Review articles
Psychometric Properties of Tools for Assessing Spirituality: A Scoping Review
Propiedades psicométricas de las herramientas de evaluación de la espiritualidad: una revisión de alcance
Aya-Roa, Kevin J.1
 http://orcid.org/0000-0002-8430-0785
http://orcid.org/0000-0002-8430-0785
Beltrán-Campos, Vicente1*
http://orcid.org/0000-0001-8925-811X
García-Campo, María de Lourdes1
http://orcid.org/0000-0002-5406-5286
Vargas-Escobar, Lina María2
http://orcid.org/0000-0003-0052-5467
Hernández-Mariano, José Ángel3
http://orcid.org/0000-0003-0339-5610
http://orcid.org/0000-0002-8430-0785Beltrán-Campos, Vicente1*
http://orcid.org/0000-0001-8925-811XGarcía-Campo, María de Lourdes1
http://orcid.org/0000-0002-5406-5286Vargas-Escobar, Lina María2
http://orcid.org/0000-0003-0052-5467Hernández-Mariano, José Ángel3
http://orcid.org/0000-0003-0339-5610
-
Publication dates-
May 26, 2025
February , 2025
- Article in PDF
- Article in XML
- Automatic translation
- Send this article by e-mail
- Share this article +
Abstract
Background
The study of spirituality has gained importance, as it correlates with mental health and coping strategies, particularly at times of vulnerability. Spirituality could therefore contribute to the development of interventions to improve people’s quality of life. Experts often base the development of interventions and treatments on instruments measuring constructs such as spiritual well-being, which requires validated, reliable instruments.
Objective
This scoping review sought to summarize the evidence in the literature on the instruments available to assess spirituality in different groups and evaluate the content and psychometric properties of these instruments.
Method
A search was conducted on PubMed, Virtual Health Library (VHL), Elsevier, Springer, Scopus, and Google Scholar databases, using a combination of keywords such as “spirituality,” “validation study,” and “psychometrics.” The search was restricted to studies published in English and Spanish from January 2013 to March 2023.
Results
Sixty-four studies were included in this review. Two categories of analysis were established, the first being constructs related to spirituality and instruments for their measurement, in which a total of 22 conceptual constructs were found. The second was the validity and reliability of the instruments, in which it was found that most studies only assessed construct validity.
Discussion and conclusion
Given the complexity of the phenomenon, many instruments lack conceptual boundaries, resulting in similarities between items in instruments measuring different constructs. Determining the attributes and dimensions for the accurate measurement of spirituality is essential.
Keywords::
Spirituality, health surveys, psychometrics, review
BACKGROUND
As holistic beings, humans have multiple dimensions, including the physical, mental, social, and spiritual, the last of which develops differently in each individual (Morales Contreras & Palencia Sierra, 2021). Spirituality as a dimension allows one to not only connect with a belief system, a higher self, or whatever we consider divine but also with those around us and the environment (Fuentes et al., 2018). Spirituality transcends the intra-, inter-, and transpersonal dimensions of human beings. Despite being abstract, it is essential. Cultivating spirituality is important for people to achieve health and well-being (de Diego-Cordero et al., 2022). Individuals who fail to develop their spirituality fully or comprehensively may struggle to find life satisfaction (Caccia & Elgier, 2020).
-
Morales Contreras & Palencia Sierra, 2021Dimensión espiritual en el cuidado enfermeroEnfermería Investiga, 2021
-
Fuentes et al., 2018La Religiosidad y la Espiritualidad ¿Son conceptos teóricos independientes?Revista de Psicología, 2018
-
de Diego-Cordero et al., 2022The efficacy of religious and spiritual interventions in nursing care to promote mental, physical and spiritual health: A systematic review and meta-analysisApplied Nursing Research, 2022
-
Caccia & Elgier, 2020Resiliencia y satisfacción con la vida en adolescentes según nivel de espiritualidadPSOCIAL, 2020
Spirituality is a factor in achieving transcendence, which in turn leads to states of mental well-being in the individual (Reed, 2018, 2021) expressed through feelings of wholeness, meaning, fulfillment, and mental health (Reed & Haugan, 2021). Incorporating spiritual care into practice is therefore part of comprehensive, holistic care (Morales Contreras & Palencia Sierra, 2021).
-
Reed, 2018Theoryof self-transcendenceMiddle Range Theory for Nursing, 2018
-
2021Self-Transcendence: Moving from Spiritual Disequilibrium to Well-Being Across the Cancer TrajectorySeminars in Oncology Nursing, 2021
-
Reed & Haugan, 2021Self-Transcendence: A Salutogenic Process for Well-BeingHealth Promotion in Health Care – Vital Theories and Research, 2021
-
Morales Contreras & Palencia Sierra, 2021Dimensión espiritual en el cuidado enfermeroEnfermería Investiga, 2021
In this respect, it is essential to have valid, reliable measurement instruments with scientific, methodological rigor to enhance the practice of health professionals and research in this area. These instruments should be able to assess subjective attributes with complex dimensions for the health-disease process of the population and concepts as significant as spirituality (Muñiz & Fonseca-Pedrero, 2019).
-
Muñiz & Fonseca-Pedrero, 2019Diez pasos para la construcción de un testPsicothema, 2019
Measurement instruments delimit the definition of the concepts to distinguish them from others (Epstein et al., 2015). This facilitates the operationalization of variables and promotes coherence between concepts, constructs, dimensions, and items or empirical indicators (Herdman et al., 1998). Moreover, the design and validation of instruments for abstract phenomena unifies definitions according to a theoretical or conceptual point of reference, thereby avoiding using, misusing, or confusing similar terms and providing guidelines for developing new research (Sánchez-Villena et al., 2021).
-
Epstein et al., 2015A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensusJournal of Clinical Epidemiology, 2015
-
Herdman et al., 1998A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approachQuality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation, 1998
-
Sánchez-Villena et al., 2021Importancia de los estudios semánticos en la adaptación transcultural y validación de instrumentos de medida en Ciencias de la SaludEnfermería Clínica, 2021
Spirituality is increasingly being incorporated into clinical practice at various levels of care (Pagán-Torres, 2022). There are several measurement instruments assessing spirituality from different theoretical and philosophical perspectives. One example is Reed’s Self-Transcendence Scale, adapted to Spanish (Pena-Gayo et al., 2018) and based on the middle-range theory of self-transcendence. Another example is Piedmont’s Assessment of Spirituality and Religious Sentiments (ASPIRES) scale, which assesses spirituality through two dimensions: religious sentiments and spiritual transcendence. This scale is based on a psychological theory incorporating spirituality as a sixth factor within the five-factor model of personality (Simkin, 2017).
-
Pagán-Torres, 2022Abriendo nuevas puertas: Relevancia clínica de integrar la religión y la espiritualidad en la disciplina de la psicologíaRevista Puertorriqueña de Psicología, 2022
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
Spirituality has also been used as a dimension for assessing other phenomena essential to people’s well-being. For example, spiritual well-being is a factor in the Meaning in Life Questionnaire (Steger et al., 2006) used in clinical practice and research in palliative care (Schiappacasse Cocio & González Soto, 2016). Due to its abstract, multifaceted nature, spirituality poses challenges for its accurate, reliable measurement, making it essential to know the psychometric properties of the instruments designed and validated in the past ten years to measure this phenomenon. This review will enable us to identify the emerging concepts and definitions, the number of scales developed, the language, populations and cultures in which they have been validated, as well as the level of validity and reliability they present. It is therefore crucial to know what types of validation are most commonly used with these measurement instruments.
-
Steger et al., 2006The meaning in life questionnaire: Assessing the presence of and search for meaning in lifeJournal of Counseling Psychology, 2006
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
This scoping review seeks to contribute to clinical practice and health research by providing an exhaustive matrix that incorporates key elements for selecting the instruments to measure spirituality. This matrix would provide useful evidence for the decision-making of those who wish to use these instruments in both research and clinical practice in this field. Our objective was therefore to summarize the evidence in the literature on the instruments available to assess spirituality in various patient groups and to evaluate the contents and psychometric properties of these instruments.
METHOD
Study design
The following research is a scoping literature review, based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018). This review was conducted in five stages: 1) problem identification, based on a research question or guiding search question; 2) literature search in databases; 3) data evaluation; 4) data analysis, and 5) presentation of results.
-
Tricco et al., 2018PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and ExplanationAnnals of Internal Medicine, 2018
Problem identification
According to the stated objective, the following guiding question was suggested: What scales or instruments for assessing spirituality have been published in the literature in the past ten years with validity and reliability testing?
Literature search
A search of PubMed, Virtual Health Library (VHL), Elsevier, Springer, Scopus, and Google Scholar databases was conducted between January and March 2023. The DeCS/MeSH Health Science Descriptors “espiritualidad” AND (“estudios de validación” OR “psicometría”) were used in Spanish and “spirituality” AND (“validation study” OR “psychometrics”) in English.
Original research articles exploring the design, translation, adaptation and/or validation of instruments related to spirituality, published in Spanish or English between January 2013 and March 2023, and responding to the guiding question were included in the review process. Published articles that did provide a detailed description of the methodological process of designing, translating, adapting, and/or validating the instruments or the different types of validity (content, construct, criterion, convergent, discriminant) were excluded, as well as letters to the editor, conference abstracts, book chapters, and literature reviews.
Searching the databases using the descriptors yielded 16,119 studies. A total of 15,983 of these were then excluded after reading the title and abstract because they failed to meet the selection criteria, and 25 because they were duplicates. Afterwards, the full texts of 111 articles were read, and 36 studies were excluded because they failed to specify the methodological design related to validity testing (design, translation, adaptation and content, construct, criterion, convergent, or discriminant validity). Lastly, 64 studies were included in the scoping review, and eight were excluded for containing incomplete information on validity and reliability statistics. The entire selection process is presented in Figure 1.
Thumbnail
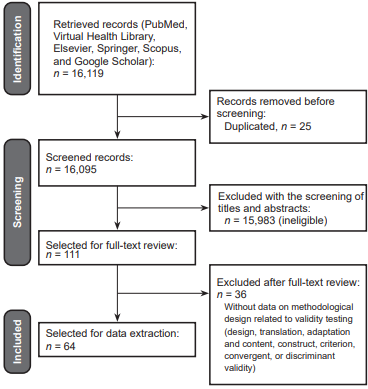
Figure 1
Flow Chart of the Selection Process of the Studies.
