Artículos
Bioethical assessment of vasectomy without children: personal autonomy against maleficence
Téllez Martínez-Fornés, Miguel*
 http://orcid.org/0009-0003-3459-6471
http://orcid.org/0009-0003-3459-6471
Abellán Salort, José Carlos**
http://orcid.org/0000-0002-4470-4646
Fouz López, María Concepción***
http://orcid.org/0009-0007-9868-8243
http://orcid.org/0009-0003-3459-6471Abellán Salort, José Carlos**
http://orcid.org/0000-0002-4470-4646Fouz López, María Concepción***
http://orcid.org/0009-0007-9868-8243
-
Publication dates-
September 10, 2024
Jul-Sep , 2024
- Article in PDF
- Article in XML
- Automatic translation
- Send this article by e-mail
- Share this article +
Summary
Vasectomy is usually requested by a couple with children who consider that they have completed their family project. In the clinical practice of the urology office of the Spanish health system, the professional must respond to an increasingly frequent demand: the request for vasectomy in young and childless patients, which raises many doubts in the urologist, regarding the suitability of its realization.
Vasectomy causes a supposedly irreversible loss of reproductive function. Performed at the request of healthy, young, childless men, while respecting their autonomy of decision, it can nevertheless be maleficent.
This paper aims to provide bioethical arguments concerning the performance of voluntary vasectomy in these cases and to evaluate the basis of the ethical criteria usually invoked to justify it. Subsequently, the legal aspects of vasectomy in Spain and the role of the professional’s conscientious objection are analyzed.
Keywords::
family planning, male sterilization, conscientious objection, health policy
1. Introduction
In this paper we will bioethically analyze the issue of vasectomy, based on a real clinical case from a urology practice, with the triple objective of providing bioethically argued reflections on the performance of voluntary vasectomy in healthy, young, childless men; to evaluate the basis and consistency of the criteria that are commonly applied to justify the performance of vasectomy and, finally, to study the ethical criteria applicable to the performance of vasectomy.
Secondly, we will analyze the medical and legal aspects of vasectomy in Spain, which implies considering the aspects of personal autonomy in this situation, reflecting on the role of the professional’s conscientious objection, and exposing the negative social effects of this decision in the context presented.
We have started from the official public statistical data obtained from the urological clinical experience of voluntary vasectomy in Spain between the years 2010 - 2020 and we have carried out a review of the scientific literature. Technical comments on vasectomy are based on urological texts widely disseminated among professionals and are shown in bibliographic references 9, 15 and in the article entitled Vasectomy and reversal: important aspects, published in the journal Urologic Clinics of North America in 2009. To find documentation related to sterilization in the absence of children and in young people, a manual search in free text was carried out using the Spanish and English language limits and publication years 2000-2022 in PubMed and in the Google browser. In both cases the terms “family planning”, “male sterilization”, “vasectomy without children”, “sterilization in young adults”, “family planning”, “male sterilization”, “vasectomy without children” and “sterilization of young adults” were used. Information on conscientious objection was sought in references 19, 20, 37, 89 and 96 of the articles and on health policies related to family planning published in texts of declarations of the United Nations (UN) and the World Health Organization (WHO). In the bioethical reflection, recognized texts in medical bioethics and particularly in personalist bioethics and Catholic doctrine are used, fundamentally texts from the Vatican, Manual of Bioethics by E. Sgreccia, Theological Bioethics by J. Gafo, the Belmont report and Principles of Biomedical Ethics by T. L. Beauchamp and J. F. Childress.
Legal texts from the Constitutional Court of Spain, Law 41/2002, of November 14, 2002, basic law regulating patient autonomy and rights and obligations regarding clinical information and documentation, and Organic Law 2/2010, of March 3, 2010, on sexual and reproductive health and the voluntary interruption of pregnancy were also consulted.
Information from the Spanish national health system published by the Spanish Ministry of Health has been consulted to obtain statistical information on vasectomy in Spain.
We conclude by proposing the reasons for the revision of the specialist’s criteria in the face of these requests in which, even if the competence and autonomy of the applicants are accredited, they can result in a maleficent practice, an assessment that is particularly evident from the postulates of personalist bioethics and bioethics with a Christian foundation.
2. Case history
A twenty-three-year-old man comes to the urology office of a hospital of the Spanish public health system to request a vasectomy. He works in an advertising company as a graphic designer. He comes from a family consisting of himself and his parents, he has no siblings and no children. He has had a partner for one year. He has not previously had any other partners. Neither he nor his current partner has any desire to have children. They have discussed it extensively with each other.
His reasons for requesting a vasectomy are that he has no desire to have children, that he does not trust the efficacy of other contraceptive methods, and that he feels that parenthood would force him to give up his current lifestyle, making it impossible for him to enjoy many activities. On the other hand, he feels that his decision has no relevance in the world, where there are already many inhabitants. He has even discussed it with his parents, who have also shown no objection to never being grandparents.
The urologist has suggested that he is too young to make this decision irreversibly and has explained to him that previous experience shows that there is a high possibility of later regret, often associated with a change of partner. The patient admits that these explanations are very reasonable but considers that they are not enough to change his mind.
In this context, the ethical considerations of the case of voluntary sterilization performed by a urologist are discussed.
3. Vasectomy, in the field of family planning
The Universal Declaration of Human Rights of the United Nations Organization (UNO) of December 10, 1948, in its article 16.3 states that “the family is the natural and fundamental group unit of society and is entitled to protection by society and the State” (1).
-
(1)Declaración Universal de Derechos Humanos, 1948
In 1978, in the Declaration of Alma Ata, the WHO recognized as one of its important tasks to help its member states achieve the goal of ensuring that every human being enjoys the highest attainable standard of health, including sexual and reproductive health (2).
-
(2)1978 Alma-Ata Declaration - WHO,
On December 18, 1979, the United Nations General Assembly adopted the Convention on the Elimination of All Forms of Discrimination against Women. (3) In Article 5, it states that there should be a “proper understanding of maternity as a social function”, with the need for both sexes to share fully in the responsibility for raising children. In Article 10, it includes the right to information specific to the health and welfare of the family, in Article 14 it speaks specifically of information on family planning and in Article 16 it advocates guaranteeing the right of women “to decide freely and responsibly on the number and spacing of their children”.
-
(3)Convención sobre la eliminación de todas las formas de discriminación contra la mujer,
Similarly, the International Conference on Population and Development held in Cairo in 1994 (4) and the Fourth World Conference on Women held in Beijing in 1995 (5), both envisage the objective of strengthening a positive approach to sexuality by promoting conditions that enable people to experience sexuality in all its aspects with confidence, pleasure, and security. Safe and effective contraception not only makes responsible procreation more viable, but also allows for a satisfying and pleasurable sexual life and reduces the fear of unwanted pregnancy (6).
-
(4)Conferencia Internacional sobre la Población y el Desarrollo, 1994
-
(5)Cuarta Conferencia Mundial sobre la Mujer, 1995
-
(6)Asociación de la satisfacción sexual en pacientes con vasectomía y sin vasectomía de 20 a 40 años adscritos en la UMF 93,
For its part, the Catholic Church admits that, “if there are serious reasons for spacing births, derived from the physical or psychological conditions of the spouses, or from external circumstances, the Church teaches that it is then licit to take into account the natural rhythms immanent to the generative functions in order to use marriage only in infertile periods and thus regulate the birth rate without offending the moral principles we have just recalled” (7). This means that Catholic bioethics, based on the anthropological vision and social doctrine of the Church, admits the ethics of responsible family planning, although direct sterilization, which has an anti-procreative purpose, would not be a licit means of family planning.
-
(7)Carta Encíclica Humanae Vitae, (7),
Therefore, family planning is generally considered a human right that improves the living conditions of women and the population, contributes to reduce poverty, and allows to reduce the pressure that a sustained population increase would exert on the environment (8).
