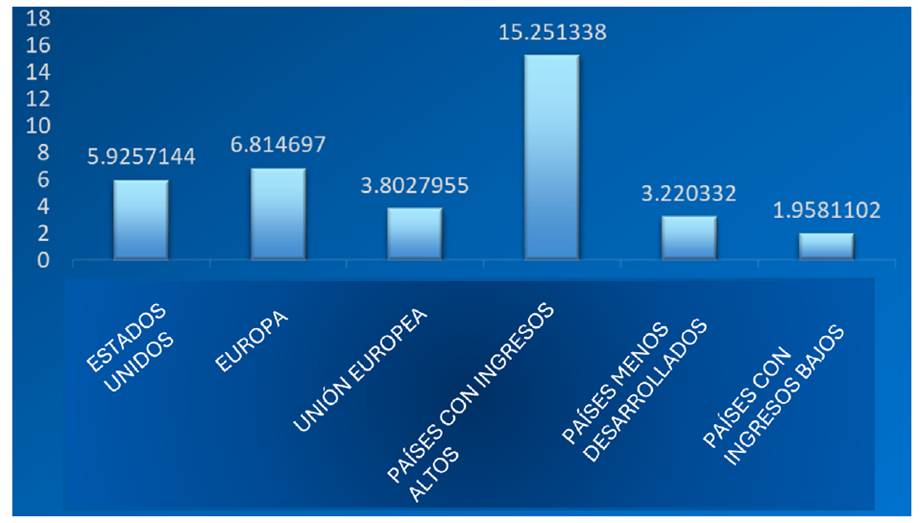
Secondly, if we admit that population growth is responsible of high level GHGs emissions, these emissions should be higher in least-developed and low-income countries than high-income countries where family planning is easy to access. Still, while in developing countries rate of unintended pregnancies is 62-76/1000 women, in developed countries, it’s still high (42-56/1000) despite facilities accessing to family planning services as J. Bearak et al. demonstrated (75). In addition, K. E. Hawkins states that the impact on the climate for a child in a developed country is much greater than in a developing countries as shown in Graphics 1 and 2 (77). Statistics based on an Oxford site (Our World in Data) (78) and the World Bank Open Data (79) show concretely these facts.
-
(75)Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical modelLancet Glob Health, 2018
-
(77)Comment on ‘Climate change and contraception.’BMJ Sex Reprod Health, 2020
-
(78)Annual greenhouse gas emissions by world region, 1850 to 2021Our World in Data, 2023
-
(79)World Bank Open DataWorld Bank Open Data,
Thumbnail
 Source: Our World in Data. Available at: https://ourworldindata.org/grapher/ghg-emissions-byworld-region
Source: Our World in Data. Available at: https://ourworldindata.org/grapher/ghg-emissions-byworld-region
Graphic 1
CO2 Gt/Region in 2021
CO2 Gt/Region in 2021
Thumbnail
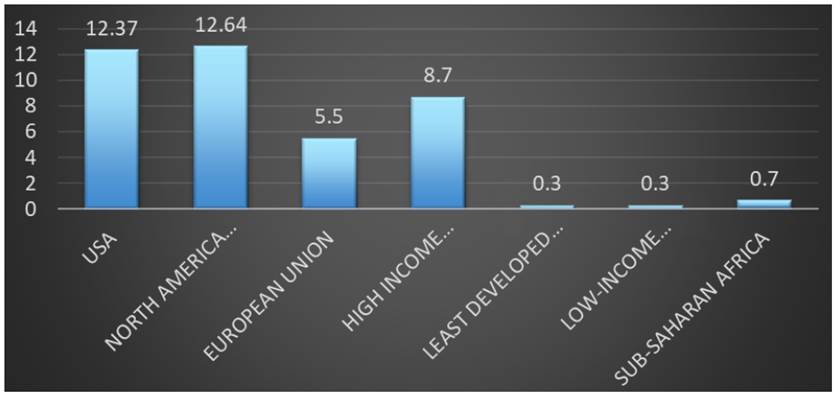 Source: World Bank Open Data. Available at: https://data.worldbank.org
Source: World Bank Open Data. Available at: https://data.worldbank.org
Graphic 2
Tonnes of CO2 per capita in 2020
Tonnes of CO2 per capita in 2020
Even the CO2 emissions per capita are lower in least-developed countries than the higher-developed ones as the chart below shows.
Consequently, it is paradoxical to understand how family planning, supposed to reduce the population growth, could contribute to the reduction of CO2 emissions when the rate of emissions is higher where abortion is legal and contraception is easily accessible.
3.2. Environmental and public health
As explained above, climate change could affect the family planning services. It is wise to ask the question from another point of view. What are the possible impacts of family planning, precisely contraception, on the environment? Since, the methods are numerous, it is more accurate to analyze the most used modern one according to United Nations, Department of Economic and Social Affairs, Population Division (80): two of mechanical barriers [2.2.1] and oral contraceptive pills as hormonal methods [2.2.2].
-
(80)Contraceptive use by Method 2019. Data Booklet, 2019
3.2.1. Mechanical barriers and global warming
The most used mechanical barriers are condoms and Copper IUD. These methods are involved in greenhouse gas emissions directly (condoms) and indirectly (Copper IUD).
a. Condoms
Condoms are mainly fabricated from natural rubber and synthetic rubber (polyisoprene or polyurethane). Two studies have highlighted the environmental impact of condoms’ production. Analyzing the life cycle of natural rubber condoms, W. Jawjit et al. demonstrated that the phase of condoms’ production (fresh latex production, concentrated latex production, condom production, condom transport, condom use and disposal) - succeeding the first phase of preparation (tree planting, latex extraction, latex transport, diesel use, electricity use, chemical use and packaging) - participate for around 52 % to global warming. The condom disposal phase participate for around 45 % of global warming (81). The results are almost the same in M. Birnbach et al.’s study (82). Both studies highlighted the condoms transportation’s impact on GHGs emissions. W. Jawjit et al. quantified this impact by studying transportation by container ships: “the impact from international transportation from Bangkok to Beijing” is between 95-98% (81, p. 103). M. Birnbach et al. estimated that air transport would be accounted for 60% of total GHGs emissions (82, p. 976).
-
(81)Evaluation of the potential environmental impacts of condom production in ThailandJ Integr Environ Sci, 2021
-
(82)A condom’s footprint - life cycle assessment of a natural rubber condomInt J Life Cycle Assess, 2020
-
(81, p. 103)Evaluation of the potential environmental impacts of condom production in ThailandJ Integr Environ Sci, 2021
-
(82, p. 976)A condom’s footprint - life cycle assessment of a natural rubber condomInt J Life Cycle Assess, 2020
As for synthetic rubber condoms, W. Jawjit et al. state that the environmental impact of polyisoprene condom’s production process “is ~2-2.5 times higher in the cases of global warming” due mainly to electricity consumption without forgetting the impact on human toxicity (81, p. 108). In addition, polyurethane production has a huge environmental impact due to the use of petroleum, thus contributing to the emission of GHGs emissions. And since it is non-biodegradable, it has an impact on “diverse fields such as aquatic life, soil health, plants, and humans” (83, p. 406).
-
(81, p. 108)Evaluation of the potential environmental impacts of condom production in ThailandJ Integr Environ Sci, 2021
-
(83, p. 406)Environmental Impact of Polyurethane ChemistryPolyurethane Chemistry: Renewable Polyols and Isocyanates, 2021
b. Copper IUD
There are no direct studies on the impact of Copper IUD’s production on global warming. However, various studies show the impact of the materials used in its production, namely plastic and copper.
F. Chaddad et al. demonstrated that deforestation to exploit copper mines, in the Amazon rainforest, leads to an increase in ground temperature, with significant CO2 emissions which contributes to climate change (84). Copper production has a significant impact on GHGs emissions due to the “intensive energy consumption (electricity, fuel use, transportation, etc.), as explained by D. Dong et al. (85). The Committee on Copper in Drinking Water & National Research Council in the United States have also presented the impact of Copper on water and human toxicity (86).
-
(84)Impact of mining-induced deforestation on soil surface temperature and carbon stocks: A case study using remote sensing in the Amazon rainforestJ South Am Earth Sci, 2022
-
(85)Assessing the future environmental impacts of copper production in China: Implications of the energy transitionJ Clean Prod, 2020
-
(86)Health Effects of Excess CopperCopper in Drinking Water, 2000
To be clear, I am not suggesting that the production of Copper IUD has any causal effect on the environment, but simply pointing out what studies show about the raw materials used in this contraceptive, which needs an attention and further direct studies on the subject.