Flow Chart of the Selection Process of the Studies.
Data evaluation
Methodological quality was first assessed separately by the researchers and then by consensus. We began by reading the full text of the studies and then proceeded to rate the methodological quality individually using the COSMIN Risk of Bias checklist (Mokkink et al., 2018). The COSMIN checklist assesses methodological rigor and risk of bias according to the type of validity tested by the survey researchers. The appropriate boxes are filled in by study type to determine the overall quality of the study. The lowest score of each evaluated standard is used, using the “worst score counts” principle.
-
Mokkink et al., 2018COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome MeasuresQuality of life research, 2018
Data were summarized in a database created by the researchers, detailing the characteristics of the studies: database, authors, name of scale, country of validation, language of validation, language of publication, country of study, population, main concept of instrument, theoretical basis of concept, dimensions of concept or subscales, and validity and reliability. Results were analyzed, evaluated, and interpreted based on the planned objective and guiding search question. The researchers worked together to complete this process. Duplicates were discarded using Mendeley software (Elsevier © 2018).
Data analysis
After the reviewers’ quality assessment and selection of studies, the recommendations of PRISMA-ScR (2018) were followed. The first phase in data analysis was data reduction, which involved synthesizing the information found through an overall classification system. To this end, a matrix was created with the characteristics of the studies: database, authors, name of scale, country of validation, language of validation, language of publication, country of study, population, main concept of instrument, theoretical basis of concept, dimensions of concept or subscales, and validity and reliability.
The next phase of the data analysis was data display, which involved examining the display of the primary information sources to identify patterns, themes, and relationships. This enabled all the derived, defined, and validated constructs assessing spirituality in people to be identified. During the third phase, involving data comparison, the instruments were grouped according to the construct assessed, and some of the results found were compared, as well as the types of validity testing among the instruments. As a result of these two phases, two essential contents or categories were identified that will be presented in the following section: constructs related to spirituality and their measurement scales and the validity and reliability of the instruments or scales for assessing spirituality. During the final phase, we drew and verified conclusions. We then condensed the main elements and arrived at overall conclusions that are useful for both practice and research.
RESULTS
General Description of Studies
Table 1 describes the characteristics of the measurement instruments or scales reviewed. Validated measurement instruments were mostly found in Asian and Middle Eastern countries (31%, n = 20), such as China, Iran, India, Taiwan, Turkey, Israel, Jordan, and South Korea, and European ones (28%, n = 18), such as Poland, Italy, Portugal, Germany, Slovakia, Spain, France, Ireland, the United Kingdom, and Sweden. Twenty percent of the instruments (n = 13) were validated in South and Central American countries such as Brazil, Argentina, Chile, Colombia, Peru, and Puerto Rico, and 17% (n = 11) in North American countries, mainly the United States and Mexico. Only two multicenter studies were identified (4%). Regarding the language of publication, 83% (n = 53) of the articles reviewed were published in English and 17% (n = 11) in Spanish.
Table 1
Characteristics of the Measurement Instruments or Scales Found in the Integrative Review
Characteristics of the Measurement Instruments or Scales Found in the Integrative Review
| Authors/year | Scale title |
Country of |
Language of |
Language of |
Population |
|---|---|---|---|---|---|
| Adib & Zehtabchi, 2016 | Instrument to assess nurses’ professional competence in spiritual care | Iran | Farsi | English | Nurses |
| Agli et al., 2017 | Functional Assessment of Chronic Illness Therapy—Spiritual Well- |
France | French | English | Older adults in nursing |
| Ahmad et al., 2022 | Functional Assessment of Chronic Illness Therapy-Spiritual Well-Being |
USA | English | English | Adults with life-limiting |
|
Becerra Canales & Becerra
|
Escala de inteligencia espiritual en la práctica sanitaria (EIEps) | Peru | Spanish | Spanish | Healthcare workers |
| Benito et al., 2014 | Cuestionario GES (Grupo Espiritualidad SECPAL) | Spain | Spanish | English | Palliative care patients |
| Berger et al., 2016 | Multidimensional Inventory for Religious/Spiritual Well-Being (MI- |
Mexico | Spanish | English | Nursing students |
| Burke et al., 2013 | Inventory of Complicated Spiritual Grief (ICSG) | USA | English | English | Christian adults and |
| Burke et al., 2021 | Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0) | USA | English | English | Adults |
| Büssing et al., 2016 | Polish version of Spiritual and Religious Attitudes in Dealing with |
Poland | Polish | English | Adults with chronic |
|
Schiappacasse Cocio &
|
Meaning in Life Scale (MILS) | Latin-American | Spanish | English | Cancer patients receiving |
| Daaleman et al., 2014 | Quality of Spiritual Care (QSC) scale | USA | English | English | Family caregivers |
| Deluga et al., 2020 | Spiritual Attitude and Involvement List (SAIL) | Poland | Polish | English | Nurses |
| Deng et al., 2021 | Functional Assessment of Chronic Illness Therapy—Spiritual Well- |
USA | English | English | Heart failure patients |
| Díaz-Castillo et al., 2021 | Escala Trifactorial de Espiritualidad | Mexico | Spanish | Spanish | Older adults |
| Elhai et al., 2018 | SHALOM Spiritual Questionnaire | Israel | Hebrew | Spanish | Adults |
| Erci & Aktürk, 2018 | System of Belief Inventory | Turkey | Turkish | English | Cancer patients |
| Feng et al., 2019 | Spiritual Intelligence Scale-Chinese Form | China | Mandarin | English | Students and adults |
| Feng et al., 2021 | Chinese Spiritual Coping Scale |
China | Mandarin | English | Adults |
|
Fopka-Kowalczyk et al.,
|
Spiritual Supporter (SpSup) Scale | Poland | Polish | English | Medical students |
| Gallardo-Peralta et al., 2018 | Índice Breve de Religiosidad y Espiritualidad | Chile | Spanish | Spanish | Older adults |
| Gallegos et al., 2021 | System of Beliefs Inventory (SBI-15R) | Peru | Spanish | English | Adults |
| Głaz, 2021 | Scale of Abandonment by God (SAG) | Poland | Polish | English | University students |
| Gonçalves et al., 2016 | Treatment Spirituality / Religiosity Scale (TSRS) | Brazil | Portuguese | English | Nursing students |
|
González-Rivera & Pagán-
|
Inventario de Estrategias de Afrontamiento Religioso (IEAR) | Puerto Rico | Spanish | Spanish | Adults |
|
González-Rivera, Veray-
|
Escala de Espiritualidad Personal (EPP) | Puerto Rico | Spanish | Spanish | Adults |
| González-Rivera, et al., 2018 | Escala de espiritualidad de Delaney | Puerto Rico | Spanish | Spanish | Adults |
| Guilherme et al., 2020 | Spiritual Care Competence Scale (SCCS) | Brazil | Portuguese | English | Nursing students |
| Hu et al., 2019 | Chinese version of the Spiritual Care Competence Scale (C-SCCS) | China | Mandarin | English | Nurses |
| İpek et al., 2017 | Spiritual Care-Giving Scale | Turkey | Turkish | English | Nursing students |
| Kabakci et al., 2022 | Spiritual Care Competence Scale (SCCS) | Turkey | Turkish | English | Midwives |
| Kang et al., 2022 | Korean version of the Nurse Spiritual Care Therapeutics Scale |
South Korea | Korean | English | Nurses |
| Levine et al., 2015 | Spiritual support subscale for the Medical Outcomes Study Social |
USA | English | English | Cancer survivors |
| Lin et al., 2015 | Chinese version of the Spiritual Interests Related Illness Tool |
Taiwan | Mandarin | English | Adults |
| Lo et al., 2016 | Daily Spiritual Experiences Scale–Chinese (DSES-C) | USA | English | English | Cancer patient |
| Lundman et al., 2015 | Swedish version of Self-Transcendence Scale | Sweden | Swedish | English | Older adults |
| Makkar & Singh, 2021 | Spirituality Measurement Scale (SMS) | India | Hindi | English | University students |
| Martins et al., 2021 | Validation of Duke University Religion Index (P-DUREL) | Portugal | Portuguese | English | Cancer patients receiving |
| Moeini et al., 2018 | Spiritual Needs Questionnaire (SpNQ). | Iran | Farsi | English | Elders with chronic |
| Nawafleh et al., 2018 | Spiritual Questionnaire | Jordan | Arabic | English | University students |
| Nooripour et al., 2023 | Spiritual Well-being Scale (SWBS) | Iran | Farsi | English | Older adults |
| Oñate et al., 2015 | Breve evaluación multidimensional de la religiosidad y la espiritualidad | Argentina | Spanish | Spanish | Young adults |
| Pais et al., 2022 | Spirituality and Spiritual Care Rating Scale (SSCRS) | India | Hindi | English | Nurses |
| Pastrana et al., 2021 | Spiritual Care Competence Questionnaire (SCCQ) | Argentina, |
Spanish | English | Healthcare professionals |
| Pena-Gayo et al., 2018 | Escala de autotrascendencia | Spain | Spanish | Spanish | Adults |
| Pinto et al., 2016 | Portuguese End of Life Spiritual Comfort Questionnaire | Portugal | Portuguese | English | Palliative care patients |
| Proyer & Laub, 2017 | Expressions of Spirituality Inventory-Revised (ESI-R) | Germany | German | English | Adults |
| Rabitti et al., 2020 | Functional Assessment of Chronic Illness Therapy-Spiritual (FACIT-Sp) | Italy | Italian | English | Cancer patients |
| Riveros et al., 2018 | Inventario de Sistema de Creencias (SBI-15 R) | Colombia | Spanish | Spanish | University student and |
| Roof et al., 2017 | Spiritual Engagement Instrument (SpEI) | USA | English | English | Adults |
| Saffari et al., 2017 | Daily Spiritual Experiences Scale (DSES) | Iran | Farsi | English | Pregnant women |
| Simão et al., 2016 | Spiritual Distress Scale | Brazil | Portuguese | English | Cancer patients |
| Simkin, 2017 | Escala de evaluación de espiritualidad y sentimientos religiosos |
Argentina | Spanish | Spanish | University students |
| Soósová & Mauer, 2021 | Daily Spiritual Experience Scale (DSES) | Slovakia | Slovak | English | Older adults |
| Tomás & Rosa, 2021 | Scale of Religious and Spiritual Coping (RCOPE) | Portugal | Portuguese | English | Adults |
| Vespa et al., 2017 | Brief Multidimensional Measure of Religiousness/Spirituality (BMMRS) | Italy | Italian | English | Older adults |
| Wang et al., 2022 | Spiritual Enlightenment Experience Scale (SEES) | China | Mandarin | English | Adults |
| Watts et al.,2022 | Watts Connectedness Scale (WCS) | UK | English | English | Adults |
| Weathers et al., 2020 | Spirituality Instrument 27 (SpI-27©) | Ireland | Irish | English | Chronic disease patients |
| White & Schim, 2013 | Spiritual Self-Care Practices Scale (SSCPS) | USA | English | English | Patients with heart failure |
| Wu et al., 2016 | Spiritual Care Needs Inventory (SCNI) | Taiwan | Mandarin | English | Hospitalized adults |
| Xie et al., 2019 | Nurse Spiritual Therapeutics Scale (NSTS) | China | Mandarin | English | Cancer patients |
| Yepes Martinez et al., 2023 | The Italian version of the Daily Spiritual Experience Scale (DSES-IT) | Italy | Italian | English | Patients with psychiatric |
| Zhao et al., 2019 | Chinese version of the Spiritual Needs Questionnaire with 27 items |
China | Mandarin | English | Cancer patients |
-
Adib & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Agli et al., 2017Validation of the Functional Assessment of Chronic Illness Therapy—Spiritual Well-being (FACIT-Sp12) on French Old PeopleJournal of Religion and Health, 2017
-
Ahmad et al., 2022The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnessesAnnals of Palliative Medicine, 2022
-
Becerra Canales & BecerraDiseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Huaman, 2020Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Benito et al., 2014Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care PatientsJournal of Pain and Symptom Management, 2014