-
(8)Aspectos ético-legales en la esterilización quirúrgica voluntariaRevista de Obstetricia y Ginecología de Venezuela, 2016
Vasectomy is a safe and simple male sterilization method that contributes to birth control, with growing social acceptance, although in some cultural traditions there are still some factors of rejection to its practice as a contraceptive strategy.
The voluntary request for vasectomy is made by the male partner or jointly by the couple when they seek a family planning method. Sometimes its practice is not performed in the context of family planning but in certain medical situations (risky pregnancies or hereditary diseases). The exceptional cases in which it is performed non-voluntarily are not the subject of the analysis presented here (9).
-
(9)La vasectomía: estudio de 300 intervenciones. Revisión de la literatura nacional y de sus complicacionesActas Urológicas Españolas, 2004
In Spain, about 12% of couples choose definitive methods of contraception (10). In the year 2000, it was estimated that about 10,000 men underwent vasectomy in Spain each year (11). In the Community of Madrid, 4,181 vasectomies were performed in 2009, compared to 3,246 tubal ligations.
-
(10)Factores biopsicosociales que influyen en la elección de la vasectomíaAten Fam, 2015
-
(11)La vasectomía: Estudio de 300 intervenciones. Revisión de la literatura nacional y de sus complicacionesActas Urológicas Españolas, 2004
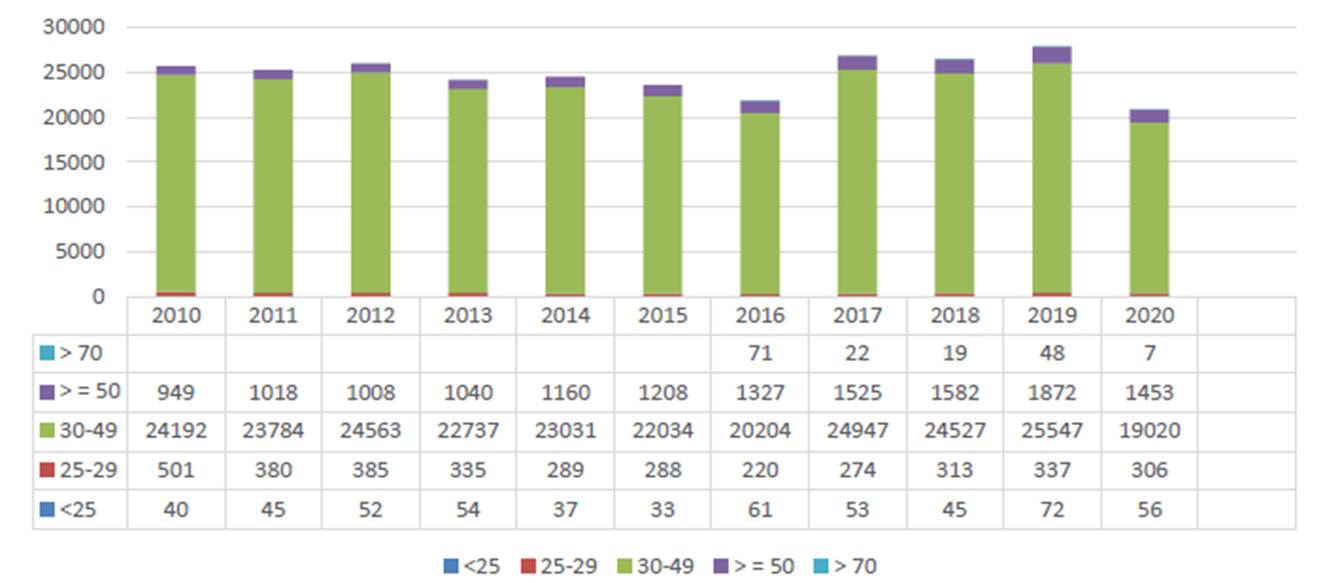
The following graphs show the updated data on vasectomies performed in Spain in recent years (12). Graph 1 shows that about 26,000 vasectomies are performed annually in Spain between 2010 and 2020.
-
(12)Registro de Actividad de Atención Especializada, RAE-CMBD,
Thumbnail
 Source: own preparation.
Source: own preparation.
Graph 1
Evolution of vasectomies in Spain by age range 2010-2020
Evolution of vasectomies in Spain by age range 2010-2020
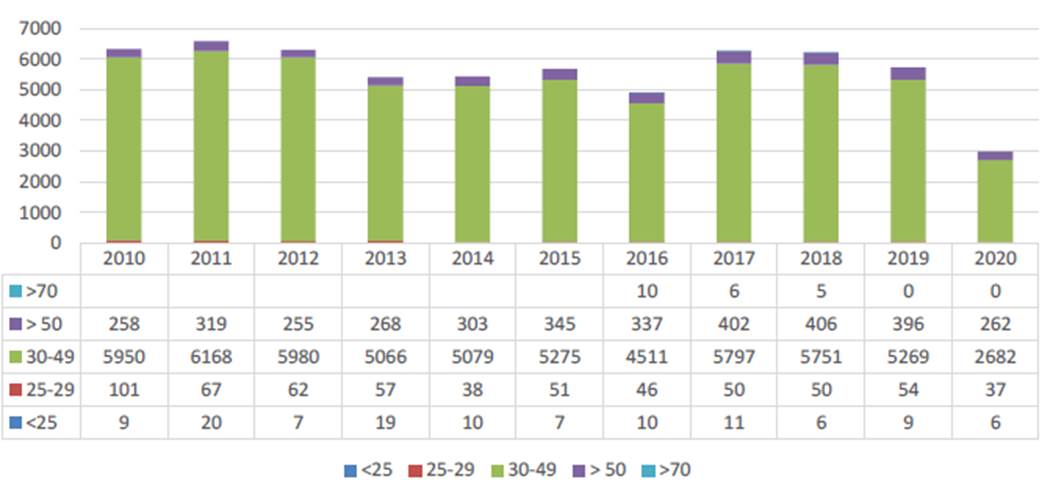
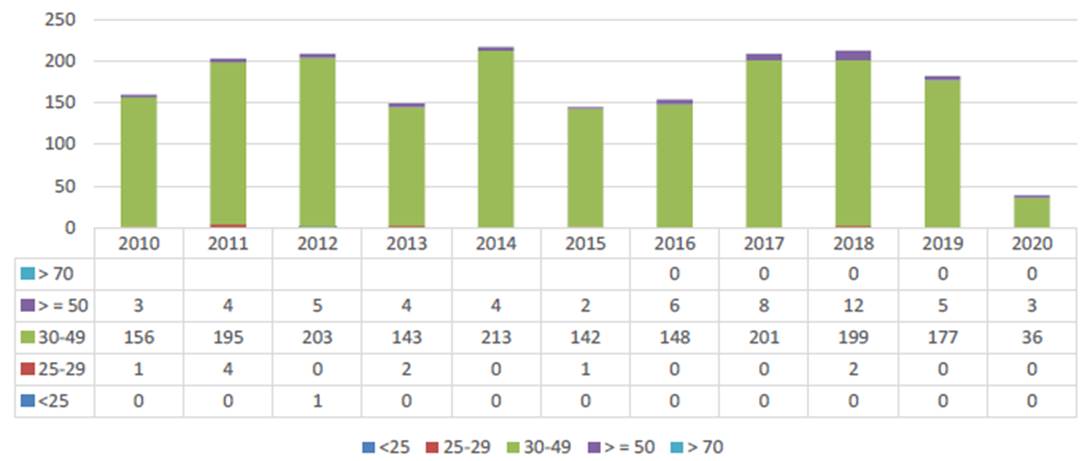
In the Community of Madrid (13), as shown in Graph 2, they represent about 6000 per year and, as shown in Graph 3, at the Severo Ochoa University Hospital in Leganés (14), there are approximately 200. The majority age group is between 30 and 49 years, followed by those over 50 years and then, at a greater distance, by the group of men between 25 and 29 years. Vasectomies performed in men under 25 years of age are a very small minority, constituting a percentage of about 1.5 per thousand vasectomies.