3.2.2. Oral contraceptive pills and endocrine disruption
One of the main SDGs targets is having good health to be more resilient when facing climate change events (SDG 13.1). Having good health means having good food and water quality. Since the Wingspread declaration on 1991 (87), endocrine disruptors have been known to be harmful for all kinds of life. Pollutants and toxins (pesticides and other chemicals) have an impact on SRHR by disrupting the ability to maintain the safe and sanitary conditions required to have a good health. M. J. Piazza and A. A. Urbanetz specify that these impacts are especially “on the genital area, ovarian steroidogenesis, polycystic ovary syndrome, endometriosis, the structure of the uterus and the vagina, and on the formation of leiomyomas [uterine fibroids]” (88, p. 154). Several studies show that hormonal contraception (especially the synthetic estrogen, 17α-Ethinylestradiol or EE2), as an endocrine disruptor originated from human excrement (particularly urine), has an important impact on aquatic life and human life, which could influence the quality of resilience facing climate change.
-
(87)Déclaration de Wingspread, 1991
-
(88, p. 154)Environmental toxins and the impact of other endocrine disrupting chemicals in women’s reproductive healthJBRA Assist Reprod, 2019
a. Aquatic life
Studies show that EE2 affects the aquatic life on numerous levels. C. Minier et al., C. R. Tyler and S. Jobling have noticed a feminization of the male through the production of vitellogenin (protein as embryonic nutrients, commonly known as egg yolk) and intersexuation (presence of developing oocytes in male testicles) (89,90). S. Jobling et al. and X. Qin et al. have highlighted reproductive disturbance due to delayed spermatogenesis, with poor sperm quality leading to reduced fertility (91,92). M. Saaristo et al. have noted a behavioral change altering the male mate choice (93). A. Kidd et al. have highlighted a near extinction of a whole species of fish from a lake in north-western Ontario, Canada (94).
-
(89An investigation of the incidence of intersex fish in Seine-Maritime and Sussex regionAnalusis, 2000
-
90)Roach, Sex, and Gender-Bending Chemicals: The Feminization of Wild Fish in English RiversBioScience, 2008
-
(91Altered Sexual Maturation and Gamete Production in Wild Roach (Rutilus rutilus) Living in Rivers That Receive Treated Sewage Effluents1Biol Reprod, 2002
-
92)The endocrine disruptor, 17α-ethinyl estradiol, alters male mate choice in a freshwater fishAquat Toxicol, 2019
-
(93)The endocrine disruptor, 17α-ethinyl estradiol, alters male mate choice in a freshwater fishAquat Toxicol, 2019
-
(94)Collapse of a fish population after exposure to a synthetic estrogenProc Natl Acad Sci, 2007
Since aquatic food has a major role in sustainable healthy diets because it contains “unique qualities and nutrients, such as iron, zinc, calcium, iodine, vitamins A, B12 and D, and omega-3 fatty acids” and since its production “has a lower environmental impact than the production of most terrestrial animal-source foods” as states the UN Nutrition department (95, p. 5), “greater production and consumption of aquatic foods depend on a host of factors, be they physical or environmental” such as water pollution (95, p. 37). This means that disrupting aquatic life may have a huge incidence on the completion of SDG 2.1 (nutritious and sufficient food), SDG 3 (health), SDG 6.3 (good quality water) and SDG 14.1 (reducing marine pollution), which lead to fragile human health to face climate change.
-
(95, p. 5)The role of aquatic foods in sustainable healthy diets, 2021
-
(95, p. 37)The role of aquatic foods in sustainable healthy diets, 2021
b. Human health
There is little scientific literature on the impact on human beings of exogenous EE2 from water. However, a number of studies on human and animal have shown the potential health effects of EE2. Already, M. Cargouët et al., S. Jobling and R. Owen have demonstrated that EE2 from the residue of contraceptive pills is present in water even after passing by water treatment stations (96- 98). M. Joyeux asserts that the cumulative exposure to EE2 over 70 years by drinking 2 liters of tap water a day would be 2.5 ng/l (99). It is important to note that the effect of EE2 lies not in quantity but in the fact that it is resistant to biodegradation and in the fact of its mixture with other endocrine disruptors known as “cocktail effect” as proved by V. Delfosse et al.(100).
-
(96-Assessment of river contamination by estrogenic compounds in París area (France)Sci Total Environ, 2004
-
98)The hidden costs of flexible fertilityNature, 2012
-
(99)Résidus médicamenteux et risques sanitaires d’origine hydriqueEnviron Risques Santé, 2006
-
(100)Mechanistic insights into the synergistic activation of the RXR-PXR heterodimer by endocrine disruptor mixturesProc Natl Acad Sci, 2021
Taking all these factors into account, studies showed that female mice6 exposed to low doses of an exogenous EE2 have experienced maternal behavior and emotional alteration (101,102) and some obsessive compulsive disorder (OCD) behavior such a repetitive behavior during lactation (103).
-
(101Developmental Exposure to Ethinylestradiol Affects Reproductive Physiology, the GnRH Neuroendocrine Network and Behaviors in Female MouseFront Neurosci, 2015
-
102)Administration of 17α-ethinylestradiol during pregnancy elicits modifications of maternal behavior and emotional alteration of the offspring in the ratDev Brain Res, 2005
-
(103)Low doses of 17α-ethinyl estradiol alter the maternal brain and induce stereotypies in CD-1 mice exposed during pregnancy and lactationReprod Toxicol, 2017
As for men, D. Margel and N. Fleshner has demonstrated a significant correlation between EE2 in environment water and prostate cancer (104) and that is due to the presence of estrogen receptors in the human prostate, as demonstrated by H. Bonkhoff (105)but more recently estrogens and their receptors have also been implicated in prostate cancer development and tumor progression. Methods Recent experimental and clinical data were reviewed to elucidate pathogenetic mechanisms how estrogens and their receptors may affect prostate carcinogenesis and tumor progression. Results The estrogen receptor beta (ERβ. For their part, M. Rolland et al., the Weybridge report, A. Marques-Pinto and D. Carvalho have noted an important correlation between endocrine disruptors and men’s fertility due to the sperm’s quality and quantity (106- 108).
-
(104)Oral contraceptive use is associated with prostate cancer: an ecological studyBMJ Open, 2011
-
(105)Estrogen receptor signaling in prostate cancer: Implications for carcinogenesis and tumor progressionThe Prostate, 2018
-
(106-Decline in semen concentration and morphology in a sample of 26 609 men close to general population between 1989 and 2005 in FranceHum Reprod, 2013
-
108)Human infertility: are endocrine disruptors to blame?Endocr Connect, 2013
In addition, the use of oral contraceptives has an impact on fetal growth and health, which is a target of SDG 3. Experiences on fetal mouse showed many consequences. B. Timms et al. have noticed an alteration of the fetal mouse and prostate urethra alteration (109). D. K. Waller et al. have noted that the use of OC during the first 3 months of pregnancy is associated with hypoplastic left heart syndrome and gastrochisis (110). N. Meyer et al. have highlighted that EE2 in drinking water caused an increase in placental weight, affected the process of angiogenesis and increased the fetal volume compared to gestational weeks (111). G. Delbès et al. noticed that the exposure to estrogens (endogenous and exogenous) may induce a disorder in fetal and neonatal testicular development (112).
-
(109)Estrogenic chemicals in plastic and oral contraceptives disrupt development of the fetal mouse prostate and urethraProc Natl Acad Sci, 2005
-
(110)Use of Oral Contraceptives in Pregnancy and Major Structural Birth Defects in OffspringEpidemiology, 2010
-
(111)Exposure to 17α-ethinyl estradiol during early pregnancy affects fetal growth and survival in miceEnviron Pollut, 2019
-
(112)Estrogen effects on fetal and neonatal testicular developmentReproduction, 2006
4. Bioethical dilemmas
The analysis in the preceding pages and the various points of view highlight three main bioethical dilemmas: social justice [3.1], health [3.2] and The human relationship with the environment [3.3].