-
Berger et al., 2016The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Burke et al., 2013Inventory of Complicated Spiritual Grief: Development and Validation of a New MeasureDeath Studies, 2013
-
Burke et al., 2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Büssing et al., 2016Spiritual and Religious Attitudes in Dealing with Illness in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK QuestionnaireJournal of Religion and Health, 2016
-
Schiappacasse Cocio &Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Daaleman et al., 2014Development and Preliminary Testing of the Quality of Spiritual Care ScaleJournal of Pain and Symptom Management, 2014
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
Deng et al., 2021Two Factor Structures Possible for the FACIT-Sp in Patients With Heart FailureJournal of Pain and Symptom Management, 2021
-
Díaz-Castillo et al., 2021Desarrollo y validación de la Escala Trifactorial de Espiritualidad en personas adultas mayores mexicanasNeurama, 2021
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Erci & Aktürk, 2018The System of Belief Inventory: A Validation Study in Turkish Cancer PatientsJournal of religion and health, 2018
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
Feng et al., 2021The Chinese Spiritual Coping Scale: Development and Initial Psychometric EvaluationJournal of religion and health, 2021
-
Fopka-Kowalczyk et al.,The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
2023The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
Gallardo-Peralta et al., 2018Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayoresRevista de Psicología, 2018
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
Gonçalves et al., 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
González-Rivera & Pagán-Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
Torres, 2018Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
González-Rivera, Veray-Desarrollo, validación y descripción teórica de la escala de espiritualidad personal en una muestra de adultos en Puerto RicoRevista Puertorriqueña de Psicología, 2017
-
Alicea, et al., 2017Desarrollo, validación y descripción teórica de la escala de espiritualidad personal en una muestra de adultos en Puerto RicoRevista Puertorriqueña de Psicología, 2017
-
González-Rivera, et al.,Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
İpek et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Kabakci et al., 2022Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence ScaleCentral European Journal of Nursing and Midwifery, 2022
-
Kang et al., 2022Nurse Spiritual Care Therapeutics Scale: Validation Among Nurses Who Care for Patients With Life-Threatening Illnesses in South KoreaJournal of hospice and palliative nursing,, 2022
-
Levine et al., 2015Development and Initial Validation of a Spiritual Support Subscale for the MOS Social Support SurveyJournal of Religion and Health, 2015
-
Lin et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Lundman et al., 2015Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old PeopleJournal of Nursing Measurement, 2015
-
Makkar & Singh, 2021Development of a spirituality measurement scaleCurrent Psychology, 2021
-
Martins et al., 2021Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing ChemoterapyJournal of Religion and Health, 2021
-
Moeini et al., 2018Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
Nooripour et al., 2023Validation of the Spiritual Well-being Scale (SWBS) and its role in Predicting Hope among Iranian ElderlyAgeing International, 2023
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Pinto et al., 2016Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patientsPorto Biomedical Journal, 2016
-
Proyer & Laub, 2017The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Rabitti et al., 2020The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions?BMC Palliative Care, 2020
-
Riveros et al., 2018Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicosRevista Colombiana de Enfermería, 2018
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Saffari et al., 2017Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental HealthJournal of Religion and Health, 2017
-
Simão et al., 2016Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
-
Soósová & Mauer, 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Vespa et al., 2017Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
-
Wang et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Watts et al.,2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Weathers et al., 2020Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illnessApplied Nursing Research, 2020
-
White & Schim, 2013Development of a Spiritual Self-Care Practice ScaleJournal of Nursing Measurement, 2013
-
Wu et al., 2016Persistent Organic Pollutants and Type 2 Diabetes: A Prospective Analysis in the Nurses’ Health Study and Meta-analysisEnvironmental Health Perspectives, 2013
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
-
Yepes Martinez et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
Constructs Related to Spirituality and its Measurement Scales
In the present review, 22 conceptual constructs were identified that assess spirituality or some aspect of the latter. These constructs are shown in Table 2. The construct related to spirituality with the largest number of instruments is spiritual care or spiritual care competence, with a total of ten instruments. In general, these scales assess the level of spiritual care or the ability of nurses or other healthcare professionals to provide spiritual care (Adib-Hajbaghery & Zehtabchi, 2016; Benito et al., 2014; Daaleman et al., 2014; Guilherme et al., 2020; Hu et al., 2019; İpek Çoban et al., 2017; Kabakci et al., 2022; Pais et al., 2022; Pastrana et al., 2021; Xie et al., 2019). According to the operational definitions and constructs of these instruments, spiritual care competence is defined as the ability of nurses or health professionals to identify spiritual needs and to plan and implement care plans, activities or interventions that enhance the spiritual dimension of the subject of care (Adib-Hajbaghery & Zehtabchi, 2016; Benito et al., 2014; Daaleman et al., 2014; Guilherme et al., 2020; Hu et al., 2019; İpek Çoban et al., 2017; Kabakci et al., 2022; Pais et al., 2022; Pastrana et al., 2021; Wang et al., 2022; Xie et al., 2019).
-
Adib-Hajbaghery & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Benito et al., 2014Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care PatientsJournal of Pain and Symptom Management, 2014
-
Daaleman et al., 2014Development and Preliminary Testing of the Quality of Spiritual Care ScaleJournal of Pain and Symptom Management, 2014
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
İpek Çoban et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Kabakci et al., 2022Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence ScaleCentral European Journal of Nursing and Midwifery, 2022
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
-
Adib-Hajbaghery & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Benito et al., 2014Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care PatientsJournal of Pain and Symptom Management, 2014
-
Daaleman et al., 2014Development and Preliminary Testing of the Quality of Spiritual Care ScaleJournal of Pain and Symptom Management, 2014
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
İpek Çoban et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Kabakci et al., 2022Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence ScaleCentral European Journal of Nursing and Midwifery, 2022
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Wang et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
Table 2
Constructs related to spirituality and its validated scales
Constructs related to spirituality and its validated scales
|
Constructs related to |
Definition | Validated scales |
|---|---|---|
| Religious and |
Religious coping refers to cognitive, behavioral, and interpersonal |
Scale of Religious and Spiritual Coping (RCOPE) |
| Spiritual and |
Operational definition not reported. | Spiritual and Religious Attitudes in Dealing with |
| Self-transcendence | Human skill to expand one’s limits in the interpersonal (with others), |
Reed’s Self-Transcendence Scale |
| Spiritual distress | A time in life when a person experiences profound discord or |
Spiritual Distress Scale (Simão et al., 2016) |
| Spiritual self-care | Spiritual self-care refers to the way people relate to their subjectivity, |
Spiritual Self-Care Practices Scale (SSCPS) |
| Spiritual support | The operational definition was not reported in the included |
Spiritual support subscale for the Medical |
| Spiritual well- |
A comprehensive sense of meaning and purpose in life, harmony and |
Functional Assessment of Chronic Illness |
| Spiritual care |
Spiritual care competence is the systematic care nurses provide to |
Spiritual Care Competence Scale (SCCS) |
| Spiritual/religious |
Participation and practices in religious or spiritual activities with |
Validation of the Duke University Religion |
| Connectedness | Connectedness is a state characterized by the presence of feelings of |
Watts Connectedness Scale (WCS) |
| Spiritual comfort | The operational definition was not reported in the included manuscripts. | Portuguese End-of-Life Spiritual Comfort |
| Religious beliefs | The concept was not clearly defined in the studies. Several definitions |
System of Beliefs Inventory (SBI-15R) |
| Spiritual grief | Spiritual grief is a spiritual crisis during grief that includes the collapse |
Inventory of Complicated Spiritual Grief (ICSG) |
| Spirituality | Subjective, mystical, and holistic interpretation of personal beliefs and |
Spirituality Measurement Scale (SMS) |
| Spirituality / |
According to Vespa et al. (2017), spirituality is the personal and |
Treatment Spirituality / Religiosity Scale (TSRS) |
| Spiritual or |
Specific feelings, transcendental growth processes, and effects that |
Daily Spiritual Experiences Scale (DSES) |
| Expressions of |
Expressions of spirituality refer to the manifestations and ways in |
Expressions of Spirituality Inventory-Revised |
| Spiritual |
Mental skills that address existential, transcendental, and conscious |
Escala de inteligencia espiritual en la práctica |
| Spiritual needs | Requirements related to the spirituality of patients, particularly in the |
Spiritual Needs Questionnaire (SpNQ) |
| Spiritual health | Spiritual health refers to the dynamic state of being, which reflects |
SHALOM Spiritual Questionnaire |
| Feelings of |
A common subjective experience among religious people in that, |
Scale of Abandonment by God (SAG) |
| Spirituality- |
Innate motivation to guide behavior in the effort to build a deeper |
Escala de evaluación de espiritualidad y |
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Feng et al., 2021The Chinese Spiritual Coping Scale: Development and Initial Psychometric EvaluationJournal of religion and health, 2021
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Feng et al., 2021The Chinese Spiritual Coping Scale: Development and Initial Psychometric EvaluationJournal of religion and health, 2021
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Büssing et al., 2016Spiritual and Religious Attitudes in Dealing with Illness in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK QuestionnaireJournal of Religion and Health, 2016
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
Pena- Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Lundman et al., 2015Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old PeopleJournal of Nursing Measurement, 2015
-
Simão et al., 2016Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
Simão et al., 2016Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
White & Schim, 2013Development of a Spiritual Self-Care Practice ScaleJournal of Nursing Measurement, 2013
-
White & Schim, 2013Development of a Spiritual Self-Care Practice ScaleJournal of Nursing Measurement, 2013
-
Levine et al., 2015Development and Initial Validation of a Spiritual Support Subscale for the MOS Social Support SurveyJournal of Religion and Health, 2015