-
(13)Registro de Actividad de Atención Especializada, RAE-CMBD,
-
(14)CMBD (conjunto mínimo básico de datos),
Thumbnail
 Source: own preparation.
Source: own preparation.
Graph 2
Evolution of vasectomies in the community of Madrid by age range 2010-2020
Evolution of vasectomies in the community of Madrid by age range 2010-2020
Thumbnail
 Source: own preparation.
Source: own preparation.
Graph 3
Evolution of vasectomies in the H.U. Severo Ochoa by age range 2010-2020
Evolution of vasectomies in the H.U. Severo Ochoa by age range 2010-2020
4. Medical aspects of vasectomy
Vasectomy is mainly performed as a method of family planning when permanent contraception is desired, in stable couples who do not want to have any more children. However, it can also be indicated for medical reasons, such as high-risk pregnancies for women, transmission of hereditary diseases, contraindications for hormonal contraceptives or even by court order in cases permitted by law. It is also used as part of the treatment for certain diseases that require the removal of organs, such as testicular or prostate tumors.
From the point of view of the surgical technique, vasectomy is performed on an outpatient basis under local anesthesia. It involves the ligation and section of the vas deferens to interrupt the sperm’s exit route. It is important to note that the contraceptive effect is not immediate; it takes about three months for the absence of spermatozoa in the ejaculated semen to occur due to the remnant in the distal spermatic ducts. This requires a sperm analysis to confirm the effectiveness of the procedure.
Vasectomy has relative contraindications, including chronic scrotal pain, severe illness, childlessness, age less than 30 years, and lack of a current relationship. Chronic scrotal pain can worsen after vasectomy, and some complications can be potentially severe in cases of serious illness. The other contraindications relate to personal changes that could lead to a request for vasectomy reversal due to a change in paternity desire.
Vasectomy complications can be immediate or long-term. Immediate complications include bleeding, hematoma, and infections, including epididymitis and abscesses. Long-term complications include chronic scrotal pain (1%) and spontaneous recanalization of the vase deferens, although the latter is rare (0.03 - 1.2%). After a decade, a small percentage of men opt for a reversal due to a change in their desire to have children. In these cases, semen quality may not be optimal, which may require assisted reproductive techniques. A critical aspect is vasectomy failure, which can result in unwanted pregnancies with psychological, family, and legal implications (15).
-
(15)Guía clínica de la Asociación Europea de Urología sobre la vasectomía,
5. Vasectomy as a satisfying surgery means vs. results
Most of the time, the male requesting a vasectomy does not suffer from any pathology, neither he nor his partner, but the reason for the request is only the desire not to have any more children. Consequently, the applicant for this voluntary sterilization wants the procedure to be minimal, uncomplicated and with an effective result. In this case, azoospermia (16,17).
-
(16Aspectos ético-legales en la esterilización quirúrgica voluntariaRevista de Obstetricia y Ginecología de Venezuela, 2016
-
17)Aspectos ético-legales en la esterilización quirúrgica voluntariaRevista de Obstetricia y Ginecología de Venezuela, 2016
The usual medical activity is in the field of curative or assistance medicine and, in this situation, the contractual relationship between the physician and the patient is equated to “a lease of services” and the application of the lex artis or good medical practice is required. In these cases, the physician is obliged to provide the appropriate means to achieve the desired end, cure, or improvement (18,19,20).
-
(18Aspectos ético-legales en la esterilización quirúrgica voluntariaRevista de Obstetricia y Ginecología de Venezuela, 2016
-
19La objeción de conciencia en el ámbito clínico. Propuesta para un uso apropiado (II)Revista de Calidad Asistencial, 2011
-
20)Estudio jurisprudencial en medicina satisfactivaRevista Española de Medicina Legal, 2013
However, when the surgical service requested does not seek the cure of a pathology but the satisfaction of a demand to achieve a certain end (satisfactory or voluntary medicine), there is a modification in this contractual relationship between the physician, in this case the technician, and the user or client, who is not a patient. It is now equated to a work contract, with an obligation of results, which, in addition to adequate means, requires the achievement of a specific end. It is therefore necessary to provide a greater guarantee that the result will be achieved (21,22).
-
(21Estudio jurisprudencial en medicina satisfactivaRevista Española de Medicina Legal, 2013
-
22)Estudio jurisprudencial en medicina satisfactivaRevista Española de Medicina Legal, 2013
In the case of satisfactory or voluntary medicine, the patient comes to the doctor for the improvement of his physical appearance or for the transformation of a biological activity, such as sexual activity and, in the specific case of vasectomy, azoospermia. In principle, a result would be required and there could be liability for defective performance of the contract. We can therefore speak, not of a patient, but of a client.
This difference between the two modalities is not always very clear, especially since the right to reproductive health is assumed to be included in the right to health, this being understood by the WHO as wellbeing in its psychological and social aspects, not only physical, including preventive activities aimed at avoiding risks to the patient’s health or integrity.
This has resulted in the courts not resolving these differences between obligation of means and results in an absolute manner but admitting certain nuances depending on the case (23). If the concept of health is understood in such a broad manner, the limits between satisfactory and curative surgery are blurred, since family planning is understood as one more part of the health of individuals.
-
(23)Estudio jurisprudencial en medicina satisfactivaRevista Española de Medicina Legal, 2013
At this point, and applied to the case presented here, the question remains as to whether, in the absence of children, it is possible to speak of family planning in the strict sense of the term. In this conceptual line, the request for a vasectomy without children would be closer to the concept of satisfactory or voluntary medicine than other cases.
6. Request for vasectomy reversal
About 6% of men who have undergone vasectomy request subsequent vasectomy reversal. This reconstruction is also requested to treat obstructive infertility (24).
-
(24)Técnicas de reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America,
Historically, the first reversal of a spermatic duct obstruction was performed by Edward Martin in 1902 in a case of obstruction secondary to epididymitis. It was Quinby in 1919 who published the first report on vasectomy reversal and then O’Connor published the first series of reversals in 14 patients, reporting success in 64% of cases. Since the 1960s, multiple reversal techniques, both macrosurgical and microsurgery, have been developed (25).
-
(25)Historia de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
Surgical reconstruction of spermatic duct obstruction does not always achieve satisfactory results. The cause of failure may be functional, due to the existence of IgA-type anti-sperm agglutinating antibodies, or to anatomical problems such as the formation of sperm granulomas on the anastomosis, which cause obstruction.
Other factors also influence the success of this surgery: fertility prior to vasectomy, previous inguinal hernia surgery that can compromise the seminal duct at other anatomical levels, the age of the couple (worse prognosis if older than 40 years), having the same partner as before the vasectomy is associated with better results, and the history of a previous reversal surgery with a bad result also worsens the chances.
Finally, a very important factor conditioning the outcome of reconstruction surgery should be noted: the interval between vasectomy and reconstruction. The Vasovasostomy Study Group reports that the patency and pregnancy rates when this interval is less than three years are 97% and 76%. These percentages decrease to 71% and 30% respectively when more than fifteen years have elapsed (26). Although vasectomy reversal remains the appropriate treatment in most couples, in some cases, it may be more cost-effective to resort to sperm extraction and in vitro fertilization techniques (27).
-
(26)Factores predictivos del éxito de la reversión microquirúrgica de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(27)Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
7. Legal framework of vasectomy in Spain
In Spain, the Penal Code on voluntary human sterilization was modified in 1983. The legislative regulation of this measure for incapable subjects was reformed in 1995 in the new Penal Code, whose article 156 contains the regulations regarding the sterilization of persons subject to guardianship due to their functional diversity, which introduced the concept of “best interest”, absent in article 428 of the previous Penal Code.
It is included in the portfolio of services of the National Health System and is included in the Royal Decree 1030/2006, of September 15, establishing the Portfolio of Common Services of the National Health System and the procedure for its updating, in its Annex III, Portfolio of common services of specialized care, where the “Performance of tubal ligation and vasectomies, according to the protocols of the health services, excluding the reversal of both” is included textually.