4.1. Social justice
It is a fact that some correlation could exist between population growth and climate change caused by GHGs emissions. But as shown through Oxford site (Our World in Data) (78) and the World Bank Open Data (79), the emissions are higher in developed countries with low birth rates than in less developed countries with high birth rates. According to a study by the Oxford Committee for Famine Relief (OXFAM), "the poorest half of the world's population is responsible for only around 10% of global emissions [...] while the richest 10% of the planet are responsible for around 50% of global emissions" (113). D. Satterthwaite explains that such difference and such high emissions are caused by the increase in wealth and consumption behavior (114, pp. 564-566). This is why he asserts that “it is not fair to equate increases in GHG emissions per person among low-income populations (say from 0.1 to 0.5 tonnes of CO2e per person per year) with comparable GHG increases among high-income populations (for instance, from 7.1 to 7.5 tonnes per person per year)” (114, p. 551). This is why population growth would have significant impact only if it is associated with high levels of consumption behavior. In consequences, social justice means not blaming underdeveloped countries, especially when it comes to population growth, for global warming. This has already been confirmed by the International Conference on Population and Development (ICPD) pointing out that environmental problems, and climate change in particular, are "largely driven by unsustainable patterns of production and consumption" (115, § 1.2).
-
(78)Annual greenhouse gas emissions by world region, 1850 to 2021Our World in Data, 2023
-
(79)World Bank Open DataWorld Bank Open Data,
-
(113)Extreme carbon inequality: Why the París climate deal must put the poorest, lowest emitting and most vulnerable people first, 2015
-
(114, pp. 564-566)The implications of population growth and urbanization for climate changeEnviron Urban, 2009
-
(114, p. 551)The implications of population growth and urbanization for climate changeEnviron Urban, 2009
-
(115, § 1.2)ICPD Programme ActionUNFPA, 2014
In this context, family planning as a solution for climate change, especially as promoted for the poor population, constitutes a direct attack on the principle of social justice. On the one hand, ICPD says clearly that “in no case should abortion be promoted as a method of family planning” (115, § 8.25). On the other hand, it takes a bad source management using a coercive population control on poor populations.
-
(115, § 8.25)ICPD Programme ActionUNFPA, 2014
4.2. Health
The logic of family planning as a solution for climate change is to make people, especially women and fragile ones, more resilient by having a good health. So be it! Nevertheless, at what price? It would be obvious to say: health itself.
-
First, women are the first to pay for the consequences of family planning physiologically and psychologically. Rather than constructing facilities and clinics to help women understanding their bodies and their menstrual cycles, completing the pregnancy with maternity cares follow-up to avoid difficulties, family planning presents, directly or indirectly, women’s fertility, pregnancy and maternity as the source of environmental degradation and climate change. This results in a pressure on women to make the “right choice”, as explained by A. Otzelberger (116, p. 3). But, what is the right to choice to make? The right choice can be only understood if it is made with sincere freedom. And freedom requires to have the possibility also to choose having a child, and not simply refusing one. This is the real condition for realizing the SDGs 3.7.
-
Second, what about the men’s and the environment protection? Since SDGs interact transversely, it seems illogical and unethical to consider that to reduce CO2 emissions, we must resort to population reduction, when there is no evidence of a causal link, through contraceptive methods, which themselves have impacts on health and climate change through CO2 emissions upstream, during and downstream of their production, and through residues found in nature. This brings us to the third dilemma.
-
(116, p. 3)Choice, not control: Why limiting the fertility of poor populations will not solve the climate crisis | Eldis, 2014
4.3. The human relationship with the environment
It seems that the primary focus of presenting family planning as a solution is climate change itself. This fact reflects a certain anti-anthropocentric thinking and an eco-centric ethics (117, pp. 756-765) by conferring nature an intrinsic value. As a result, the moral value of nature takes precedence over that of human beings. As E. Sgreccia states: “human being loses his central role within the natural world to the point of being considered an integral part of environmental reality, and the natural elements are seen as subjects capable of underlining relations of a moral nature with human being” (117, p. 756).
-
(117, pp. 756-765)Manuel de bioéthique. Aspects médicaux sociaux, 2012
-
(117, p. 756)Manuel de bioéthique. Aspects médicaux sociaux, 2012
In this context, to found an environmental ethic with the aim of preserving it, it is impossible to do so without placing the human being at the center of all reflection and action. The reason is: since bioethical discourse, in order to have an integral approach, must take into account metaphysical and ontological dimensions, it is important to return to the scala naturae or the great chain of being derived from Plato and Aristotle. The human being is placed above the terrestrial creatures, by extension, the nature. However, this primary place has not to be considered as a position of dominance, in a utilitarian sense, where human being, in the name of freedom, takes advantage of everything for his own benefit. It has to be a position of responsibility (117, pp. 770-771) where nature, in this particular case, climate change, has to be treated as good, a common good that needs to be preserved, but not to the detriment of human dignity (health, freedom, autonomy, worth, physical integrity, etc.) of the present and the future generations.
-
(117, pp. 770-771)Manuel de bioéthique. Aspects médicaux sociaux, 2012
5. Conclusion
The analysis in the preceding pages leads to this conclusion: family planning, particularly contraceptives, is not a suitable means of combating climate change and achieving the goals of sustainable development, whereas reducing consumption and adopting an appropriate lifestyle is a healthy and responsible attitude to make it possible. Thus, the conflicting studies and the unclear correlation between climate change and population growth invite us to be prudent and cautious while considering family planning as a solution to fight climate change. More in-depth and detailed studies are needed to get a better grasp of the subject.
In the meantime, to better reconciler health preservation, procreative choice and environmental interest, I propose three fundamental attitudes which can only be effective in the long term and they need good programs for their applications.
a. Education
Everything begins with a good education and procreation is not exempt from it. This is why sexual life should not be considered as a spontaneous biologism, nor only from freedom’s perspective without ethical standards, nor through coercive plans to serve ecological ideologies. Procreation is not only a female matter. It is a couple matter where man and women decide together when, how and how many child they want. Sustainability in this case is to give equally (SDG 5) the decision for both partners.
In addition, to have a healthy sexual life is to give young girls (even young boys) a good sexual education that respect their bodies through objective and scientific information to be more aware of and respectful towards each person. This begins by knowing the sexual functions of human bodies understanding a woman’s fertility, which leads to the second attitude.
b. Fertility Awareness-Based Methods
Since, as demonstrated, modern contraceptive methods have an environmental and health impacts, other methods exist that are neither polluting nor harmful to health and that are respectful towards couples’ relationship. It is about Fertility Awareness-Based Methods (118) that are effective (119,120) if women and couples are trained. More respectful of sustainable development (SDGs 3, 5, 6, 8, 13 and 14), these methods are as follows:
-
(118)Cycle féminin au naturel. Gérer sa fertilité et prendre soin de sa santé gynécologique, 2022
-
(119The effectiveness of a fertility awareness based method to avoid pregnancy in relation to a couple’s sexual behaviour during the fertile time: a prospective longitudinal studyHum Reprod, 2007
-
120)Evaluation of Effectiveness of Natural Fertility Regulation Programme in China - WOOMB InternationalScience of Fertility, 2021
-
Calendar-based methods: Ogino-Knaus + Standard Days Method
-
Symptoms-based methods: TwoDay Method, BBT method, ovulation method (Billings), symptothermal method (WHO, 2018)
-
Creighton Model FertilityCare™, Marquette Mehtods, Fertility Education and Medical Management (FEMM), FemTech (smartphone applications, caluclothermia, LH strips or “ovulation tests”, connected bracelet, pocket microscope, Proov urinary strips).
c. Responsible production/consumption behavior
As demonstrated, the lifestyle is a big factor of climate change. One of sustainability conditions to fight the environmental crises is adopting a healthy and responsible production/consumption behavior as recommended particularly by SDG 12.1, 12.2 and 12.8. This demands that each person, each family, each community and each country should take responsibility of each act in everyday life. This is why, the United Nations Department of Economic and Social Affairs calls for solutions independently from demographic trends to achieve a better sustainability. It declares that “high-income and upper-middle-income countries should acknowledge their disproportionate contributions to global environmental damage and take the lead in building a more sustainable economic system for the benefit of future generations” (121).
-
(121)Population growth, environmental degradation and climate change, 2022
Yet, the crucial question remains: who would be prepared and willing, particularly in developed countries, to sacrifices in everyday life?