-
Fopka et al., 2023The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
Rabitt et al., 2020The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions?BMC Palliative Care, 2020
-
Agli et al., 2017Validation of the Functional Assessment of Chronic Illness Therapy—Spiritual Well-being (FACIT-Sp12) on French Old PeopleJournal of Religion and Health, 2017
-
Rabitt et al., 2020The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions?BMC Palliative Care, 2020
-
Ahmad et al., 2022The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnessesAnnals of Palliative Medicine, 2022
-
Deng et al., 2021Two Factor Structures Possible for the FACIT-Sp in Patients With Heart FailureJournal of Pain and Symptom Management, 2021
-
Nooripour et al., 2023Validation of the Spiritual Well-being Scale (SWBS) and its role in Predicting Hope among Iranian ElderlyAgeing International, 2023
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Adib-Hajbaghery & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Adib-Hajbaghery & Zehtabchi 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Kabakci & Çelik, 2022Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence ScaleCentral European Journal of Nursing and Midwifery, 2022
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
-
İpek et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Daaleman et al., 2014Development and Preliminary Testing of the Quality of Spiritual Care ScaleJournal of Pain and Symptom Management, 2014
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Benito et al., 2014Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care PatientsJournal of Pain and Symptom Management, 2014
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Martins et al., 2021Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing ChemoterapyJournal of Religion and Health, 2021
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Watts et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Watts et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Pinto et al., 2016Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patientsPorto Biomedical Journal, 2016
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
Riveros et al., 2018Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicosRevista Colombiana de Enfermería, 2018
-
Burke et al., 2014Inventory of Complicated Spiritual Grief: Development and Validation of a New MeasureDeath Studies, 2013
-
2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Burke et al., 2014Inventory of Complicated Spiritual Grief: Development and Validation of a New MeasureDeath Studies, 2013
-
Burke et al., 2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
González-Rivera, Veray- Alicea, et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera et al., 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Makkar et al., 2021Development of a spirituality measurement scaleCurrent Psychology, 2021
-
Weathers et al., 2020Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illnessApplied Nursing Research, 2020
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
González-Rivera, Veray- Alicea, et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera et al., 2018Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
González-Rivera, Quintero- Jiménez, et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Vespa et al. (2017)Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
-
Oñate et al. (2015)Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Gonçalves et al. 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
Berger et al., 2016The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Vespa et al., 2017Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Gallardo-Peralta et al.,2018Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayoresRevista de Psicología, 2018
-
Díaz-Castillo et al., 2021Desarrollo y validación de la Escala Trifactorial de Espiritualidad en personas adultas mayores mexicanasNeurama, 2021
-
Erci, & Aktürk, 2018The System of Belief Inventory: A Validation Study in Turkish Cancer PatientsJournal of religion and health, 2018
-
Soósová & Mauer, 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Wang et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Saffari et al., 2017Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental HealthJournal of Religion and Health, 2017
-
Soósová & Mauer, 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Yepes Martinez et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
-
Wang et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Proyer & Laub, 2017The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Proyer & Laub, 2017The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Becerra Canales & Becerra Huaman, 2020Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Becerra Canales & Becerra Huaman, 2020Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
Moeini et al., 2018Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
-
Moeini et al., 2018)Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
-
Wu et al., 2016)Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in TaiwanClinical Nursing Research, 2016
-
Lin et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
Another construct with the largest number of instruments found was spirituality from a theocentric perspective (spirituality/religiosity), with eight instruments (Berger et al., 2016; Erci & Aktürk, 2018; Gallardo-Peralta et al., 2018; Gonçalves et al., 2016; Oñate et al., 2015; Simkin, 2017; Vespa et al., 2017). These scales are striking because they include dimensions such as the connection to God or a higher power and transcendental phenomena such as death (Berger et al., 2016; Díaz-Castillo et al., 2021; Gallardo-Peralta et al., 2018; Gonçalves et al., 2016; Vespa et al., 2017). Items in these dimensions address the most common religious practices, such as prayer, meditation, fasting, and the reading of sacred books, and would be the empirical indicators of the connection with God.
-
Berger et al., 2016The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Erci & Aktürk, 2018The System of Belief Inventory: A Validation Study in Turkish Cancer PatientsJournal of religion and health, 2018
-
Gallardo-Peralta et al., 2018Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayoresRevista de Psicología, 2018
-
Gonçalves et al., 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
-
Vespa et al., 2017Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
-
Berger et al., 2016The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Díaz-Castillo et al., 2021Desarrollo y validación de la Escala Trifactorial de Espiritualidad en personas adultas mayores mexicanasNeurama, 2021
-
Gallardo-Peralta et al., 2018Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayoresRevista de Psicología, 2018
-
Gonçalves et al., 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
Vespa et al., 2017Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
Some instruments assess spirituality as a broad, holistic, multi-dimensional concept. Seven measurement instruments were found that assess spirituality from multiple perspectives and had been validated in different populations. One of the most outstanding features of these instruments is that they have subscales assessing three or more dimensions of spirituality, such as intrapersonal, extrapersonal, and transpersonal connections (González-Rivera & Pagán-Torres, 2018; González-Rivera, Quintero-Jiménez et al., 2017; González-Rivera, Veray-Alicea, et al., 2017; Makkar & Singh, 2021; Nawafleh et al., 2018; Schiappacasse Cocio & González Soto, 2016; Weathers et al., 2020; González-Rivera, et al., 2018).
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
González-Rivera, Quintero-Jiménez et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera, Veray-Alicea, et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
Makkar & Singh, 2021Development of a spirituality measurement scaleCurrent Psychology, 2021
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Weathers et al., 2020Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illnessApplied Nursing Research, 2020
-
González-Rivera, et al., 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
Spirituality as a holistic dimension has conceptually abstract dimensions, such as meaning (Deluga et al., 2020; González-Rivera & Pagán-Torres, 2018) and self-awareness (Weathers et al., 2020), in some of the instruments reviewed. Spiritual needs are another construct identified (Lin et al., 2015;Moeini et al., 2018; Wu et al., 2016; Zhao et al., 2019). These instruments are designed for people who require spiritual care. Although identifying spiritual needs can be extremely useful, this review did not identify any scales available in Spanish or validated in Spanish-speaking countries that addressed spiritual needs.
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Weathers et al., 2020Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illnessApplied Nursing Research, 2020
-
Lin et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Moeini et al., 2018Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Wu et al., 2016Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in TaiwanClinical Nursing Research, 2016
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
The definitions provided in the instruments (Lin et al., 2015; Moeini et al., 2018; Wu et al., 2016; Zhao et al., 2019) suggest that spiritual needs are what people must satisfy to fully develop spirituality or any of its dimensions.
-
Lin et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Moeini et al., 2018Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Wu et al., 2016Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in TaiwanClinical Nursing Research, 2016
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
The spiritual and religious experiences construct (Lo et al., 2016; Saffari et al., 2017; Soósová & Mauer, 2021; Wang et al., 2022; Yepes Martinez et al., 2023) assesses spirituality and religiosity from multiple perspectives, including intrapersonal aspects such as meaning, peace, and faith (Saffari et al., 2017), religiosity (Lo et al., 2016; Soósová & Mauer, 2021; Yepes Martinez et al., 2023) and attention to spiritual needs (Wang et al., 2022; Yepes Martinez et al., 2023).
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Saffari et al., 2017Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental HealthJournal of Religion and Health, 2017
-
Soósová & Mauer, 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Wang et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Yepes Martinez et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
-
Saffari et al., 2017Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental HealthJournal of Religion and Health, 2017
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Soósová & Mauer, 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Yepes Martinez et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
-
Wang et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Yepes Martinez et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
Other constructs assessing spirituality found were religious and spiritual coping (Feng et al., 2019; González-Rivera & Pagán-Torres, 2018; Tomás & Rosa, 2021), spiritual and religious attitudes (Büssing et al., 2016; Deluga et al., 2020), self-transcendence (Lundman et al., 2015; Pena-Gayo et al., 2018), spiritual distress (Simão et al., 2016), spiritual self-care (White & Schim, 2013), spiritual support (Fopka-Kowalczyk et al., 2023; Levine et al., 2015), spiritual well-being (Agli et al., 2017; Ahmad et al., 2022; Deng et al., 2021; Nooripour et al., 2023; Rabitti et al., 2020), spiritual and/or religious engagement (Martins et al., 2021; Roof et al., 2017), connectedness (Watts et al., 2022), spiritual comfort (Pinto et al., 2016), religious beliefs (Gallegos et al., 2021; Riveros et al., 2018), spiritual grief (Burke et al., 2013, 2021), spiritual and/or religious expressions (Proyer & Laub, 2017), spiritual intelligence (Becerra Canales & Becerra Huaman, 2020; Feng et al., 2019), feelings of abandonment by God (Głaz, 2021), and spiritual transcendence (Simkin, 2017).