As regards the legal liability of the professional, the Spanish legal system uses the system of fault-based liability when it comes to judging the physician’s liability. An obligation of means is required, which is determined by the lex artis ad hoc, consisting of the application of the correct and usual clinical practice in these cases. The physician is obliged, not to cure, but to provide all the care required according to the state of science. In this situation, when an injury occurs, it is the patient who is obliged to prove the fault or negligence of the physician and to demonstrate the causal link between the physician’s actions and the injury. (28) To do so, he must have access to the medical records. The absence of this reverses the burden of proof, which becomes the responsibility of the professional.
-
(28)Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
However, in the field of satisfactory or voluntary medicine, an obligation of results is required. Failure to achieve them implies a breach of this obligation, which leads to a presumption of the physician’s fault. For his defense, it is necessary for the professional to prove his diligence. In these cases, the doctrine of the Supreme Court recognizes that a greater guarantee is required to obtain the desired result, in this case, to avoid procreation. In cases of voluntary medicine in which there is no promise of results, the performance must be in accordance with the lex artis ad hoc(29).
-
(29)Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
As regards jurisprudence, in 1994, the Spanish Constitutional Court admitted the forced sterilization of the mentally ill (30,31).
-
(30Bioética y esterilizaciónManual de Bioética. I Fundamentos y ética biomédica, 2009
-
31)Sentencia 215/1994, 1994
The Supreme Court, in general, rules out any kind of strict liability if the action is not negligent, nor is there any reversal of the burden of proof, with the patient being the one who must prove negligence and the cause-effect relationship, except for cases in which it is considered that there has been a disproportionate or grossly disproportionate damage (32).
-
(32)Sentencia 215/1994, 1994
In general, the Consumers and Users Law is not applicable except in organizational aspects (poor organization of the service), defects in the material or in the provision of health services (for example, that it was not carried out under the required hygienic conditions).
In addition, the theory of “loss of opportunity” would be applicable to voluntary sterilization only about the adequate treatment of any complications that might arise because of the vasectomy surgical procedure. (33)
-
(33)Sentencia 215/1994, 1994
As for the situation in other countries in our environment, it should be noted that, in France, it was approved in 2001 and in Italy, in a judgment of June 1987 by the Supreme Court (34), based on the argument that sterilization “would lead to greater relaxation and serenity in relations with one’s own spouse or partner.”
-
(34)Sentencia 215/1994, 1994
The Council of Ministers of the European Union, in Resolution No. 75 of November 14, 1975, recommended that voluntary sterilization for family planning purposes be made available as a medical service (35).
-
(35)Sentencia 215/1994, 1994
8. Information and consent for vasectomy
Spanish Law 41/2002 of November 14, 2002, the basic law regulating patient autonomy and the rights and obligations regarding clinical information and documentation(36) regulates the right to information and informed consent: “free, voluntary and conscious agreement of a patient, expressed in the full use of his faculties after receiving adequate information, for an action affecting his health to take place” (Art. 3).
-
(36)Ley 41/2002, de 14 de noviembre, básica reguladora de la autonomía del paciente y de derechos y obligaciones en materia de información y documentación clínicaBOE, 2022
In voluntary or satisfactory medicine, the information must also be objective, truthful, complete, and accessible. It is essential that it includes the possibility of failure of the intervention, which means that information must be given on the probability of obtaining or not obtaining the result sought. Information on any possible sequelae, risks, complications, or adverse results that may appear, both frequent and rare, is also mandatory.
The latter is a differentiating feature compared to the usual information provided in curative medicine, since in the case of voluntary or satisfactory medicine, the user must be warned of any risk, even the exceptional ones.
It should be borne in mind that this knowledge can induce the subject not to undergo an unnecessary, dispensable, or relatively necessary intervention. Thus, the decision of the Supreme Court of July 2, 2002, (prior to the Law on Patient Autonomy), states that “complete and accessible information -exhaustive, sufficient, truthful and loyal- and the obtaining of informed consent constitute a basic prerequisite for the patient to be able to decide with full awareness and freedom about the operation of voluntary or satisfying medicine aimed at obtaining the purpose of vasectomy, ...” (37,38,39).
-
(37El consentimiento en materia de bioética y biojurídica. La esterilización en el derecho español y en derecho comparado,
-
38El consentimiento en materia de bioética y biojurídica. La esterilización en el derecho español y en derecho comparado,
-
39)El consentimiento en materia de bioética y biojurídica. La esterilización en el derecho español y en derecho comparado,
On the other hand, if there is no harm linked to the omission of consent or information or to the medical intervention itself, it does not generate professional liability or relevant consequences.
It is advisable to hold two medical interviews to ensure that informed consent is being given correctly. In the first one, complete information would be given and in the second one the consent would be signed.
In some risk situations, this informative practice would be particularly indicated: young, with few or no children, all children of the same sex, a child with deteriorating health, unstable marriage, single or widowed, marital coercion, decision taken in an exceptionally difficult situation, hasty decision, lack of access to other contraceptive methods, religious or cultural conditioning factors, subsidies or other incentives that condition the decision, incorrect or incomplete information, insecurity about whether to have more children if she loses one or if she remarries (40,41).
-
(40El consentimiento en materia de bioética y biojurídica. La esterilización en el derecho español y en derecho comparado,
-
41)Selected practice recommendations for contraceptive useWHO, 2016
9. Bioethical analysis of the case
9.1 Special characteristics: age, absence of children
The question arises as to whether the age of the subject requesting vasectomy is a special characteristic for the request he is making. Certainly, young people are, after all, free to perform many acts in their lives, including the choice of their personal relationships, lifestyle, economic investments, and so on. In fact, on many occasions, they perform risky acts that they may later regret (42).
-
(42)Sterilisation of young, competent, and childless adultsBritish Medical Journal, 2005
However, it must be considered that the decision taken in this case requires the collaboration of a physician to perform a non-curative act and, therefore, is not strictly a medical act (43).
-
(43)Sterilisation of young, competent, and childless adultsBritish Medical Journal, 2005
Along the same lines, one may wonder about the situation that arises when not having children.
There are aspects that may compromise the decision in the future, mainly the appearance or change to a new partner who wants children and the impossibility of guaranteeing the reversibility of fertility. Again, the physician is directly involved in the achievement of the individual’s goal, which could affect him or her in the future.
10. Moral goods involved in this case
10.1 Autonomy: subject’s capacity to decide
Since the publication of the Belmont Report in 1979 (44), the progressive application of the concept of autonomy developed by Beauchamp and Childress in their principlism theory has begun (45).
-
(44)Comisión Nacional para la Protección de los sujetos humanos de investigación biomédica y del comportamiento. Informe Belmont. Principios y guías éticos para la protección de los sujetos humanos de investigación,
-
(45)Principles of biomedical ethics, 2001
This principle did not appear in the Hippocratic Oath or in the ancient Codes of Ethics. The individual is considered as being capable of deliberating on his or her personal objectives and acting under the direction of this deliberation.
The principle of autonomy implies giving value to the opinions and choices of individuals thus considered and refraining from obstructing their actions, unless these produce a clear harm to others, even if they produce it to themselves. To show disrespect for an autonomous agent is to repudiate the criteria of these persons, to deny an individual the freedom to act according to such criteria or to withhold information necessary for them to make a judgment, when there are no convincing reasons for doing so (46).
-
(46)Capacidad de moral e competencia jurídica para tomar uma decisâo autonómicaConflitos Morais en Bioética Clínica, 2022
When analyzing the decision made by the individual patient requesting sterilization, it is necessary to verify that the conditions for an autonomous decision are met that he acts intentionally, with understanding of the meaning and consequences of his action and without sufficiently powerful external influences that lead to control his will and determine the meaning of the action.
Of these three conditions, understanding and external influences can occur with varying degrees of autonomy, but not the intentionality of the decision, and it is at this point where the analysis of the case must be carried out.