Referencias
-
1World Health Organization. WHO. Defining sexual health [Internet]. 2002 [citado 15 de agosto de 2023]. Disponible en: Disponible en: https://www.who.int/teams/sexual-and-reproductive-health-and-research/key-areas-of-work/sexual-health/defining-sexual-health Links
-
2Transforming our world: the 2030 Agenda for Sustainable Development. Resolution adopted by the General Assembly on 25 September 2015 [Internet]. Disponible en: https://sdgs.un.org/2030agenda Links
-
3Pörtner HO, Roberts DC, Tingor MMB, Poloczanska E, Mintenbeck K, Alegría A, et al. Climate Change 2022: Impacts, Adaptation and Vulnerability [Internet]. Cambridge, UK and New York, NY, USA: Intergovernmental Panel on Climate Change; 2022 [citado 24 de agosto de 2023]] p. 3056. Disponible en: Disponible en: https://www.ipcc.ch/report/ar6/wg2/ Links
-
4Bryant L, Carver L, Butler CD, Anage A. Climate change and family planning: least-developed countries define the agenda. Bull World Health Organ [Internet]. 2009 Nov [citado 10 de septiembre de 2023]; 87(11):852-7. Disponible en: Disponible en: https://apps.who.int/iris/handle/10665/270557 Links
-
5International Planned Parenthood Federation. IPPF, Population & Sustainability Network. Climate change: “Time to Think Family Planning” [Internet]. London; 2016 [citado 9 de septiembre de 2023] p. 20. Disponible en: Disponible en: https://www.ippf.org/ sites/default/files/2016-11/Climate%20Change%20Time%20to%20Think%20Family%20Planning%20Advocacy%20Toolkit%20Final.pdf Links
-
6International Planned Parenthood Federation. IPPF. The climate crisis and sexual and reproductive health and rights [Internet]. London; 2021 [citado 9 de septiembre de 2023] Disponible en: Disponible en: https://www.ippf.org/sites/default/files/2021-03/ IPPF%20position%20paper%20The%20climate%20crisis%20and%20sexual%20and%20reproductive%20health%20and%20rights_Jan2021.pdf Links
-
7Project Drawdown [Internet]. 2020 [citado 5 de septiembre de 2023]. Drawdown Solutions Library. Disponible en: Disponible en: https://www.drawdown.org/solutions Links
-
8UNFPA. The State of World Population 2015: Shelter from the storm - A transformative agenda for women and girls in a crisis-prone world [Internet]. 2015 Dec [citado 6 de septiembre de 2023]. Disponible en: Disponible en: https://www.unfpa.org/publications/state-world-population-2015 Links
-
9United Nations Human Rights Special Procedures. Safe Climate. A Report of the Special Rapporteur on Human Rights and the Environment [Internet]. UN Environment; 2019 [citado 6 de septiembre de 2023] p. 44. Report No.: A/74/161. Disponible en: Disponible en: https://www.unep.org/resources/report/safe-climate-report-special-rapporteur-human-rights-and-environment Links
-
10Leyser-Whalen O, Chaleshtori SZ, Monteblanco A. Another disaster: Access to abortion after Hurricane Harvey. Health Care Women Int [Internet]. 2020 Oct [citado 5 de septiembre de 2023]; 41(10):1111-27. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8018709/ Links
-
11Human Rights Council. Analytical study on gender-responsive climate action for the full and effective enjoyment of the rights of women - Report of the Office of the United Nations High Commissioner for Human Rights [Internet]. UN; 2019 May [citado 6 de septiembre de 2023] Report No.: A/HRC/41/26. Disponible en: Disponible en: https://undocs.org/A/HRC/41/26 Links
-
12Barot S. In a State of Crisis: Meeting the Sexual and Reproductive Health Needs of Women in Humanitarian Situations. Guttmacher Policy Rev [Internet]. 2017 [citado 6 de septiembre de 2023]; 20:7. Disponible en: Disponible en: https://www.guttmacher.org/gpr/2017/02/state-crisis-meeting-sexual-and-reproductive-health-needs-women-humanitarian-situations Links
-
13Contraception Policy Atlas 2023 [Internet]. Brussels: European Parliamentary Forum (EPF) for Sexual & Reproductive Rights; 2023 [citado 3 de mayo de 2023] Disponible en: Disponible en: https://www.epfweb.org/node/89 Links
-
14Bradley SEK, Polis CB, Bankole A, Croft T. Global Contraceptive Failure Rates: Who Is Most at Risk? Stud Fam Plann [Internet]. 2019 Mar [citado 22 de noviembre de 2022]; 50(1):3-24. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6594038/ Links
-
15Sachs J. Common Wealth. Economics for a Crowded Planet. New York: Penguin; 2009. 400 p. Links
-
16Thurston AM, Stöckl H, Ranganathan M. Natural hazards, disasters and violence against women and girls: a global mixed-methods systematic review. BMJ Glob Health [Internet]. 2021 Apr 1 [citado 8 de enero de 2024];6(4):e004377. Disponible en: Disponible en: https://gh.bmj.com/content/6/4/e004377 Links
-
17Rousseau C. Climate change and sexual and reproductive health: what implications for future research? Sex Reprod Health Matters [Internet]. 2023 Dec [citado 5 de septiembre de 2023]; 31(1):2232196. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10444000/ Links
-
18Sachs J, Lafortune G, Fuller G, Eamon D. Sustainable Development Report 2023. Implementing the SDG Stimulus. Includes the SDG Index and Dashboards [Internet]. New édition. Dublin: Dublin University Press; 2023 [citado 5 de agosto de 2023]. 533 p. Disponible en: Disponible en: https://dashboards.sdgindex.org/chapters Links
-
19Vers l’égalité réelle entre les femmes et les hommes. Chiffres-clés, édition 2022 [Internet]. París: Ministre de l’Égalité entre les femmes et les hommes, de la Diversité et de l’Égalité des chances; 2022 [citado 19 de junio de 2023] Disponible en: Disponible en: https://www.egalite-femmes-hommes.gouv.fr/publication-de-ledition-2022-deschiffres-cles-vers-legalite-reelle-entre-les-femmes-et-les-hommes Links
-
20Junel B. Femmes et hommes sur le marché du travail : des écarts moins marqués en début de vie active [Internet]. Montrouge: Institut national de la statistique et des études économiques; 2019 Nov [citado 21 de junio de 2023]. Report No.: 168. Disponible en: Disponible en: https://www.insee.fr/fr/statistiques/3716874#titre-bloc-1 Links
-
21Meurs D, Pora P. Égalité professionnelle entre les femmes et les hommes en France : une lente convergence freinée par les maternités. Econ Stat Econ Stat [Internet]. 2019 [citado 15 de febrero de 2023] ;(510-511-512):109-30. Disponible en: Disponible en: https://www.insee.fr/fr/statistiques/4253041?sommaire=4253159 Links
-
22McLaughlin L. The Price of Failure of Informed Consent Law: Coercive Sterilizations of HIV-Positive Women in South Africa. Law Inequal [Internet]. 2014 [citado 18 de noviembre de 2022]; 32(1):69-93. Disponible en: Disponible en: https://scholarship.law.umn.edu/lawineq/vol32/iss1/3 Links
-
23High Court of Namibia. LM and Others v Government of Namibia. Nos. 1603/2008; 3518/2008; 3007/2008. 30 July 2012 [Internet]. [citado 17 de noviembre de 2022]. Disponible en: Disponible en: https://namiblii.org/akn/na/judgment/nahc/2012/211/eng@201207-30 Links
-
24Supreme Court of Namibia. Government of the Republic of Namibia v LM and Others. No. SA 49/2012. 3 Novembre 2014 [Internet]. [citado 17 de noviembre de 2022]. Disponible en: Disponible en: https://namiblii.org/akn/na/judgment/nasc/2014/19/eng@2014-11-03 Links
-
25Li H, Mitra M, Wu JP, Parísh SL, Valentine A, Dembo RS. Female Sterilization and Cognitive Disability in the United States, 2011-2015. Obstet Gynecol [Internet]. 2018 Sep [citado 18 de noviembre de 2022]; 132(3):559-64. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6105402/ Links
-
26Uldry M, EDF Women’s Committee. Forced sterilization of persons with disabilities in the European Union [Internet]. Brussels: The European Disability Forum; 2022 Sep [citado 27 de octubre de 2022] Disponible en: Disponible en: https://www.edf-feph.org/content/uploads/2022/09/Final-Forced-Sterilisarion-Report-2022-European-Union-copia_compressed.pdf Links
-