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Büssing et al., 2016Spiritual and Religious Attitudes in Dealing with Illness in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK QuestionnaireJournal of Religion and Health, 2016
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
Lundman et al., 2015Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old PeopleJournal of Nursing Measurement, 2015
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Simão et al., 2016Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
White & Schim, 2013Development of a Spiritual Self-Care Practice ScaleJournal of Nursing Measurement, 2013
-
Fopka-Kowalczyk et al., 2023The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
Levine et al., 2015Development and Initial Validation of a Spiritual Support Subscale for the MOS Social Support SurveyJournal of Religion and Health, 2015
-
Agli et al., 2017Validation of the Functional Assessment of Chronic Illness Therapy—Spiritual Well-being (FACIT-Sp12) on French Old PeopleJournal of Religion and Health, 2017
-
Ahmad et al., 2022The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnessesAnnals of Palliative Medicine, 2022
-
Deng et al., 2021Two Factor Structures Possible for the FACIT-Sp in Patients With Heart FailureJournal of Pain and Symptom Management, 2021
-
Nooripour et al., 2023Validation of the Spiritual Well-being Scale (SWBS) and its role in Predicting Hope among Iranian ElderlyAgeing International, 2023
-
Rabitti et al., 2020The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions?BMC Palliative Care, 2020
-
Martins et al., 2021Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing ChemoterapyJournal of Religion and Health, 2021
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Watts et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Pinto et al., 2016Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patientsPorto Biomedical Journal, 2016
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
Riveros et al., 2018Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicosRevista Colombiana de Enfermería, 2018
-
Burke et al., 2013Inventory of Complicated Spiritual Grief: Development and Validation of a New MeasureDeath Studies, 2013
-
2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Proyer & Laub, 2017)The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Becerra Canales & Becerra Huaman, 2020Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
Of the 22 concepts related to spirituality, four were found to lack clear operational definitions in the psychometric studies reviewed. Most of these studies presented multiple theoretical definitions of spirituality and religiosity, highlighting both the differences between constructs and their shared defining characteristics. However, many of these studies lacked a precise definition of the phenomenon they aimed to measure using a solid theoretical or empirical reference, revealing a possible conceptual confusion between the construct of spirituality and emerging concepts such as spiritual and religious attitudes, spiritual support, spiritual comfort and religious beliefs.
We identified three concepts that might seem similar: spiritual distress, spiritual pain, and feelings of abandonment by God. While the definition of these concepts suggests that people may experience a loss in their relationship with God or a transpersonal disconnection at some point, they are distinguished by their conceptual boundaries. Spiritual pain is linked to grief, whereas spiritual distress focuses on an internal conflict related to beliefs and values. Conversely, feelings of abandonment by God refer to the perception of a temporary separation from God for no clear reason. However, this feeling is part of the process of spiritual growth.
Although most of the concepts are understandable, most of the definitions found in psychometric studies are not consistent with the dimensions of the instruments used. Moreover, in many studies involving the translation and cultural adaptation of instruments to measure spirituality, the researcher’s original definition of the instrument was not clarified, making it difficult to conduct an exhaustive analysis of the validity of the construct in these contexts.
Validity and Reliability of the Instruments or scales for the Assessment of Spirituality
The populations in which the instruments were validated were primarily adults of all ages (Burke et al., 2021; Elhai et al., 2018; Feng et al., 2019; Gallegos et al., 2021; González-Rivera & Pagán-Torres, 2018; González-Rivera, Quintero-Jiménez, et al., 2017; González-Rivera, Veray-Alicea, et al., 2017; Lin et al., 2015; Lundman et al., 2015; Oñate et al., 2015; Pena-Gayo et al., 2018; Proyer & Laub, 2017; Roof et al., 2017; Tomás & Rosa, 2021; Wang et al., 2022; Watts et al., 2022; Wu et al., 2016), healthcare professionals (Becerra-Partida et al., 2019; Pastrana et al., 2021) such as nurses (Adib-Hajbaghery & Zehtabchi, 2016; Deluga et al., 2020; Hu et al., 2019; Kang et al., 2022; Pais et al., 2022), university students (Berger et al., 2016; Głaz, 2021; González-Rivera & Pagán-Torres, 2018; Guilherme et al., 2020; Makkar & Singh, 2021; Nawafleh et al., 2018; Riveros et al., 2018; Simkin et al., 2017) , nursing students (Fopka-Kowalczyk et al., 2023; Gonçalves et al., 2016; Guilherme et al., 2020; İpek Çoban et al., 2017), and people diagnosed with cancer (Erci & Aktürk, 2018; Lo et al., 2016; Martins et al., 2021; Pinto et al., 2016; Schiappacasse Cocio & González Soto, 2016; Simão et al., 2016; Xie et al., 2019; Zhao et al., 2021).
-
Burke et al., 2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
González-Rivera & Pagán-Torres, 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
González-Rivera, Quintero-Jiménez, et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera, Veray-Alicea, et al., 2017Desarrollo, validación y descripción teórica de la escala de espiritualidad personal en una muestra de adultos en Puerto RicoRevista Puertorriqueña de Psicología, 2017
-
Lin et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Lundman et al., 2015Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old PeopleJournal of Nursing Measurement, 2015
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Proyer & Laub, 2017The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Wang et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Watts et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Wu et al., 2016Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in TaiwanClinical Nursing Research, 2016
-
Becerra-Partida et al., 2019Depresión en pacientes con diabetes mellitus tipo 2 del programa Diabet IMSS en Guadalajara, Jalisco, MéxicoRevista CONAMED, 2019
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Adib-Hajbaghery & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
Kang et al., 2022Nurse Spiritual Care Therapeutics Scale: Validation Among Nurses Who Care for Patients With Life-Threatening Illnesses in South KoreaJournal of hospice and palliative nursing,, 2022
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Berger et al., 2016;The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
González-Rivera & Pagán-Torres, 2018Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Makkar & Singh, 2021Development of a spirituality measurement scaleCurrent Psychology, 2021
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
Riveros et al., 2018Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicosRevista Colombiana de Enfermería, 2018
-
Simkin et al., 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
-
Fopka-Kowalczyk et al., 2023The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
Gonçalves et al., 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
İpek Çoban et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Erci & Aktürk, 2018The System of Belief Inventory: A Validation Study in Turkish Cancer PatientsJournal of religion and health, 2018
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Martins et al., 2021Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing ChemoterapyJournal of Religion and Health, 2021
-
Pinto et al., 2016Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patientsPorto Biomedical Journal, 2016
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Simão et al., 2016;Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
-
Zhao et al., 2021Mass hysteria attack rates in children and adolescents: a meta-analysisJournal of International Medical Research, 2021
Of all the studies reviewed, only 11% (n = 7) measured content validity with a panel of experts (Adib-Hajbaghery & Zehtabchi, 2016; Gallegos et al., 2021; Guilherme et al., 2020; Hu et al., 2019; Wu et al., 2013; Xie et al., 2019), usually comprising nurses, theologians, psychologists, and priests. The number of experts ranged from five to 20.
-
Adib-Hajbaghery & Zehtabchi, 2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
Wu et al., 2013Persistent Organic Pollutants and Type 2 Diabetes: A Prospective Analysis in the Nurses’ Health Study and Meta-analysisEnvironmental Health Perspectives, 2013
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
Ninety-seven per cent of the studies reviewed (n = 61) measured construct validity using exploratory factor analysis, confirmatory factor analysis, or model fit indices, as shown in Table 3. Convergent construct validity was only measured in one instrument (Schiappacasse Cocio & González Soto, 2016).
-
Schiappacasse Cocio & González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
Table 3
Validity and reliability of measurement instruments
Validity and reliability of measurement instruments
| Authors/year |
Content |
Construct |
Factors |
Variance |
Criterion |
Overall |
|---|---|---|---|---|---|---|
|
Adib-Hajbaghery & Zehtabchi,
|
X | - | - | - | - | α: 0.91 |
| Agli et al., 2017 | - | X | 3 | - | - | α: 0.84 |
| Ahmad et al., 2022 | - | X | 3 | 74.2% | - | α: 0.78 |
|
Becerra Canales & Becerra
|
- | X | 3 | 54% | - | α: 0.9 |
| Benito et al., 2014 | - | X | 3 | - | X | α: 0.72 |
| Berger et al., 2016 | - | X | 6 | 58.9% | - | α: 0.91 |
| Burke et al., 2014 | - | X | 2 | - | - | - |
| Burke et al., 2021 | - | X | 3 | - | - | α: 0.96 |
| Büssing et al., 2016 | - | X | 3 | - | - | - |
|
Schiappacasse Cocio &
|
- | X | - | - | - | α: 0.91 |
| Daaleman et al., 2014 | - | X | 2 | 61% | - | α: 0.87 |
| Deluga et al., 2020 | - | X | 6 | 67.9% | - | α: 0.7 |
| Deng et al., 2021 | - | X | 2 - 3 | - | - | α: 0.91 |
| Pais et al., 2022 | - | X | 3 | - | - | α: 0.9 |
| Díaz-Castillo et al., 2021 | - | X | 3 | 59.2% | - | α: 0.93 |
| Elhai et al., 2018 | - | X | 4 | 69% | - | - |
| Erci & Aktürk, 2018 | - | X | 2 | 60.8% | - | α: 0.98 |
| Feng et al., 2019 | - | X | 3 | 52.1% | - | α: 0.85 |
| Feng et al., 2021 | - | X | 4 | 55% | - | α: 0.93 |
| Fopka et al., 2023 | - | X | 5 | 48% | - | α: : 0.88 |
| Gallardo-Peralta et al., 2018 | - | X | 2 | - | - | α: 0.92 |
| Gallegos et al., 2021 | X | X | 2 | - | - | - |
| Głaz, 2021 | - | X | 1 | 47.8% | - | α: 0.89 |
| Gonçalves et al., 2016 | - | X | 2 | - | - | α: 0.85 |
|
González-Rivera, Veray-Alicea,
|
- | X | 3 | 67.% | - | α: 0.84 |
|
González-Rivera, Quintero-
|
- | X | 3 | 72.8% | - | α: 0.92 |
| González-Rivera et al., 2018 | - | X | 3 | - | - | α: 0.88 |
|
González-Rivera & Pagán-
|
- | X | 2 | - | - | α: 0.95 |
| Guilherme et al., 2020 | X | X | 6 | 61.2% | - | α: 0.89 |
| İpek Çoban et al., 2017 | - | X | 5 | 63.6% | - | α: 0.96 |
| Hu et al., 2019 | X | X | 4 | 53.1% | X | α: > 0.7 |
| Kabakci et al., 2022 | - | X | 5 | 69% | - | α: 0.92 |
| Kang et al., 2022 | - | X | 3 | 69.4% | - | α: 0.95 |
| Levine et al., 2015 | - | X | 4 | - | - | - |
| Ling et al., 2015 | - | X | 5 | 50.4% | X | α: 0.88 |
| Lo et al., 2016 | - | X | 2 | 57% | - | α: 0.94 |
| Lundman et al., 2015 | - | X | 2 | - | X | α: 0.83 |
| Makkar & Singh, 2021 | - | X | 5 | 66.4% | - | α: 0.94 |
| Martins et al., 2021 | - | X | 1 | 74.3% | - | α: 0.89 |