On the other hand, respecting the autonomy of the individual requires recognition of the right to have one’s own point of view, to exercise one’s own options and to act in accordance with one’s values and beliefs (47).
-
(47)Bioética teológica, 2003
The principle of autonomy requires that the autonomous actions of individuals should not be subjected by others to external controls that limit or impede them. This principle is binding under equal conditions but can be limited by other moral considerations in situations of conflict with other ethical values or with the autonomy of other persons (48).
-
(48)Sobre el principio de autonomía en la bioéticaBioética, autonomía y libertad, 2007
Modern anthropology has incorporated autonomy as a fundamental notion in philosophical thought: every man deserves to be respected in decisions that are not harmful to others.
In the specific case at hand, there are no arguments to maintain that youth makes the exercise of autonomy impossible. The intention is clear and corresponds to the desire not to have children; understanding is framed by the information he receives, which will be analyzed in the following point: and the existence of external influences should be assessed in the interview that the physician holds with him.
It is true that decisions can change with the passage of time, which has a lot to do with the responsibility that the person has in his or her choice and in assuming its consequences, but this argument does not invalidate the authenticity of the option initially taken.
It is interesting to point out that a decision taken coldly and after adequate reflection with sufficient information is more autonomous than any other taken hastily and, perhaps, in less independent conditions. And this argument has nothing to do with youth or maturity (49).
-
(49)Sterilisation of young, competent, and childless adultsBritish Medical Journal, 2005
It is also necessary to analyze whether the absence of children can be a condition for autonomy in the decision. Although the concept of family planning is based on responsible maternity/paternity, there are no reasons based exclusively on freedom of decision that invalidate the personal option of not forming a family or not having children. In the latter situation, the only requirement would be that this personal decision be shared by the couple, with prior knowledge and without coercion, in the form of an agreement or transactional agreement. Even this last condition could be questioned (50).
-
(50)Selected practice recommendations for contraceptive use, 2016
It is worth asking, like Habermas, how the meaning of the question, what should I do, is transformed when my actions touch the interests of others, in this case of my partner, and lead to a conflict. It seems that these cases should be assessed more impartially, deciding alongside the preferences of others (51).
-
(51)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
10.2 Information: Irreversibility and risks of the procedure
In the case we are analyzing, information plays a more relevant role than in other more common vasectomy requests. It is essential to provide exhaustive information on the following points (52):
-
(52)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
-
Risks: of course, as in all cases of elective or voluntary surgery, there must be complete information on all risks, including those that are very rare and particularly the very serious ones, even if they are exceptional. In particular, the risk of bleeding or serious life-threatening infections must be reported (53,54,55).
-
Complications: particularly those that remain or appear in the long term, such as chronic scrotal pain and spontaneous recanalization (56,57,58).
-
Irreversibility of the procedure: Together with the uncertain results of reconstructive surgery, associated with the progressive loss of fertility originated by the maintained obstruction (59,60,61).
-
Regret: The strong association between regret and the request for subsequent reversal and the two factors that concur in the case: youth and absence of children (62,63).
-
Health care cost: In our public health care system, vasectomy reversal vasectomy reconstruction is not included in the service portfolio. This point should be expressly informed and should be included in the text of the informed consent document that is requested for the performance of the vasectomy. In some cases, it can be a very important condition for making the final decision (64, 65).
-
Alternatives: Specifically, information should be provided on the existence and availability of effective contraceptive methods that are not irreversible (66).
-
(53De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
-
54De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
-
55)Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(56Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
57Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
58)Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(59Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
60Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
61)Técnicas de reversión de la vasectomía. En Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(62Técnicas de reversión de la vasectomía. En Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
63)Factores predictivos del éxito de la reversión microquirúrgica de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(64Real Decreto-ley 16/2012, de 20 de abril, de medidas urgentes para garantizar la sostenibilidad del Sistema Nacional de Salud y mejorar la calidad y seguridad de sus prestacionesBOE, 2012
-
65)Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantesUrologic Clinics of North America, 2009
-
(66)Bioética y esterilizaciónManual de Bioética. I Fundamentos y ética biomédica, 2009
10.3 Maleficence: Loss of reproductive function
Male sterilization in humans implies a consensual and, in principle, irreversible injury to the generative faculties of the male, which could be interpreted as “maleficent”, that is, harmful to the person requesting it, from a bioethical perspective that takes into consideration the inviolability of the person and his physical integrity and functions, including the reproductive, the unitotality of the human being and the principles of optionality and globality.
a) Inviolability of the person and his physical integrity
On the rational level, this foundation would be found in the fact that the person is the principal and transcendent value. It is an ontological and ethical foundation. If man were the arbitrary master of himself, why could he not have the same dominion over others?
This approach, whether creationist or personalist, which considers the value of man as absolute or intangible, is opposed to the immanentist concept that considers man as the master of man or the State as the master of man, which opens the door to all kinds of violence: sterilization, but also suicide, euthanasia, abortion (67).
-
(67)Bioética y esterilizaciónManual de Bioética. I Fundamentos y ética biomédica, 2009
Bioethics of personalist inspiration bases its argumentation on the affirmation of the existence of an objective moral law in human nature, in its deepest being, identified by the universal natural law, which requires that the moral order be adapted to the ontological order.
This interpretation does not allow the voluntary and arbitrary suppression of one of the essential dimensions of one’s being. Sexuality represents a physical, psychological, social, and spiritual dimension of the totality of the person and is governed by ethical norms of a heteronomous and universal character that sanction the impossibility of separating these dimensions without contradicting the natural law and, with it, man himself.
The point is that the unitive and procreative dimensions are distinct, but they are associated and, from this point of view of natural law, one cannot be suppressed without harming the other (68).
-
(68)Bioética y esterilizaciónManual de Bioética. I Fundamentos y ética biomédica, 2009
However, there is a widespread opinion that, in the present context and with respect to the progress of biomedicine, there is a need to develop a new interpretation of the human body, considering its biological, psychological, and social aspects (69,70).
-
(69Bioética teológica, 2003
-
70)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
If subjectivist or materialist positions of life are adopted, the previous interpretation of the person is not valid, since moral norms in sexuality, human procreation, etc., would only be the result of social agreement, being defined by the thinking of the majority and not by the imperative of any objective moral rule. From this perspective, if it is not made clear that not all uses of reason are valid as a source of moral autonomy, although we are obliged to seek sources of legitimacy for our decisions, the specter of moral relativism is present (71).
-
(71)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
This reflection constitutes the central axis of the problem: autonomy versus physical integrity. Where is the priority? Life and physical integrity are fundamental rights that carry with them a duty of respect on the part of others and a duty of protection on the part of the subject himself. In this case, it is not permissible for the individual to self-injure. This basic character makes it difficult to establish the automatic priority of autonomy over physical integrity in all cases (72,73,74).
-
(72De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
-
73De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
-
74)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
In the specific case of sterilization, a part of the subject’s biology is eliminated, the reproductive faculty is intentionally irreversibly suppressed, bodily injury is not justifiable in a therapeutic purpose, and can seriously affect the development of the personality. In view of this argument, personalist thought cannot accept the priority of autonomy over the integrity of the biological faculties of the human being (75).
-
(75)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
b) Unitotality of the human being
According to Elio Sgreccia, egregious representative of the bioethical current of ontological personalism, the person is a unifying existence, plurality and diversity of faculties and vital expressions. Each unity refers to plurality and there is a hierarchy of personal goods ordered for the good of the whole.
This means that it is licit to surgically remove an organ or a part of it to safeguard the totality of physical life, when there is no other remedy, and the decision cannot be postponed in time. This would be the case of curative or therapeutic sterilization.
However, it would not be licit to suppress a physical good simply by an act of the will. In this sense, voluntary sterilization would entail a mutilation or lasting suspension of the procreative faculty, which goes against this concept of unity and uniqueness (76).