27Devandas-Aguilar C. Santé et droits des filles et des jeunes femmes handicapées en matière de sexualité et de procréation [Internet]. Organisation des Nations Unies; 2017 [citado 15 de noviembre de 2022] Report No. A/72/133. Disponible en: Disponible en: https://www.ohchr.org/en/calls-for-input/report-sexual-and-reproductive-health-and-rights-girls-and-young-women-disabilities Links
-
28ECHR. N.B. v. Slovakia. No. 29518/10, 12 June 2012 [Internet]. Disponible en: Disponible en: https://hudoc.echr.coe.int/fre?i=001-111427 Links
-
29ECHR. V.C v. Slovakia. No. 18968/07, 2011 [Internet]. Disponible en: https://hudoc.echr.coe.int/fre?i=001-107364 Links
-
30Nesher T. Why Is the Birth Rate in Israel’s Ethiopian Community Declining? Haaretz [Internet]. 2012 [citado 24 de noviembre de 2022]; Disponible en: Disponible en: https://www.haaretz.com/2012-12-09/ty-article/.premium/ethiopians-coerced-into-birth-control/0000017f-e7be-df2c-a1ff-ffff7aae0000 Links
-
31Greenwood P. Ethiopian women in Israel “given contraceptive without consent.” The Guardian [Internet]. 2013 [citado 24 de noviembre de 2022]; Disponible en: Disponible en: https://www.theguardian.com/world/2013/feb/28/ethiopian-women-given-contraceptives-israel Links
-
32Arefi A. Quand Israël impose la contraception à ses Éthiopiennes. Le Point [Internet]. 2013 [citado 24 de noviembre de 2022]; Disponible en: Disponible en: https://www.lepoint.fr/monde/quand-israel-force-ses-ethiopiennes-a-la-contraception-30-01-2013-1622050_24.php Links
-
33Nesher T. Israel Admits Ethiopian Women Were Given Birth Control Shots. Haaretz [Internet]. 2013 Jan 27 [citado 24 de noviembre de 2022]; Disponible en: Disponible en: https://www.haaretz.com/israel-news/2013-01-27/ty-article/.premium/ethiopiansfooled-into-birth-control/0000017f-f512-d044-adff-f7fb92c30000 Links
-
34Lewin T. Implanted Birth Control Device Renews Debate Over Forced Contraception. The New York Times [Internet]. 1991 [citado 18 de noviembre de 2022]; Disponible en: Disponible en: https://www.nytimes.com/1991/01/10/us/implanted-birth-control-device-renews-debate-over-forced-contraception.html Links
-
35Burke M. The constitutionality of the use of the Norplant contraceptive device as a condition of probation. Hastings Const Law Q [Internet]. 1992 [citado 18 de noviembre de 2022]; 20(1):207-46. Disponible en: Disponible en: https://repository.uclawsf.edu/cgi/ viewcontent.cgi?article=1512&context=hastings_constitutional_law_quaterly Links
-
36Poursafa P, Keikha M, Kelishadi R. Systematic review on adverse birth outcomes of climate change. J Res Med Sci Off J Isfahan Univ Med Sci [Internet]. 2015 [citado 5 de septiembre de 2023]; 20(4):397-402. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4468458/ Links
-
37Preston EV, Eberle C, Brown FM, James-Todd T. Climate factors and gestational diabetes mellitus risk - a systematic review. Environ Health [Internet]. 2020 [citado 5 de septiembre de 2023]; 19(1):112. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7653781/ Links
-
38Qu Y, Zhang W, Ryan I, Deng X, Dong G, Liu X. Ambient extreme heat exposure in summer and transitional months and emergency department visits and hospital admissions due to pregnancy complications. Sci Total Environ [Internet]. 2021 [citado 5 de septiembre de 2023]; 777:146134. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0048969721012018 Links
-
39Pandipati S, Abel DE. Anticipated impacts of climate change on women’s health: A background primer. Int J Gynecol Obstet [Internet]. 2023 [citado 5 de septiembre de 2023]; 160(2):394-9. Disponible en: Disponible en: https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1002/ijgo.14393 Links
-
40Arnal-Morvan B. Pilule ou pas pilule ? - Tout savoir sur les différents moyens de contraception y compris masculins. Vergèze: Thierry Souccar; 2022. Links
-
41Fitzpatrick D, Pirie K, Reeves G, Green J, Beral V. Combined and progestagen-only hormonal contraceptives and breast cancer risk: A UK nested case-control study and meta-analysis. PLOS Med [Internet]. 2023 [citado 26 de marzo de 2023];20(3):e1004188. Disponible en: Disponible en: https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1004188 Links
-
42International Agency for Research on Cancer. IARC. Pharmaceuticals. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans Volume 100A [Internet]. Lyon: International Agency for Research on Cancer (IARC). World Health Organization (WHO); 2012 [citado 3 de diciembre de 2022]. Disponible en: Disponible en: https://publications.iarc.fr/118 Links
-
43Mohammad-Alizadeh-Charandabi S, Mirghafourvand M, Froghy L, Javadzadeh Y, Razmaraii N. The effect of multivitamin supplements on continuation rate and side effects of combined oral contraceptives: A randomised controlled trial. Eur J Contracept Reprod Health Care [Internet]. 2015 [citado 3 de diciembre de 2022]; 20(5):361-71. Disponible en: Disponible en: https://www.tandfonline.com/doi/full/10.3109/13625187.2015.1010115 Links
-
44Lidegaard Ø, Løkkegaard E, Jensen A, Skovlund CW, Keiding N. Thrombotic Stroke and Myocardial Infarction with Hormonal Contraception. N Engl J Med [Internet]. 2012 [citado 3 de diciembre de 2022]; 366(24):2257-66. Disponible en: Disponible en: https://www.nejm.org/doi/full/10.1056/NEJMoa1111840 Links
-
45Keenan L, Kerr T, Duane M, Van Gundy K. Systematic Review of Hormonal Contraception and Risk of Venous Thrombosis. Linacre Q [Internet]. 2018 [citado 31 de enero de 2024]; 85(4):470-7. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/32431379/ Links
-
46Fairweather D, Rose NR. Women and Autoimmune Diseases. Emerg Infect Dis [Internet]. 2004 [citado 4 de enero de 2023]; 10(11):2005-11. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3328995/ Links
-
47Bernier MO, Mikaeloff Y, Hudson M, Suissa S. Combined oral contraceptive use and the risk of systemic lupus erythematosus. Arthritis Care Res [Internet]. 2009 [citado 4 de enero de 2023]; 61(4):476-81. Disponible en: Disponible en: https://onlinelibrary.wiley.com/doi/epdf/10.1002/art.24398 Links
-
48Larsen SV, Mikkelsen AP, Lidegaard Ø, Frokjaer VG. Depression Associated With Hormonal Contraceptive Use as a Risk Indicator for Postpartum Depression. JAMA Psychiatry. 2023; 80(7):682-9. https://doi.org/10.1001/jamapsychiatry.2023.0807 Links
-
49Nielsen SE, Ertman N, Lakhani YS, Cahill L. Hormonal contraception usage is associated with altered memory for an emotional story. Neurobiol Learn Mem [Internet]. 2011 [citado 5 de mayo de 2023]; 96(2):378-84. Disponible en: Disponible en: https:// www.sciencedirect.com/science/article/pii/S1074742711001249 Links
-
50Kuhlmann S, Wolf OT. Cortisol and memory retrieval in women: influence of menstrual cycle and oral contraceptives. Psychopharmacology (Berl) [Internet]. 2005 Nov 1 [citado 5 de mayo de 2023]; 183(1):65-71. Disponible en: Disponible en: https://link.springer.com/article/10.1007/s00213-005-0143-z Links
-
51Bianchini F, Verde P, Colangeli S, Boccia M, Strollo F, Guariglia C, et al. Effects of oral contraceptives and natural menstrual cycling on environmental learning. BMC Womens Health [Internet]. 2018 Nov 7 [citado 5 de mayo de 2023]; 18(1):179. Disponible en: https://doi.org/10.1186/s12905-018-0671-4 Links
-
52Rumberg B, Baars A, Fiebach J, Ladd ME, Forsting M, Senf W, et al. Cycle and gender-specific cerebral activation during a verb generation task using fMRI: ComParíson of women in different cycle phases, under oral contraception, and men. Neurosci Res [Internet]. 2010 Apr 1 [citado 5 de mayo de 2023]; 66(4):366-71. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0168010209020951 Links
-
53Marečková K, Perrin JS, Nawaz Khan I, Lawrence C, Dickie E, McQuiggan DA, et al. Hormonal contraceptives, menstrual cycle and brain response to faces. Soc Cogn Affect Neurosci [Internet]. 2014 Feb 1 [citado 5 de mayo de 2023]; 9(2):191-200. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3907931/ Links