| Moeini et al., 2018 | - | X | 5 | 60% | - | α: 0.82 |
| Nawafleh et al., 2018 | - | X | 4 | 95.9% | - | α: 0.92 |
| Nooripour et al., 2023 | - | X | 4 | 61% | - | α: 0.71 |
| Pinto et al., 2016 | - | X | 5 | 57.3% | - | α: 0.84 |
| Oñate et al., 2015 | - | X | 1 | 61% | - | α: 0.92 |
| Pastrana et al., 2021 | - | X | 6 | 67% | - | α: 0.92 |
| Pena-Gayo et al., 2018 | X | X | 3 | 42.3% | - | α: 0.89 |
| Proyer & Laub, 2017 | - | X | 5 | 65.6% | - | - |
| Rabitti et al., 2020 | - | X | 3 | 55% | - | α: 0.79 |
| Riveros et al., 2018 | - | X | 2 | 59.7% | - | α: 0.92 |
| Roof et al., 2017 | - | X | 4 | 85.2% | - | α: 0.94 |
| Saffari et al., 2017 | - | X | 3 | 59% | X | α: 0.9 |
| Simão et al., 2016 | - | X | 3 | - | - | α: 0.73 |
| Simkin, 2017 | - | X | 2 – 3 c/ |
- | - | - |
| Soósová et al., 2021 | - | X | 1 | 75.8% | X | α: 0.98 |
| Tomás & Rosa, 2021 | - | X | 2 | 69% | - | - |
| Vespa et al., 2017 | - | X | 2 | 72% | - | - |
| Wan et al., 2022 | - | X | 3 | 63% | - | α: 0.93 |
| Watts et al., 2022 | - | X | 3 | 50% | X | α: 0.86 |
| Weathers et al., 2020 | - | X | 5 | 56.3% | - | α: 0.9 |
| White & Schim, 2013 | - | X | 4 | 47% | X | α: 0.91١ |
| Wu et al., 2016 | X | X | 2 | 66.2% | - | - |
| Xie et al., 2019 | X | X | 3 | 65.2% | - | α: 0.88 |
| Yepes et al., 2023 | - | X | 2 | 60.3% | - | α: 0.93 |
| Zhao et al., 2019 | - | X | 6 | 63% | - | α: 0.9 |
-
Adib-Hajbaghery & Zehtabchi,Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
2016Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual CareJournal of Nursing Measurement, 2016
-
Agli et al., 2017Validation of the Functional Assessment of Chronic Illness Therapy—Spiritual Well-being (FACIT-Sp12) on French Old PeopleJournal of Religion and Health, 2017
-
Ahmad et al., 2022The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnessesAnnals of Palliative Medicine, 2022
-
Becerra Canales & BecerraDiseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Huaman, 2020Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-PerúEnfermería Global, 2020
-
Benito et al., 2014Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care PatientsJournal of Pain and Symptom Management, 2014
-
Berger et al., 2016The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College StudentsThe Spanish Journal of Psychology, 2016
-
Burke et al., 2014Inventory of Complicated Spiritual Grief: Development and Validation of a New MeasureDeath Studies, 2013
-
Burke et al., 2021Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavementDeath Studies, 2021
-
Büssing et al., 2016Spiritual and Religious Attitudes in Dealing with Illness in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK QuestionnaireJournal of Religion and Health, 2016
-
Schiappacasse Cocio &Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
González Soto, 2016Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativosGaceta Mexicana de Oncología, 2016
-
Daaleman et al., 2014Development and Preliminary Testing of the Quality of Spiritual Care ScaleJournal of Pain and Symptom Management, 2014
-
Deluga et al., 2020Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement ListPLOS ONE, 2020
-
Deng et al., 2021Two Factor Structures Possible for the FACIT-Sp in Patients With Heart FailureJournal of Pain and Symptom Management, 2021
-
Pais et al., 2022Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian ContextJournal of Religion and Health, 2022
-
Díaz-Castillo et al., 2021Desarrollo y validación de la Escala Trifactorial de Espiritualidad en personas adultas mayores mexicanasNeurama, 2021
-
Elhai et al., 2018Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaireAging & Mental Health, 2018
-
Erci & Aktürk, 2018The System of Belief Inventory: A Validation Study in Turkish Cancer PatientsJournal of religion and health, 2018
-
Feng et al., 2019Spiritual Intelligence Scale--Chinese form: Construction and initial validationCurrent Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 2019
-
Feng et al., 2021The Chinese Spiritual Coping Scale: Development and Initial Psychometric EvaluationJournal of religion and health, 2021
-
Fopka et al., 2023The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric EvaluationJournal of religion and health, 2023
-
Gallardo-Peralta et al., 2018Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayoresRevista de Psicología, 2018
-
Gallegos et al., 2021Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru)nternational Journal of Latin American Religions, 2021
-
Głaz, 2021Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG)Journal of Religion and Health, 2021
-
Gonçalves et al., 2016Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity ScaleRevista Brasileira de Enfermagem, 2016
-
González-Rivera, Veray-Alicea,Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera, Quintero-Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
Jiménez et al., 2017Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueñosRevista Electrónica de Psicología Iztacala, 2017
-
González-Rivera et al., 2018Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento ReligiosoRevista Evaluar, 2018
-
González-Rivera & Pagán-Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
Torres, 2018Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults InteraccionesInteracciones, 2018
-
Guilherme et al., 2020Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing studentsReme: Revista Mineira de Enfermagem, 2020
-
İpek Çoban et al., 2017Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish PopulationJournal of Religion and Health, 2017
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
Kabakci et al., 2022Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence ScaleCentral European Journal of Nursing and Midwifery, 2022
-
Kang et al., 2022Nurse Spiritual Care Therapeutics Scale: Validation Among Nurses Who Care for Patients With Life-Threatening Illnesses in South KoreaJournal of hospice and palliative nursing,, 2022
-
Levine et al., 2015Development and Initial Validation of a Spiritual Support Subscale for the MOS Social Support SurveyJournal of Religion and Health, 2015
-
Ling et al., 2015Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in TaiwanEuropean journal of oncology nursing, 2015
-
Lo et al., 2016Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer PainJournal of Pain and Symptom Management, 2016
-
Lundman et al., 2015Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old PeopleJournal of Nursing Measurement, 2015
-
Makkar & Singh, 2021Development of a spirituality measurement scaleCurrent Psychology, 2021
-
Martins et al., 2021Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing ChemoterapyJournal of Religion and Health, 2021
-
Moeini et al., 2018Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic DiseasesJournal of Pain and Symptom Management, 2018
-
Nawafleh et al., 2018Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South JordanApplied Nursing Research, 2018
-
Nooripour et al., 2023Validation of the Spiritual Well-being Scale (SWBS) and its role in Predicting Hope among Iranian ElderlyAgeing International, 2023
-
Pinto et al., 2016Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patientsPorto Biomedical Journal, 2016
-
Oñate et al., 2015Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, 2015
-
Pastrana et al., 2021Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ)Journal of Religion and Health, 2021
-
Pena-Gayo et al., 2018Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish contextRevista Latino-Americana de Enfermagem, 2018
-
Proyer & Laub, 2017The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial ValidationCurrent Psychology, 2017
-
Rabitti et al., 2020The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions?BMC Palliative Care, 2020
-
Riveros et al., 2018Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicosRevista Colombiana de Enfermería, 2018
-
Roof et al., 2017The spiritual engagement instrumentAsian Journal of Business Ethics, 2017
-
Saffari et al., 2017Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental HealthJournal of Religion and Health, 2017
-
Simão et al., 2016Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress ScaleJournal of clinical nursing, 2016
-
Simkin, 2017Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factoresUniversitas Psychologica, 2017
-
Soósová et al., 2021Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak ElderlyJournal of Religion and Health, 2021
-
Tomás & Rosa, 2021Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese PopulationJournal of religion and health, 2021
-
Vespa et al., 2017Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical DiseasesJournal of Religion and Health, 2017
-
Wan et al., 2022The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience ScaleArchive for the Psychology of Religion, 2022
-
Watts et al., 2022The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and worldPsychopharmacology, 2022
-
Weathers et al., 2020Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illnessApplied Nursing Research, 2020
-
White & Schim, 2013Development of a Spiritual Self-Care Practice ScaleJournal of Nursing Measurement, 2013
-
Wu et al., 2016Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in TaiwanClinical Nursing Research, 2016
-
Xie et al., 2019Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patientsJournal of Clinical Nursing, 2019
-
Yepes et al., 2023Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric PatientsJournal of Religion and Health, 2023
-
Zhao et al., 2019Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patientsInternational Journal of Nursing Sciences, 2019
Among the instruments with construct validity testing, we found an average of three factors, ranging from one to six, with an average of 61% of total explained variance, ranging from 42.3% to 95.9%. Of the instruments, 84.3% (n = 54) reported overall reliability using Cronbach’s alpha, with a range of 0.71 to 0.98.
DISCUSSION AND CONCLUSION
Main results
This review identified 64 research studies assessing spirituality from different theoretical and philosophical points of view and perspectives, including those specific to a particular population. The various constructs that can arise from spirituality or deal with the spiritual dimension of a human being are usually extremely abstract and often difficult to understand due to the nature of the phenomenon (Fuentes, 2018). Some characteristics theorists have identified about spirituality should be highlighted, such as the fact that it is subjective and individual and develops differently in each person (Sarrazin Martínez, 2021).
-
Fuentes, 2018La Religiosidad y la Espiritualidad ¿Son conceptos teóricos independientes?Revista de Psicología, 2018
-
Sarrazin Martínez, 2021La relación entre religión, espiritualidad y salud: una revisión crítica desde las ciencias socialesHallazgos,, 2021
This level of abstraction of the phenomenon gives it interpretive richness, enabling it to be evaluated from multiple theoretical perspectives. Among the psychometric studies, three approaches were identified in the definitions of spirituality or an emerging concept of this phenomenon. The first is a homocentric approach, where humans connect and relate to their environment, finding purpose or meaning in their lives through these connections. The second is a theocentric approach, in which humans establish a relationship with God, a higher power, or a mystical element, finding fulfillment and their life’s purpose in it. The third is a mixed vision, which does not separate the different connections humans establish. All these approaches enable humans to transcend their lives. These findings were expected given the nature of the phenomenon, since spirituality favors a connection with the variables of the being at an intrapersonal, interpersonal, and transpersonal level (Fuentes, 2018; López-Tarrida et al., 2020), which in turn leads the person to transcend (Reed, 2018, 2021).