-
(76)De moralidad y eticidad. Dos dimensiones para la bioéticaActa Bioética, 2002
There are other different personalist interpretations that appeal to the principles of optionality and globality to consider also the whole of the psychological and existential situations of the subject.
c) The principles of optionality and globality
The principle of optionality (77) is proposed by E. Sgreccia as the ethical possibility of choosing the lesser evil or the dominant beneficial end between two hypotheses that cannot be practiced simultaneously, in this case fertility and conjugal union. To save the latter, it would be permissible to suppress the former, by means of contraceptives or sterilization. It is understood in this case that the globality of the personal good includes conjugal, family or social well-being, which would require the suppression of fertility.
-
(77)Congregación para la doctrina de la feAcerca de la esterilización en los hospitales católicos, 1975
It can be interpreted, on the contrary, that the suppression of the physical dimension implies that there is no more globality (78).
-
(78)Congregación para la doctrina de la feAcerca de la esterilización en los hospitales católicos, 1975
d) Justice: Social repercussion
Continuing with this same personalist approach, for E. Sgreccia, the legalization of voluntary sterilization is presented as a symptom of uncertainty and the fall of ethical values that affect life and the person. They indicate an anomie, a lack and emptiness of the value of life and the value of the person. It could be considered a symptom of a psychic character, of a destructive nature, which should rather arouse alarm (79).
-
(79)Congregación para la doctrina de la feAcerca de la esterilización en los hospitales católicos, 1975
In contrast to their ideas, although sharing some elements of the substance of the question, we find the argumentation of the anti-analysts. One of their ideologues, David Benatar, argues that existence inflicts real harm regardless of the feelings of the existing being and, consequently, it is always morally wrong to beget more sentient beings (80). The position could not be clearer in terms of its goal, the extinction of the human species, and its means, voluntary sterilization. Framed in nihilistic thought, however, it clearly coincides with Sgreccia’s assertion of the destructive nature of sterilization.
-
(80)Better Never to Have Been: The Harm of Coming Into Existence, 2006
Between these two positions lies much of contemporary thought. UN policies regarding family planning recognize the difficulty of carrying out responsible parenthood without adequate means of contraception (81,82). The role of women in modern society is also associated with the possibility of enjoying responsible, healthy, and socially beneficial motherhood (83). Maternity and paternity are personal goods, but not only of individuals, since they are also valuable for the common good, and therefore the defense and even the promotion of goods such as maternity, natality, or potentially fertile family models should be promoted.
-
(81Selected practice recommendations for contraceptive use, 2016
-
82)Selected practice recommendations for contraceptive use, 2016
-
(83)Selected practice recommendations for contraceptive use, 2016
It is necessary to harmonize this vision of maternity/paternity with the support of the family institution, as a basic pillar of society, as recognized by the UN in the Universal Declaration of Human Rights in its article 16.3 (84). Therefore, it is up to governments and politicians to shape family planning policies and contraceptive programs so that it is possible to maintain a healthy state of the family institution that is compatible with personal desires to limit the size of these families.
-
(84)resolución 217 ADeclaración Universal de Derechos Humanos, 1948
The question remains as to whether it is socially acceptable to facilitate, with public funding, the voluntary sterilization of individuals who have no family project to contribute to society.
The principle of equality on this point, understood as fairness in the distribution of risks and benefits, presents the difficulty of distinguishing who is equal, since there are differences of all kinds among men (85,86).
-
(85Comisión Nacional para la Protección de los sujetos humanos de investigación biomédica y del comportamiento. Informe Belmont. Principios y guías éticos para la protección de los sujetos humanos de investigación, 2023
-
86)Comisión Nacional para la Protección de los sujetos humanos de investigación biomédica y del comportamiento. Informe Belmont. Principios y guías éticos para la protección de los sujetos humanos de investigación, 2023
The application of the principle of justice should lead to an equitable selection of subjects to choose, within society, potential candidates to receive a free service.
e) Professional conscientious objection
It is increasingly common for people’s lifestyle, moral convictions, religious beliefs or ideology to conflict with legal duties, which is not alien to health professionals with respect to certain clinical indications.
In cases that fall within the scope of curative medicine, these situations must be assessed considering the risks involved in the procedure to be followed, as opposed to not performing it or performing it with the restrictive conditions that the patient wishes to impose on the physician.
The criterion to be followed is not always clear, but in general it can be accepted that the greater the risk, the lesser the physician’s obligation to follow the patient’s requests (87).
-
(87)Caso: solicitud de reversión de vasectomía en varón VIH con pareja serodiscordanteCuadernos de Bioética, 2016
Another element of the argument is when the treatment or procedure to be performed is futile, for example, when there are therapeutic alternatives to it or when it is not essential to solve the medical problem that has arisen (88,89).
-
(88La objeción de conciencia en el ámbito clínico. Propuesta para un uso apropiado (II)Revista de Calidad Asistencial, 2011
-
89)La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
In these situations, the physician’s refusal does not stem from a conflict between his conscience and the laws in force, but because he knows that he cannot engage in malpractice and must refuse these requests. It is therefore more a matter open to deliberation than a question of conscientious objection (90,91).
-
(90La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
-
91)La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
However, in the field of sexuality and reproduction, there are points of strong controversy (92,93). Thus, two concepts of sexuality and reproduction are opposed: when they are understood as two inseparable elements or if they are independent.
-
(92La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
-
93)La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
At the heart of this controversy are the concepts of reproductive health and reproductive rights recognized in the Program of Action of the Cairo Conference: rights of freedom and choice in the private sphere of the couple (94), as well as in Spain, in the Organic Law 2/2010 on sexual and reproductive health and the voluntary interruption of pregnancy (95).
-
(94)La objeción de conciencia de los profesionales sanitarios en la ética y deontologíaCuadernos de Bioética, 2010
-
(95)Ley Orgánica 2/2010, de 3 de marzo, de salud sexual y reproductiva y de la interrupción voluntaria del embarazoBOE, 2010
In this context, it should be recalled that voluntary sterilization is decriminalized in Spain, in article 156 of the Penal Code. From the legal point of view, it is considered an injury (art. 149 of the PC), which is not punishable if there is valid, free, conscious and express consent of the citizen.
This decriminalization reflects a social transformation that is favorable to guaranteeing the autonomy of patients and not punishing actions that do not conform to curative medicine, being framed in aspects of improvement or enhancement of health.
Notwithstanding the above, and even though it is a perfectly legal medical practice in Spain and as in other countries in our environment, included in the catalog of health benefits of the public health system, the physician, as well as other professionals who could collaborate in the vasectomy surgery, have recognized, constitutionally and legally, their right to conscientious objection, to the extent that, in the case we are analyzing, there are anthropological, moral and social elements, which could cause the health professionals to have ethical reservations or moral questions that would prevent them from agreeing to the request for sterilization by this young, autonomous and childless patient, without seriously compromising or contradicting their personal ethical, moral or religious convictions.
In this type of clinical cases, we understand that the requirements developed by the most authoritative legal doctrine (96) and by the jurisprudence of the Spanish Constitutional Court (97) are fulfilled so that the right to conscientious objection of health professionals must be guaranteed as a fundamental right in the corresponding medical-surgical services.
-
(96)opinión del Comité de Bioética de España sobre la objeción de conciencia en sanidad,
-
(97)BOE, 1987
11. Conclusions
From the bioethical point of view, we conclude that the fundamental point on which the problem is based is whether autonomy of will is the priority principle in the decision making process regarding voluntary sterilization.
The predominant criterion in the literature consulted on vasectomy is that family planning is a reproductive health right to which every individual with decision-making capacity should have free, voluntary, and unrestricted access.
Regarding the universality of the criteria applied for the performance of vasectomy according to the different schools of thought, the personalist theory and Catholic anthropology and bioethics disagree with the predominant criteria of other schools of thought, placing the integrity of the person before the principle of autonomy.
From the personalist perspective, and in the view of Catholic bioethics, autonomy, that is, having competence, maturity, and complete information, does not make the action licit, since the physician must seek the good of the patient and avoid maleficence, and must not go against his organism, mutilating a healthy part and altering its healthy function and bodily nature (98).