-
54Hill S. This Is Your Brain on Birth Control: The Surprising Science of Women, Hormones, and the Law of Unintended Consequences. New York: Avery; 2019. Links
-
55Malmborg A, Persson E, Brynhildsen J, Hammar M. Hormonal contraception and sexual desire: A questionnaire-based study of young Swedish women. Eur J Contracept Reprod Health Care [Internet]. 2016 [citado 3 de diciembre de 2022]; 21(2):158-67. Disponible en: Disponible en: https://www.tandfonline.com/doi/ abs/10.3109/13625187.2015.1079609?journalCode=iejc20 Links
-
56World Health Organization Department of Sexual and Reproductive Health and Research (WHO/SRH), Johns Hopkins Bloomberg School of Public Health/ Center for Communication Programs (CCP), Knowledge SUCCESS. Family Planning: A Global Handbook for Providers. Evidence-based guidance developed through worldwide collaboration [Internet]. 4th ed. Geneva and Baltimore: World Health Organization and Johns Hopkins; 2022 [citado 7 de ocubre de 2023]. Disponible en: Disponible en: https://www.who.int/publications/i/item/9780999203705 Links
-
57Kim SK, Romero R, Kusanovic JP, Erez O, Vaisbuch E, Mazaki-Tovi S. The prognosis of pregnancy conceived despite the presence of an intrauterine device (IUD). J Perinat Med [Internet]. 2010 [citado 19 de diciembre de 2022]; 38(1):45-53. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3418877/ Links
-
58Thorp JM. Public Health Impact of Legal Termination of Pregnancy in the US: 40 Years Later. Scientifica [Internet]. 2012 [citado 5 de noviembre de 2022]; 2012:e980812. Disponible en: Disponible en: https://www.hindawi.com/journals/scientifica/2012/980812/ Links
-
59Raymond EG, Shannon C, Weaver MA, Winikoff B. First-trimester medical abortion with mifepristone 200 mg and misoprostol: a systematic review. Contraception [Internet]. 2013 [citado 11 de febrero de 2024]; 87(1):26-37. Disponible en: Disponible en: https://www.contraceptionjournal.org/article/S0010-7824(12)00643-9/fulltext Links
-
60Upadhyay UD, Desai S, Zlidar V, Weitz TA, Grossman D, Anderson P, et al. Incidence of Emergency Department Visits and Complications After Abortion. Obstet Gynecol [Internet]. 2015 [citado 11 de febrero de 2024]; 125(1):175. Disponible en: Disponible en: https://journals.lww.com/greenjournal/fulltext/2015/01000/incidence_of_emergency_department_visits_and.29.aspx Links
-
61Mentula MJ, Niinimäki M, Suhonen S, Hemminki E, Gissler M, Heikinheimo O. Immediate adverse events after second trimester medical termination of pregnancy: results of a nationwide registry study. Hum Reprod [Internet]. 2011 [citado 11 de febrero de 2024]; 26(4):927-32. Disponible en: https://doi.org/10.1093/humrep/der016 Links
-
62Zhao P, Zhao Y, He J, Bai XX, Chen J. Subsequent placenta accreta after previous mifepristone-induced abortion: A case report. World J Clin Cases [Internet]. 2021 [citado 6 de noviembre de 2024]; 9(33):10244-8. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8638051/ Links
-
63Krugh M, Maani CV. Misoprostol. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 [citado 6 de noviembre de 2022]. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK539873/ Links
-
64Bradshaw Z, Slade P. The effects of induced abortion on emotional experiences and relationships: A critical review of the literature. Clin Psychol Rev [Internet]. 2003 Dec 1 [citado 7 de noviembre de 2022]; 23(7):929-58. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0272735803000928 Links
-
65Gebeyehu NA, Tegegne KD, Abebe K, Asefa Y, Assfaw BB, Adella GA, et al. Global prevalence of post-abortion depression: systematic review and Meta-analysis. BMC Psychiatry [Internet]. 2023 [citado 28 de noviembre de 2023]; 23(1):1-16. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10605843/ Links
-
66Rue VM, Coleman PK, Rue JJ, Reardon DC. Induced abortion and traumatic stress: a preliminary comParíson of American and Russian women. Med Sci Monit [Internet]. 2004 [citado 7 de noviembre de 2022]; 10(10):SR5-16. Disponible en: Disponible en: https://pubmed.ncbi.nlm.nih.gov/15448616/ Links
-
67Skop I. Chemical Abortion: Risks Posed by Changes in Supervision. J Am Physicians Surg [Internet]. 2022 [citado 15 junio de 2023]; 27(2):56-61. Disponible en: Disponible en: https://lozierinstitute.org/chemical-abortion-risks-posed-by-changes-in-supervision/ Links
-
68Cuellar Torriente M. Silent Uterine Rupture with the Use of Misoprostol for Second Trimester Termination of Pregnancy: A Case Report. Obstet Gynecol Int [Internet]. 2011 [citado 1 de octubre de 2023;2011:e584652. Disponible en: Disponible en: https://www.hindawi.com/journals/ogi/2011/584652/ Links
-
69Maslovich MM, Burke LM. Intrauterine Fetal Demise. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 [citado 1 de octubre de 2023. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK557533/ Links
-
70O’Neill BC, Liddle B, Jiang L, Smith KR, Pachauri S, Dalton M, et al. Demographic change and carbon dioxide emissions. The Lancet [Internet]. 2012 [citado 24 de agosto de 2023]; 380(9837):157-64. Disponible en: Disponible en: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(12)60958-1/abstract Links
-
71Bongaarts J, Sitruk-Ware R. Climate change and contraception. BMJ Sex Reprod Health [Internet]. 2019 Oct 1 [citado 24 de agosto de 2023]; 45(4):233-5. Disponible en: Disponible en: https://srh.bmj.com/content/45/4/233 Links
-
72Proctor RN, Schiebinger L. Yale E360. 2022 [citado 24 de agosto de 2023]. How Preventing Unwanted Pregnancies Can Help on Climate. Disponible en: Disponible en: https://e360.yale.edu/features/unwanted-pregnancy-contraception-abortion-climate-change Links
-
73Joyce TJ, Tan R, Zhang Y. Back to the Future? Abortion Before & After Roe [Internet]. National Bureau of Economic Research; 2012 [citado 7 de septiembre de 2023]. (Working Paper Series). Disponible en: Disponible en: https://www.nber.org/papers/ w18338 Links
-
74Bearak J, Popinchalk A, Ganatra B, Moller AB, Tunçalp Ö, Beavin C, et al. Unintended pregnancy and abortion by income, region, and the legal status of abortion: estimates from a comprehensive model for 1990-2019. Lancet Glob Health [Internet]. 2020 [citado 29 de octubre de 2022]; 8(9):e1152-61. Disponible en: Disponible en: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(20)30315-6/fulltext Links
-
75Bearak J, Popinchalk A, Alkema L, Sedgh G. Global, regional, and subregional trends in unintended pregnancy and its outcomes from 1990 to 2014: estimates from a Bayesian hierarchical model. Lancet Glob Health [Internet]. 2018 Apr 1 [citado 24 de agosto de 2023]; 6(4):e380-9. Disponible en: Disponible en: https://www.thelancet.com/journals/langlo/article/PIIS2214-109X(18)30029-9/fulltext Links
-
76Guttmacher Institute [Internet]. 2020 [citado 11 de enero de 2024]. Unintended Pregnancy and Abortion Worldwide. Disponible en: Disponible en: https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide Links
-
77Hawkins KE. Comment on ‘Climate change and contraception.’ BMJ Sex Reprod Health [Internet]. 2020 [citado 24 de agosto de 2023]; 46(2):156-156. Disponible en: Disponible en: https://srh.bmj.com/content/46/2/156.2 Links
-
78Our World in Data [Internet]. 2023 [citado 24 de agosto de 2023]. Annual greenhouse gas emissions by world region, 1850 to 2021. Disponible en: Disponible en: https://ourworldindata.org/grapher/ghg-emissions-by-world-region Links
-
79World Bank Open Data [Internet]. [citado 5 de septiembre de 2023]. World Bank Open Data. Disponible en: Disponible en: https://data.worldbank.org/ Links
-