-
Fuentes, 2018La Religiosidad y la Espiritualidad ¿Son conceptos teóricos independientes?Revista de Psicología, 2018
-
López-Tarrida et al., 2020Cuidando con sentido: la atención de lo espiritual en la práctica clínica desde la perspectiva del profesionalRevista Española de Salud Pública, 2020
-
Reed, 2018Theoryof self-transcendenceMiddle Range Theory for Nursing, 2018
-
2021Self-Transcendence: Moving from Spiritual Disequilibrium to Well-Being Across the Cancer TrajectorySeminars in Oncology Nursing, 2021
Spiritual needs are one of the constructs enabling us to assess spirituality in people who are ill. Identifying spiritual needs can be helpful in healthcare practice. It is because it facilitates the identification of challenges in religious or intra- and intrapersonal practices that it can be useful for hospitalized people or those with health problems (Morales-Ramón & Ojeda-Vargas, 2014; Pérez-García, 2016). However, nursing practice would be limited if only spiritual needs of a religious nature were addressed (Morales-Ramón & Ojeda-Vargas, 2014; Muñoz Devesa et al., 2014).
-
Morales-Ramón & Ojeda-Vargas, 2014El cuidado espiritual como una oportunidad de cuidado y trascendencia en la atención de enfermeríaSalud en Tabasco, 2014
-
Pérez-García, 2016Enfermería y necesidades espirituales en el paciente con enfermedad en etapa terminalEnfermería: Cuidados Humanizados, 2016
-
Morales-Ramón & Ojeda-Vargas, 2014El cuidado espiritual como una oportunidad de cuidado y trascendencia en la atención de enfermeríaSalud en Tabasco, 2014
-
Muñoz Devesa et al., 2014La Enfermería y los cuidados del sufrimiento espiritualIndex de Enfermería, 2014
Among the multiple constructs of spirituality, religious practices or rituals and theocentric belief systems are part of the transpersonal dimension of spirituality in believers. Although these two constructs closely related in some ways, they are theoretically quite different (Sarrazin Martínez, 2021). Instruments assessing religiosity as part of spirituality are therefore useful for religious populations.
-
Sarrazin Martínez, 2021La relación entre religión, espiritualidad y salud: una revisión crítica desde las ciencias socialesHallazgos,, 2021
A total of 54 different instruments assessed spirituality from multiple components, theories, and philosophical perspectives. This could be because spiritual care is becoming increasingly requested at institutions due to the implementation of human caring models in clinical practice (Soto-Rubio et al., 2020). Nurses and other health professionals are therefore becoming more aware and knowledgeable about this phenomenon, as reported by (Sarrazin Martínez, 2021).
-
Soto-Rubio et al., 2020Responding to the Spiritual Needs of Palliative Care Patients: A Randomized Controlled Trial to Test the Effectiveness of the Kibo Therapeutic InterviewFrontiers in Psychology, 2020
-
Sarrazin Martínez, 2021La relación entre religión, espiritualidad y salud: una revisión crítica desde las ciencias socialesHallazgos,, 2021
However, in several of the instruments found, there is evidence of a lack of conceptual clarity in the constructs assessed, making it difficult to understand the empirical indicators. This can also be observed in the similarity of items found in instruments assessing spirituality from different constructs.
Given the nature of the phenomenon, a lack of conceptual clarity is common in studies conducted since the 1990s. A previous review on spirituality questionnaires, conducted by de Jager Meezenbroek et al. (2012), reported that the items in the questionnaires analyzed were not as clear or appropriate for practice. Therefore, although numerous scales, inventories, and instruments exist to measure spirituality, exploring, assessing, and approaching spirituality in clinical practice is complex (López-Tarrida et al., 2020), especially when the constructs in the instruments are unclear.
-
de Jager Meezenbroek et al. (2012)Measuring Spirituality as a Universal Human Experience: A Review of Spirituality QuestionnairesJournal of Religion and Health, 2012
-
López-Tarrida et al., 2020Cuidando con sentido: la atención de lo espiritual en la práctica clínica desde la perspectiva del profesionalRevista Española de Salud Pública, 2020
Waltz et al. (2017) suggest that the first step a researcher should take when designing instruments, is conceptual operationalization, in which attributes, characteristics and dimensions are defined to distinguish the concept being assessed from others that could be considered synonyms. Conceptual inaccuracy has been one of the most common flaws in instruments assessing attributes of spirituality. This could be due to the lack of fit between the dimensions of the instruments and the conceptual definition of the phenomenon that is to be measured. It was clear from most psychometric studies that the conceptual definition was not consistent with the instrument or its dimensions. Although a conceptual definition of spirituality was given in the introduction section of many of the studies included in this review, the dimensions of the validated instrument were not known until the material and methods section. The defining characteristics enable concepts to be differentiated, thereby establishing a conceptual delimitation. These elements are known as dimensions or factors, and items are grouped according to these defining characteristics, dimensions, or factors, thereby measuring the concept intended to be evaluated (Waltz et al., 2017). The lack of a clear link between the conceptual definition and the dimensions of the instrument can therefore limit accuracy in measuring the phenomenon.
-
Waltz et al. (2017)Measurement in Nursing and Health Research, 2017
-
Waltz et al., 2017Measurement in Nursing and Health Research, 2017
In this review, three types of validity (content, construct, and criterion) were measured for the Spiritual Caregiving Scale (Hu et al., 2019), and only seven studies measured content validity. Content validity is a logical judgment attempting to determine whether items reflect the content domain being measured by assessing clarity, coherence, relevance, and (Urrutia Egaña et al., 2014).
-
Hu et al., 2019Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practiceBMC Medical Research Methodology, 2019
-
Urrutia Egaña et al., 2014Métodos óptimos para determinar validez de contenidoEducación Médica Superior, 2014
Construct validity was the most frequently reported aspect in the measurement instruments reviewed. A total of 73% of the studies used Bartlett’s test of sphericity and the Kaiser-Meyer-Olkin (KMO) measure to verify sampling adequacy for factor analysis. The KMO test shows the degree to which each variable can be predicted by the other variables. This statistic must be calculated before running the correlation matrices for factor analysis, and the criterion that KMO must be equal to or greater than 0.8 must be met (Pizarro Romero & Martínez Mora, 2020).
-
Pizarro Romero & Martínez Mora, 2020Análisis factorial exploratorio mediante el uso de las medidas de adecuación muestral kmo y esfericidad de bartlett para determinar factores principalesJournal of Science and Research, 2020
Bartlett’s test of sphericity indicates whether a correlation matrix is suitable for factor analysis, for which it must be < 0.5 (López-Aguado & Gutiérrez-Provecho, 2019). Factor analysis can then be performed. The grouping of items into factors in the pilot test confirms the concept or construct being measured by empirically dividing these groupings into dimensions (Lloret-Segura et al., 2014). To ensure accurate assessment, it is essential to clearly define the unique qualities and characteristics that differentiate the concept from others.
-
López-Aguado & Gutiérrez-Provecho, 2019Cómo realizar e interpretar un análisis factorial exploratorio utilizando SPSSREIRE Revista d’Innovaciói Recerca en Educació, 2019
-
Lloret-Segura et al., 2014El Análisis Factorial Exploratorio de los Ítems: una guía práctica, revisada y actualizadaAnales de Psicología, 2014
Certain aspects must be considered for an adequate interpretation of our results. Although our systematic search to identify the articles included in this review was not restricted by geographic region or language of publication, we cannot guarantee that we have managed to retrieve all the manuscripts on the psychometric properties of instruments evaluated spirituality, which is a limitation of this type of studies.
Despite this limitation, advantages of the present review include the fact that we searched for studies in six different electronic databases, enabling us to summarize the available evidence on the topic of interest from a larger number of studies than previous reviews. Moreover, unlike other reviews, we included information on instruments to assess spirituality among different population groups. Furthermore, researchers read and evaluated the articles to ensure an appropriate and scientifically rigorous selection, and the evaluation was conducted in phases.
In conclusion, since spirituality can be measured from multiple perspectives, concepts, and theoretical points of reference, numerous constructs have been created. Although the level of conceptual abstraction of this phenomenon provides a richness of interpretation, in practice this can cause confusion.
The need for greater clarity in certain constructs in spirituality scales is evinced by the similarity of items across instruments. There is often a lack of clarity between the conceptual operationalization and wording of the categories and empirical indicators.
Most of the studies included in this review only measured the construct validity of instruments to assess spirituality, ignoring content and criterion validity. The absence of holistic validation could restrict the precision and applicability of the measurements made, thus limiting their usefulness in various research contexts or practical applications.
The reliability of the measurement instruments analyzed in this review ranged from 0.7 to 0.98. This wide range of reliability indicates sharp differences in the consistency and stability of the measurements obtained through these instruments. Despite the variability, it is important to note that most instruments demonstrate levels of reliability that can be considered acceptable in terms of internal consistency and reproducibility of results. However, it should be noted that reliability alone does not guarantee the validity of measurements, as precision and consistency may not necessarily determine the accuracy of what is being measured.