-
(98)Santo Padre Francisco. Exhortaciones Apostólicas,
In relation to the universality of the criteria applied for the performance of vasectomy, the ontologically based personalist bioethics current of thought prioritizes the integrity of the person over the principle of autonomy, which may differ from the predominant criteria in other currents of thought in bioethics.
Regarding legal aspects, voluntary sterilization is decriminalized in Spain, in article 156 of the Penal Code, where it is considered an injury (art. 149 of the PC), which is not punishable if there is valid, free, conscious, and express consent of the citizen.
Regarding the principle of autonomy, we have explained how nowadays, in pluralistic societies, in the request for vasectomy, it is understood that the autonomy of the individual’s decision must be respected and the interference of the professional’s personal criteria in the individual’s decision making should be avoided.
Regarding the negative social effects, it is recognized that it is difficult to carry out responsible parenthood without adequate means of contraception.
It is necessary to harmonize this vision of maternity/paternity with the support of the family institution, as the basic pillar of society. Governments are responsible for shaping family planning policies and contraceptive programs in such a way that it is possible to maintain a healthy state of the family institution that is compatible with personal desires to limit the size of these families.
Regarding the conscientious objection of health professionals, in this area of vasectomy, we conclude that it is appropriate because of the characteristics it presents:
As general conclusions regarding vasectomy and the specific case presented, of a request for vasectomy in a childless young man, we can affirm:
-
When deciding on sterilization, the patient’s autonomy should be respected, avoiding biases in the interpretation of the individual’s wishes, such as ethnicity, socioeconomic status, sexual orientation, age, and paternity.
-
Ample information should be provided on the risks and complications of vasectomy, especially those that remain long-term.
-
Information should be provided on the irreversibility of the procedure.
-
It should be clearly stated whether vasectomy reversal techniques are accessible and whether they are available free of charge.
-
Reversible contraceptive alternatives, some as effective as sterilization, should be widely reported.
-
In the case of requests made by very young or childless men, emphasis should be placed on providing information about the increased risk of subsequent regret.
-
Conscientious objection to vasectomy should be recognized both generally and cases because of the risk of regret. In these cases, the patient should be informed where his or her claim can be made.
-
In the case of free vasectomy, the authorities must clearly specify the criteria for individuals to access this service.
-
In short, even if vasectomy is legal, the physician can always refuse on conscientious objection, based on ethical grounds, since this practice implies going against the higher good of physical integrity without any therapeutic purpose, and doing so could be maleficent for that person.
Referencias
-
1Declaración Universal de Derechos Humanos. Asamblea General de la ONU, resolución 217 A, 10 de diciembre de 1948. Disponible en: http://www.un.org/es/universal-declaration-human-rights/index.html Links
-
21978 Alma-Ata Declaration - WHO | World Health Organization. Disponible en: https://www.who.int/teams/social-determinants-of-health/declaration-of-alma-ata#:~:text=International%20conference%20on%20primary%20health,goal%20of%20Health%20for%20All. Links
-
3Convención sobre la eliminación de todas las formas de discriminación contra la mujer [consultado 16 de octubre de 2023]. Disponible en: Disponible en: http://www.un.org/womenwatch/daw/cedaw/text/sconvention.htm Links
-
4Conferencia Internacional sobre la Población y el Desarrollo celebrada en El Cairo en 1994 [consultado 16 de octubre de 2023]. Disponible en: Disponible en: https://www.unfpa.org/sites/default/files/pub-pdf/icpd_spa.pdf Links
-
5Cuarta Conferencia Mundial sobre la Mujer en Beijing en 1995 [consultado 16 de octubre de 2023]. Disponible en: Disponible en: http://www.un.org/womenwatch/daw/beijing/pdf/ Beijing%20full%20report%20S.pdf Links
-
6Carmona H. Asociación de la satisfacción sexual en pacientes con vasectomía y sin vasectomía de 20 a 40 años adscritos en la UMF 93 [Tesis doctoral] Repositorio Institucional de la Universidad del Estado Autónomo de México. Disponible en: http://ri.uaemex.mx/handle/20.500.11799/111127 Links
-
7Pablo VI. Carta Encíclica Humanae Vitae, (7) [consultado 16 de octubre de 2023]. Disponible en: Disponible en: https://www.vatican.va/content/paul-vi/es/encyclicals/documents/ hf_p-vi_enc_25071968_humanae-vitae.html Links
-
8Fernandes J, Pizzi R. Aspectos ético-legales en la esterilización quirúrgica voluntaria. Revista de Obstetricia y Ginecología de Venezuela 2016; 76(3):196-202. Disponible en: https://ve.scielo.org/pdf/og/v76n3/art08.pdf Links
-
9Romero P, Merenciano FJ, Rafie W. La vasectomía: estudio de 300 intervenciones. Revisión de la literatura nacional y de sus complicaciones. Actas Urológicas Españolas 2004; 28(3):175-214. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0210-48062004000300002&lng=es&tlng=es Links
-
10Ramos-Salazar LV, Castañeda-Sánchez O, López-Ruiz EM. Factores biopsicosociales que influyen en la elección de la vasectomía. Aten Fam 2015; 22(3):8286. Disponible en: https://www.elsevier.es/es-revista-atencion-familiar-223-articulo-factores-biopsicosociales-que-influyen-eleccion-S1405887116300578 Links
-
11Romero P, Merenciano F J, Rafie W. La vasectomía: Estudio de 300 intervenciones. Revisión de la literatura nacional y de sus complicaciones. Actas Urológicas Españolas 2004; 28(3):175-214. Disponible en: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0210-48062004000300002&lng=es Links
-
12Ministerio de Sanidad de España. Subdirección General de Información Sanitaria. Registro de Actividad de Atención Especializada, RAE-CMBD [consultado 16 de octubre de 2023]. Disponible en: Disponible en: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SolicitudCMBD.htm Links
-
13Ministerio de Sanidad de España. Subdirección General de Información Sanitaria. Registro de Actividad de Atención Especializada, RAE-CMBD [consultado 16 de octubre de 2023]. Disponible en: Disponible en: https://www.sanidad.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SolicitudCMBD.htm Links
-
14Hospital Universitario Severo Ochoa, Leganés, Madrid. Unidad de Archivo y Codificación clínica . CMBD (conjunto mínimo básico de datos). Links
-
15Dohle G, Diemer T, Kopa C, Krausz C,Giwercman, A, Jungwirth, F. Guía clínica de la Asociación Europea de Urología sobre la vasectomía. https://doi.org/10.1016/j.acuroe.2012.08.012 Links
-
15-18Fernandes J, Pizzi R. Aspectos ético-legales en la esterilización quirúrgica voluntaria. Revista de Obstetricia y Ginecología de Venezuela. 2016; 76(3):196-202. Disponible en: https://ve.scielo.org/pdf/og/v76n3/art08.pdf Links
-
19Couceiro A, Seoane JA, Hernando P. La objeción de conciencia en el ámbito clínico. Propuesta para un uso apropiado (II) Revista de Calidad Asistencial. 2011; 26(5):320-324. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=3668438 Links
-
19-23Tena A, Azparren L, Donat, E. Estudio jurisprudencial en medicina satisfactiva. Revista Española de Medicina Legal. 2013; 39(4):162-167. Disponible en: https://www.elsevier.es/es-revista-revista-espanola-medicina-legal-285-articulo-estudio-jurisprudencial-medicina-satisfactiva-S0377473213000679 Links
-