80United Nations, Department of Economic and Social Affairs, Population Division. Contraceptive use by Method 2019. Data Booklet [Internet]. New York: United Nations; 2019 [citado 26 de noviembre de 2022]. 26 p. Disponible en: Disponible en: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/files/documents/2020/Jan/un_2019_contraceptiveusebymethod_databooklet.pdf Links
-
81Jawjit W, Pavasant P, Kroeze C, Tuffrey J. Evaluation of the potential environmental impacts of condom production in Thailand. J Integr Environ Sci [Internet]. 2021 [citado 2 de enero de 2023]; 18(1):89-114. Disponible en: Disponible en: https://www.tandfonline.com/doi/full/10.1080/1943815X.2021.1949354 Links
-
82Birnbach M, Lehmann A, Naranjo E, Finkbeiner M. A condom’s footprint - life cycle assessment of a natural rubber condom. Int J Life Cycle Assess [Internet]. 2020 [citado 2 de enero de 2023]; 25(6):964-79. Disponible en: Disponible en: https://link.springer. com/article/10.1007/s11367-019-01701-y Links
-
83Adetunji C, Olaniyan O, Anani O, Inobeme A, Mathew J. Environmental Impact of Polyurethane Chemistry. In: Polyurethane Chemistry: Renewable Polyols and Isocyanates [Internet]. 2021 [citado 23 de octubre de 2023]. Disponible en: Disponible en: https://www.researchgate.net/publication/351811523_Environmental_Impact_of_Polyurethane_Chemistry Links
-
84Chaddad F, Mello FAO, Tayebi M, Safanelli JL, Campos LR, Amorim MTA, et al. Impact of mining-induced deforestation on soil surface temperature and carbon stocks: A case study using remote sensing in the Amazon rainforest. J South Am Earth Sci [Internet]. 2022 [citado 8 de septiembre de 2023]; 119:103983. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S089598112200270X Links
-
85Dong D, van Oers L, Tukker A, van der Voet E. Assessing the future environmental impacts of copper production in China: Implications of the energy transition. J Clean Prod [Internet]. 2020 [citado 8 de septiembre de 2023]; 274:122825. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0959652620328705 Links
-
86Committee on Copper in Drinking Water, National Research Council. Health Effects of Excess Copper. In: Copper in Drinking Water [Internet]. National Academies Press (US); 2000 [citado 8 de septiembre de 2023]. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/books/NBK225400/ Links
-
87Déclaration de Wingspread [Internet]. 1991. Disponible en: http://www.reseau-environnement-sante.fr/la-declaration-de-wingspread/ Links
-
88Piazza MJ, Urbanetz AA. Environmental toxins and the impact of other endocrine disrupting chemicals in women’s reproductive health. JBRA Assist Reprod. 2019; 23(2):154-64. Links
-
89Minier C, Caltot G, Leboulanger F, Hill EM. An investigation of the incidence of intersex fish in Seine-Maritime and Sussex region. Analusis [Internet]. 2000 [citado 2 de enero de 2023]; 28(9):801-6. Disponible en: Disponible en: https://analusis.edpsciences.org/articles/analusis/abs/2000/09/minier/minier.html Links
-
90Tyler CR, Jobling S. Roach, Sex, and Gender-Bending Chemicals: The Feminization of Wild Fish in English Rivers. BioScience [Internet]. 2008 [citado 21 de marso de 2022]; 58(11):1051-9. Disponible en: Disponible en: https://academic.oup.com/bioscience/article/58/11/1051/264727 Links
-
91Jobling S, Beresford N, Nolan M, Rodgers-Gray T, Brighty GC, Sumpter JP, et al. Altered Sexual Maturation and Gamete Production in Wild Roach (Rutilus rutilus) Living in Rivers That Receive Treated Sewage Effluents1. Biol Reprod [Internet]. 2002 [citado 4 de enero de 2023]; 66(2):272-81. Disponible en: Disponible en: https://academic.oup.com/biolreprod/article/66/2/272/2723352 Links
-
92Qin X, Lai KP, Wu RSS, Kong RYC. Continuous 17α-ethinylestradiol exposure impairs the sperm quality of marine medaka (Oryzias melastigma). Mar Pollut Bull [Internet]. 2022 [citado 6 de enero de 2023]; 183:114093. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0025326X22007755 Links
-
93Saaristo M, Johnstone CP, Xu K, Allinson M, Wong BBM. The endocrine disruptor, 17α-ethinyl estradiol, alters male mate choice in a freshwater fish. Aquat Toxicol [Internet]. 2019 [citado 6 de enero de 2023]; 208:118-25. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0166445X18309408 Links
-
94Kidd KA, Blanchfield PJ, Mills KH, Palace VP, Evans RE, Lazorchak JM, et al. Collapse of a fish population after exposure to a synthetic estrogen. Proc Natl Acad Sci [Internet]. 2007 [citado 2 de enero de 2023]; 104(21):8897-901. Disponible en: Disponible en: https://www.pnas.org/doi/10.1073/pnas.0609568104 Links
-
95UN Nutrition. The role of aquatic foods in sustainable healthy diets [Internet]. Rome; 2021 [citado 12 de enero de 2024] Disponible en: Disponible en: https://www.unnutrition.org/wp-content/uploads/FINAL-UN-Nutrition-Aquatic-foods-Paper_EN_.pdf Links
-
96Cargouët M, Perdiz D, Mouatassim-Souali A, Tamisier-Karolak S, Levi Y. Assessment of river contamination by estrogenic compounds in París area (France). Sci Total Environ [Internet]. 2004 [citado 9 de enero de 2023]; 324(1):55-66. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0048969703006430 Links
-
97Jobling S, Owen R. Ethinyl oestradiol in the aquatic environment. In: Late Lessons from Early Warnings: Science, Precaution, Innovation [Internet]. Copenhague: European Environment Agency; 2013 [citado 2 de enero de 2023]. Disponible en: Disponible en: https://www.eea.europa.eu/publications/late-lessons-2#additional-files Links
-
98Owen R, Jobling S. The hidden costs of flexible fertility. Nature [Internet]. 2012 [citado 6 de enero de 2023]; 485(7399):441. Disponible en: Disponible en: https://www.nature.com/articles/485441a Links
-
99Joyeux M. Résidus médicamenteux et risques sanitaires d’origine hydrique. Environ Risques Santé [Internet]. 2006 [citado 9 de enero de 2023]; 5(4):1-9. Disponible en: Disponible en: http://www.internuntia.fr/pdf/edp_residus_medicamenteux_mj.pdf Links
-
100Delfosse V, Huet T, Harrus D, Granell M, Bourguet M, Gardia-Parège C, et al. Mechanistic insights into the synergistic activation of the RXR-PXR heterodimer by endocrine disruptor mixtures. Proc Natl Acad Sci [Internet]. 2021 [citado 21 de marzo de 2022]; 118(1):e2020551118. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7817120/ Links
-
101Derouiche L, Keller M, Martini M, Duittoz AH, Pillon D. Developmental Exposure to Ethinylestradiol Affects Reproductive Physiology, the GnRH Neuroendocrine Network and Behaviors in Female Mouse. Front Neurosci [Internet]. 2015 [citado 20 de marzo de 2023]; 9. Disponible en: Disponible en: https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2015.00463/full Links
-
102Arabo A, Lefebvre M, Fermanel M, Caston J. Administration of 17α-ethinylestradiol during pregnancy elicits modifications of maternal behavior and emotional alteration of the offspring in the rat. Dev Brain Res [Internet]. 2005 [citado 15 de febrero de 2023]; 156(1):93-103. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0165380605000325 Links
-
103Catanese MC, Vandenberg LN. Low doses of 17α-ethinyl estradiol alter the maternal brain and induce stereotypies in CD-1 mice exposed during pregnancy and lactation. Reprod Toxicol [Internet]. 2017 [citado de octubre de 2023]; 73:20-9. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/S0890623817301910 Links
-
104Margel D, Fleshner NE. Oral contraceptive use is associated with prostate cancer: an ecological study. BMJ Open [Internet]. 2011 [citado 6 de enero de 2023]; 1(2):e000311. Disponible en: Disponible en: https://bmjopen.bmj.com/content/1/2/e000311 Links
-
105Bonkhoff H. Estrogen receptor signaling in prostate cancer: Implications for carcinogenesis and tumor progression. The Prostate [Internet]. 2018 [citado 10 de enero de 2023]; 78(1):2-10. Disponible en: https://doi.org/10.1002/pros.23446 Links
-