24Lipshultz LI, Rumohr JA y Bennet RC. Técnicas de reversión de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed. Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona, 2009; 36 3):375-382. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=3306137 Links
-
25Kim HH, Goldstein M. Historia de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona. 2009; 36(3):359-375. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=3306126 Links
-
26Nagler HM, Jung H. Factores predictivos del éxito de la reversión microquirúrgica de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America. Barcelona, Elsevier. 2009; 36(3): 383-390. Disponible: https://revistasacademicas.cl/schu Links
-
26-29Robb P. y Sandlow J. Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona. 2009;36(3):391-396. http://biblioteca.solcaquito.org.ec:9997/handle/123456789/988 Links
-
30Sgreccia E. Bioética y esterilización. En Manual de Bioética. I Fundamentos y ética biomédica. Ed. Biblioteca de Autores Cristianos. Madrid 2009; 710-713. Links
-
30-35Sentencia 215/1994, de 14 de julio del Tribunal Constitucional español. Disponible en: https://hj.tribunalconstitucional.es/HJ/es/Resolucion/Show/2732 Links
-
36Ley 41/2002, de 14 de noviembre, básica reguladora de la autonomía del paciente y de derechos y obligaciones en materia de información y documentación clínica. BOE, 2022;(274). Links
-
36-40Seoane JA. El consentimiento en materia de bioética y biojurídica. La esterilización en el derecho español y en derecho comparado [Tesis doctoral]. Facultad de Derecho. A Links
-
41Selected practice recommendations for contraceptive use. WHO. 2016 [consultado 16 de febrero 2023]. Disponible en: https://iris.who.int/bitstream/handle/10665/252267/9789241565400-eng.pdf Links
-
42-43Benn P, Lupton M. Sterilisation of young, competent, and childless adults. British Medical Journal. 2005; 330:1323-1325. https://doi.org/10.1136/bmj.330.7503.1323 Links
-
44Comisión Nacional para la Protección de los sujetos humanos de investigación biomédica y del comportamiento. Informe Belmont. Principios y guías éticos para la protección de los sujetos humanos de investigación. EU [consultado 16 de febrero 2023]. Disponible en: Disponible en: http://www.bioeticayderecho.ub.edu/archivos/norm/ InformeBelmont.pdf Links
-
45Beauchamp, TL, Childress, JF. Principles of biomedical ethics. Oxford University Press, EU. 2001. Links
-
46Silva, J. Capacidad de moral e competencia jurídica para tomar uma decisâo autonómica. Conflitos Morais en Bioética Clínica. Recife. 2022; 27-39. Links
-
47Gafo J. Bioética teológica. Universidad Pontificia de Comillas, Madrid. 2003; 10. Links
-
48Sobre el principio de autonomía en la bioética. Ed. Abellán Salort, José Carlos. Bioética, autonomía y libertad. Fundación Universitaria Española, Madrid. 2007. Links
-
49Benn P, Lupton M. Sterilisation of young, competent, and childless adults. British Medical Journal. 2005; (330):1323-1325. https://doi.org/10.1136/bmj.330.7503.1323 Links
-
50Selected practice recommendations for contraceptive use. WHO. 2016 [consultado 16 de febrero 2023]. Disponible en: https://iris.who.int/bitstream/handle/10665/252267/9789241565400-webannex-eng.pdf?sequence=5 Links
-
51-54Diaz, E. De moralidad y eticidad. Dos dimensiones para la bioética. Acta Bioética 2002; (1):9-19. http://dx.doi.org/10.4067/S1726-569X2002000100002 http://dx.doi.org/10.4067/S1726-569X2002000100002 Links
-
54-60Adams CE, Wald M. Riesgos y complicaciones de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona. 2009; 36(3):331-336. Links
-
60-62Lipshultz LI, Rumohr JA y Bennet RC. Técnicas de reversión de la vasectomía. En Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed. Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona, 2009; 36 3):24. Links
-
63Nagler HM, Jung H. Factores predictivos del éxito de la reversión microquirúrgica de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America. Barcelona, Elsevier. 2009; 36(3): 383-390. Disponible: https://revistasacademicas.cl/schu Links
-
64Real Decreto-ley 16/2012, de 20 de abril, de medidas urgentes para garantizar la sostenibilidad del Sistema Nacional de Salud y mejorar la calidad y seguridad de sus prestaciones. (España) Jefatura del Estado. BOE 2012; (98). Disponible en: https://www.boe.es/eli/es/rdl/2012/04/20/16/con Links
-
65Robb P. y Sandlow J. Coste-efectividad de la reversión de la vasectomía. Vasectomía y reversión: aspectos importantes. Urologic Clinics of North America Ed Jay I Sandlow and Harris M. Nagler. Elsevier. Barcelona. 2009;36(3):391-396. http://biblioteca.solcaquito.org.ec:9997/handle/123456789/988 Links
-
65-68Sgreccia E. Bioética y esterilización. En Manual de Bioética. I Fundamentos y ética biomédica. Ed. Biblioteca de Autores Cristianos. Madrid 2009; 710-713. Links
-
69Gafo J. Bioética teológica.Universidad Pontificia de Comillas, Madrid. 2003; 10. Links
-
69-77Diaz, E. De moralidad y eticidad. Dos dimensiones para la bioética. Acta Bioética 2002; (1):9-19. http://dx.doi.org/10.4067/S1726-569X2002000100002 Links
-
77-79La Santa Sede. Congregación para la doctrina de la fe. Documentos de carácter doctrinal. Acerca de la esterilización en los hospitales católicos. 1975. Disponible en: https://www.vatican.va/roman_curia/congregations/cfaith/documents/rc_con_cfaith_doc_19750313_quaecumque-sterilizatio_sp.html Links
-
80Benatar, David. Better Never to Have Been: The Harm of Coming Into Existence. Oxford, Oxford University Press. 2006. Links
-
81-83Selected practice recommendations for contraceptive use. WHO. 2016 [consultado 16 de febrero 2023]. Disponible en: http://www.who.int/reproductivehealth/ publications/family_planning/SPR-3/en/ Links
-
84Declaración Universal de Derechos Humanos. Asamblea General de la ONU, resolución 217 A, 10 de diciembre de 1948. Disponible en: https://www.un.org/es/ about-us/universal-declaration-of-human-rights Links
-
84-86Comisión Nacional para la Protección de los sujetos humanos de investigación biomédica y del comportamiento. Informe Belmont. Principios y guías éticos para la protección de los sujetos humanos de investigación. EU [consultado 16 de febrero 2023]. Disponible en: http://www.bioeticayderecho.ub.edu/archivos/norm/ InformeBelmont.pdf Links
-
87Rascón J, Sandoica, E. Caso: solicitud de reversión de vasectomía en varón VIH con pareja serodiscordante. Cuadernos de Bioética. 2016; 27(3):425-427. https://www.redalyc.org/articulo.oa?id=87549410015 Links
-
88Couceiro A, Seoane JA y Hernando P. La objeción de conciencia en el ámbito clínico. Propuesta para un uso apropiado (II) Revista de Calidad Asistencial. 2011; 26(5):320-324. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=3668438 Links
-
82-94Martínez León, Mercedes; Rabadán Jiménez, José. La objeción de conciencia de los profesionales sanitarios en la ética y deontología. Cuadernos de Bioética. 2010 (2):199-210. Disponible en: https://dialnet.unirioja.es/servlet/articulo?codigo=3301305 Links
-
95Ley Orgánica 2/2010, de 3 de marzo, de salud sexual y reproductiva y de la interrupción voluntaria del embarazo. Jefatura del Estado. BOE. 2010; (55). Disponible en: https://www.boe.es/eli/es/lo/2010/03/03/2/con Links
-
96Comité de Bioética de España: opinión del Comité de Bioética de España sobre la objeción de conciencia en sanidad. Links
-
97Tribunal Constitucional. BOE. 1987; (271). Disponible en: https://hj.tribunalconstitucional.es/es-ES/Resolucion/Show/893#:~:text=%C2%ABLa%20Ley%20fijar%C3%A1%20las%20obligaciones,caso%2C%20una%20prestaci%C3%B3n%20 sustitutoria.%C2%BB Links
-
98La santa sede. Santo Padre Francisco. Exhortaciones Apostólicas. Disponible en: https://www.vatican.va/content/francesco/es/apost_exhortations/documents/papa-francesco_esortazione-ap_20160319_amoris-laetitia.htm Links