106Rolland M, Le Moal J, Wagner V, Royère D, De Mouzon J. Decline in semen concentration and morphology in a sample of 26 609 men close to general population between 1989 and 2005 in France. Hum Reprod [Internet]. 2013 [citado 4 de enero de 2023]; 28(2):462-70. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4042534/ Links
-
107Bergman A, Brandt I, Brouwer B, Harisson P, Holmes P, Humfrey C, et al. European workshop on the impact of endocrine disrupters on human health and wildlife. Reports of proceedings [Internet]. Weybridge, UK: European Commission, European Environment Agency, World Health Organisation, uropean Office; 1996 [citado 3 de enero de 2023] Report No.: CGNA17549ENC. Disponible en: Disponible en: http://www.iehconsulting.co.uk/IEH_Consulting/IEHCPubs/EndocrineDisrupters/ WEYBRIDGE.pdf Links
-
108Marques-Pinto A, Carvalho D. Human infertility: are endocrine disruptors to blame? Endocr Connect [Internet]. 2013 [citado 13 de enero de 2023]; 2(3):R15-29. Disponible en: Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3845732/ Links
-
109Timms BG, Howdeshell KL, Barton L, Bradley S, Richter CA, vom Saal FS. Estrogenic chemicals in plastic and oral contraceptives disrupt development of the fetal mouse prostate and urethra. Proc Natl Acad Sci [Internet]. 2005 [citado 6 de enero de 2023]; 102(19):7014-9. Disponible en: Disponible en: https://www.pnas.org/doi/10.1073/pnas.0502544102 Links
-
110Waller DK, Gallaway MS, Taylor LG, Ramadhani TA, Canfield MA, Scheuerle A. Use of Oral Contraceptives in Pregnancy and Major Structural Birth Defects in Offspring. Epidemiology [Internet]. 2010 [citado 10 de enero de 2023]; 21(2):232-93. Disponible en: Disponible en: https://journals.lww.com/epidem/Fulltext/2010/03000/Use_of_ Oral_Contraceptives_in_Pregnancy_and_Major.11.aspx Links
-
111Meyer N, Santamaria CG, Müller JE, Schumacher A, Rodriguez HA, Zenclussen AC. Exposure to 17α-ethinyl estradiol during early pregnancy affects fetal growth and survival in mice. Environ Pollut [Internet]. 2019 [citado 6 de enero de 2023]; 251:493-501. Disponible en: Disponible en: https://www.sciencedirect.com/science/article/pii/ S0269749119306943 Links
-
112Delbès G, Levacher C, Habert R. Estrogen effects on fetal and neonatal testicular development. Reproduction [Internet]. 2006 [citado 15 de febrero de 2023]; 132(4):527-38. Disponible en: Disponible en: https://rep.bioscientifica.com/view/journals/rep/132/4/1320527.xml Links
-
113Oxfam Media Briefing. Extreme carbon inequality: Why the París climate deal must put the poorest, lowest emitting and most vulnerable people first [Internet]. 2015 [citado 24 de agosto de 2023] Disponible en: Disponible en: https://policy-practice.oxfam.org/resources/extreme-carbon-inequality-why-the-paris-climate-deal-must-putthe-poorest-lowes-582545/ Links
-
114Satterthwaite D. The implications of population growth and urbanization for climate change. Environ Urban [Internet]. 2009 [citado 5 de septiembre de 2023]; 21(2):545-67. Disponible en: Disponible en: https://www.iied.org/g02648 Links
-
115United Nations. ICPD Programme Action [Internet]. Disponible en: https://www.unfpa.org/icpd-redesign . UNFPA; 2014 [citado 10 de enero de 2023]. Disponible en: Disponible en: https://www.unfpa.org/icpd-redesign Links
-
116Otzelberger A. Choice, not control: Why limiting the fertility of poor populations will not solve the climate crisis | Eldis [Internet]. Geneva: CARE International; 2014 [citado 5 de septiembre de 2023] Disponible en: Disponible en: https://careclimatechange.org/choice-not-population-control/ Links
-
117Sgreccia E. Manuel de bioéthique. Aspects médicaux sociaux. París: Mame; 2012. Links
-
118Vallet M, Saab-Tsnobiladzé S. Cycle féminin au naturel. Gérer sa fertilité et prendre soin de sa santé gynécologique. París: Leduc; 2022. Links
-
119Frank-Herrmann P, Heil J, Gnoth C, Toledo E, Baur S, Pyper C, et al. The effectiveness of a fertility awareness based method to avoid pregnancy in relation to a couple’s sexual behaviour during the fertile time: a prospective longitudinal study. Hum Reprod [Internet]. 2007 [citado 24 de noviembre de 2022]; 22(5):1310-9. Disponible en: Disponible en: https://academic.oup.com/humrep/article/22/5/1310/2914315?login=false Links
-
120Qian SZ, Zhang DW, Huai-Zhi Z, Lu RK, Peng L, He CH, et al. Evaluation of Effectiveness of Natural Fertility Regulation Programme in China - WOOMB International [Internet]. Science of Fertility. 2021 [citado 30 de noviembre de 2022]. Disponible en: Disponible en: https://woombinternational.org/wp-content/uploads/2022/05/Evaluation-of-the-Effectiveness-of-a-Natural-Fertility-Regulation-Programme-in-China.pdf Links
-
121United Nations Department of Economic and Social Affairs. United Nations. 2022 [citado 21 de octubre de 2023]. Population growth, environmental degradation and climate change. Disponible en: Disponible en: https://www.un.org/en/desa/population-growth-environmental-degradation-and-climate-change Links
Appendix
SDG 2.1: by 2030, end hunger and ensure access by all people, in particular the poor and people in vulnerable situations, including infants, to safe, nutritious and sufficient food all year round.
SDG 3.1: by 2030, reduce the global maternal mortality ratio to less than 70 per 100,000 live births.
SDG 3.2: by 2030, end preventable deaths of newborns and children under 5 years of age, with all countries aiming to reduce neonatal mortality to at least as low as 12 per 1,000 live births and under-5 mortality to at least as low as 25 per 1,000 live births.
SDG 3.3: by 2030, end the epidemics of AIDS, tuberculosis, malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases.
SDG 3.7: by 2030, ensure universal access to sexual and reproductive health-care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programmes.
SDG 5.2: eliminate all forms of violence against all women and girls in the public and private spheres, including trafficking and sexual and other types of exploitation.
SDG 5.3: achieve universal health coverage, including financial risk protection, access to quality essential health-care services and access to safe, effective, quality and affordable essential medicines and vaccines for all.
SDG 5.6: ensure universal access to sexual and reproductive health and reproductive rights as agreed in accordance with the Programme of Action of the International Conference on Population and Development and the Beijing Platform for Action and the outcome documents of their review conferences.
SDG 6.3: by 2030, improve water quality by reducing pollution, eliminating dumping and minimizing release of hazardous chemicals and materials, halving the proportion of untreated wastewater and substantially increasing recycling and safe reuse globally.
SDG 8.5: by 2030, achieve full and productive employment and decent work for all women and men, including for young people and persons with disabilities, and equal pay for work of equal value.
SDG 10.2: by 2030, empower and promote the social, economic and political inclusion of all, irrespective of age, sex, disability, race, ethnicity, origin, religion or economic or other status.
SDG 12.1: implement the 10-year framework of programmes on sustainable consumption and production, all countries taking action, with developed countries taking the lead, taking into account the development and capabilities of developing countries.
SDG 12.2: by 2030, achieve the sustainable management and efficient use of natural resources.
SDG 12.8: by 2030, ensure that people everywhere have the relevant information and awareness for sustainable development and lifestyles in harmony with nature.
SDG 13.1: strengthen resilience and adaptive capacity to climate-related hazards and natural disasters in all countries.
SDG 14.1: by 2025, prevent and significantly reduce marine pollution of all kinds, in particular from land-based activities, including marine debris and nutrient pollution.