References
- Adib-Hajbaghery, M., & Zehtabchi, S. (2016). Developing and Validating an Instrument to Assess the Nurses’ Professional Competence in Spiritual Care. Journal of Nursing Measurement, 24(1), 15-27. https://doi.org/10.1891/1061-3749.24.1.15 Links
- Agli, O., Bailly, N., & Ferrand, C. (2017). Validation of the Functional Assessment of Chronic Illness Therapy—Spiritual Well-being (FACIT-Sp12) on French Old People. Journal of Religion and Health, 56(2), 464-476. https://doi.org/10.1007/s10943-016-0220-0 Links
- Ahmad, N., Sinaii, N., Panahi, S., Bagereka, P., Serna-Tamayo, C., Shnayder, S., Ameli, R., & Berger, A. (2022). The FACIT-Sp spiritual wellbeing scale: a factor analysis in patients with severe and/or life-limiting medical illnesses. Annals of Palliative Medicine, 11(12), 3663-3673. https://doi.org/10.21037/apm-22-692 Links
- Becerra Canales, B., & Becerra Huaman, D. (2020). Diseño y validación de la escala de Inteligencia Espiritual en la práctica sanitaria, Ica-Perú. Enfermería Global, 19(4), 349-378. https://doi.org/10.6018/eglobal.417371 Links
- Becerra-Partida, E. N., Millán, R. M., & Arias, D. R. R. (2019). Depresión en pacientes con diabetes mellitus tipo 2 del programa DiabetIMSS en Guadalajara, Jalisco, México. Revista CONAMED, 24(4), 174–178. http://www.conamed.gob.mx/gobmx/revista/pdf/vol_23_2018/COMPLETO_4.pdf Links
- Benito, E., Oliver, A., Galiana, L., Barreto, P., Pascual, A., Gomis, C., & Barbero, J. (2014). Development and Validation of a New Tool for the Assessment and Spiritual Care of Palliative Care Patients. Journal of Pain and Symptom Management, 47(6), 1008-1018.e1. https://doi.org/10.1016/j.jpainsymman.2013.06.018 Links
- Berger, D., Fink, A., Perez Gomez, M. M., Lewis, A., & Unterrainer, H. (2016). The Validation of a Spanish Version of the Multidimensional Inventory of Religious/Spiritual Well-Being in Mexican College Students. The Spanish Journal of Psychology, 19, https://doi.org/10.1017/sjp.2016.9 Links
- Burke, L. A., Crunk, A. E., Neimeyer, R. A., & Bai, H. (2021). Inventory of Complicated Spiritual Grief 2.0 (ICSG 2.0): Validation of a revised measure of spiritual distress in bereavement. Death Studies, 45(4), 249-265. https://doi.org/10.1080/07481187.2019.1627031 Links
- Burke, L. A., Neimeyer, R. A., Holland, J. M., Dennard, S., Oliver, L., & Shear, M. K. (2013). Inventory of Complicated Spiritual Grief: Development and Validation of a New Measure. Death Studies, 38(4), 239–250. https://doi.org/10.1080/07481187.2013.810098 Links
- Büssing, A., Franczak, K., & Surzykiewicz, J. (2016). Spiritual and Religious Attitudes in Dealing with Illness in Polish Patients with Chronic Diseases: Validation of the Polish Version of the SpREUK Questionnaire. Journal of Religion and Health, 55(1), 67–84. https://doi.org/10.1007/s10943-014-9967-3 Links
- Caccia, P., & Elgier, M. (2020). Resiliencia y satisfacción con la vida en adolescentes según nivel de espiritualidad. PSOCIAL; 6(2), 62–70. https://publicaciones.sociales.uba.ar/index.php/psicologiasocial/article/view/5975 Links
- Daaleman, T. P., Reed, D., Cohen, L. W., & Zimmerman, S. (2014). Development and Preliminary Testing of the Quality of Spiritual Care Scale. Journal of Pain and Symptom Management, 47(4), 793-800. https://doi.org/10.1016/j.jpainsymman.2013.06.004 Links
- de Diego-Cordero, R., Suárez-Reina, P., Badanta, B., Lucchetti, G., & Vega-Escaño, J. (2022). The efficacy of religious and spiritual interventions in nursing care to promote mental, physical and spiritual health: A systematic review and meta-analysis. Applied Nursing Research, 67, 151618. https://doi.org/10.1016/j.apnr.2022.151618 Links
- de Jager Meezenbroek, E., Garssen, B., van den Berg, M., van Dierendonck, D., Visser, A., & Schaufeli, W. B. (2012). Measuring Spirituality as a Universal Human Experience: A Review of Spirituality Questionnaires. Journal of Religion and Health, 51(2), 336-354. https://doi.org/10.1007/s10943-010-9376-1 Links
- Deluga, A., Dobrowolska, B., Jurek, K., Ślusarska, B., Nowicki, G., & Palese, A. (2020). Nurses’ spiritual attitudes and involvement—Validation of the Polish version of the Spiritual Attitude and Involvement List. PLOS ONE, 15(9), e0239068. https://doi.org/10.1371/journal.pone.0239068 Links
- Deng, L. R., Masters, K. S., Schmiege, S. J., Hess, E., & Bekelman, D. B. (2021). Two Factor Structures Possible for the FACIT-Sp in Patients With Heart Failure. Journal of Pain and Symptom Management, 62(5), 1034-1040. https://doi.org/10.1016/j.jpainsymman.2021.05.009 Links
- Díaz-Castillo, R., Montero-López Lena, M., González-Escobar, S., & González-Arratia López Fuente, N. I. (2021). Desarrollo y validación de la Escala Trifactorial de Espiritualidad en personas adultas mayores mexicanas. Neurama, 8(1), 39–52. https://www.neurama.es/articulos/15/articulo4.pdf Links
- Elhai, N., Carmel, S., O’Rourke, N., & Bachner, Y. G. (2018). Translation and validation of the Hebrew version of the SHALOM Spiritual questionnaire. Aging & Mental Health, 22(1), 46–52. https://doi.org/10.1080/13607863.2016.1222350 Links
- Epstein, J., Santo, R. M., & Guillemin, F. (2015). A review of guidelines for cross-cultural adaptation of questionnaires could not bring out a consensus. Journal of Clinical Epidemiology, 68(4), 435-441. https://doi.org/10.1016/j.jclinepi.2014.11.021 Links
- Erci, B., & Aktürk, Ü. (2018). The System of Belief Inventory: A Validation Study in Turkish Cancer Patients. Journal of religion and health, 57(4), 1237-1245. https://doi.org/10.1007/s10943-017-0406-0 Links
- Feng, J., Li, Y., Sun, Y., Wang, L., Qi, W., Wang, K. T., & Xue, Y. (2021). The Chinese Spiritual Coping Scale: Development and Initial Psychometric Evaluation. Journal of religion and health, 60(1), 458–474. https://doi.org/10.1007/s10943-019-00970-z Links
- Feng, M., Xiong, X.-y., & Li, J.-j. (2019). Spiritual Intelligence Scale--Chinese form: Construction and initial validation. Current Psychology: A Journal for Diverse Perspectives on Diverse Psychological Issues, 38(5), 1318–1327. https://doi.org/10.1007/s12144-017-9678-5 Links
- Fopka-Kowalczyk, M., Best, M., & Krajnik, M. (2023). The Spiritual Supporter Scale as a New Tool for Assessing Spiritual Care Competencies in Professionals: Design, Validation, and Psychometric Evaluation. Journal of religion and health, 62(3), 2081–2111. https://doi.org/10.1007/s10943-022-01608-3 Links
- Fuentes, L. del C. (2018). La Religiosidad y la Espiritualidad ¿Son conceptos teóricos independientes? Revista de Psicología, 14(28), 109-119. https://erevistas.uca.edu.ar/index.php/RPSI/article/view/1742 Links
- Gallardo-Peralta, L. P., Cuadra-Peralta, A., & Veloso-Besio, C. (2018). Validación de un Índice Breve de Religiosidad y Espiritualidad en personas mayores. Revista de Psicología, 27(1), 1. https://doi.org/10.5354/0719-0581.2018.50736 Links
- Gallegos, W. L. A., Loayza, A. E., Rivera, R., & Cohello, A. L. N. (2021). Modified and Validated Version of the System of Beliefs Inventory (SBI-15R) in a Sample of Inhabitants from Arequipa City (Peru). International Journal of Latin American Religions, 5(2), 501-518. https://doi.org/10.1007/s41603-021-00139-1 Links
- González-Rivera, J. A., & Pagán-Torres, O. M. (2018). Desarrollo y Validación de un instrumento para medir Estrategias de Afrontamiento Religioso. Revista Evaluar, 18(1), 70-86. https://doi.org/10.35670/1667-4545.v18.n1.19771 Links
- González-Rivera, J. A., Quintero-Jiménez, N., Veray-Alicea, J., & Rosario-Rodríguez, A. (2017). Adaptación y validación de la escala de espiritualidad de delaney en una muestra de adultos puertorriqueños. Revista Electrónica de Psicología Iztacala, 20(1). https://www.revistas.unam.mx/index.php/repi/article/view/58935 Links
- González-Rivera, J. A., Veray-Alicea, J., & Rosario-Rodríguez, A. (2017). Desarrollo, validación y descripción teórica de la escala de espiritualidad personal en una muestra de adultos en Puerto Rico. Revista Puertorriqueña de Psicología, 28(2), 388-404. Links
- González-Rivera, J., Rosario-Rodríguez, A., & Pagán-Torres, O. (2018). Confirmatory Factorial Analysis of the Personal Spirituality Scale in Puerto Ricans Adults Interacciones. Interacciones, 4(3), 153-162. https://doi.org/10.24016/2018.v4n3.101 Links
- Gonçalves, A. M. D. S., Santos, M. A. D., Chaves, E. D. C. L., & Pillon, S. C. (2016). Adaptação transcultural e validação da versão brasileira da Treatment Spirituality / Religiosity Scale. Revista Brasileira de Enfermagem, 69(2), 235-241. https://doi.org/10.1590/0034-7167.2016690205i Links
- Guilherme, C., Fulquini, F., Ribeiro, V., Gadioli, B., Eduardo, A., Caldeira, S., & Carvalho, E. (2020). Validity evidenceofthe spiritual care competence scale for brazilian undergraduate nursing students. Reme: Revista Mineira de Enfermagem, 24(1), e-1343. https://doi.org/10.5935/1415.2762.20200080 Links
- Głaz, S. (2021). Psychological Analysis of Religiosity and Spirituality: Construction of the Scale of Abandonment by God (SAG). Journal of Religion and Health, 60(5), 3545–3561. https://doi.org/10.1007/s10943-021-01197-7 Links
- Herdman, M., Fox-Rushby, J., & Badia, X. (1998). A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Quality of life research : an international journal of quality of life aspects of treatment, care and rehabilitation, 7(4), 323-335. https://doi.org/10.1023/a:1024985930536 Links
- Hu, Y., Tiew, L. H., & Li, F. (2019). Psychometric properties of the Chinese version of the spiritual care-giving scale (C-SCGS) in nursing practice. BMC Medical Research Methodology, 19(1), 21. https://doi.org/10.1186/s12874-019-0662-7 Links
- İpek Çoban, G., Şirin, M., & Yurttaş, A. (2017). Reliability and Validity of the Spiritual Care-Giving Scale in a Turkish Population. Journal of Religion and Health, 56(1), 63-73. https://doi.org/10.1007/s10943-015-0086-6 Links
- Kabakci, E. N., & Çelik, N. (2022). Adaptation into Turkish and evaluation of the psychometric properties of the Spiritual Care Competence Scale. Central European Journal of Nursing and Midwifery, 13(2), 648-656. https://doi.org/10.15452/cejnm.2022.13.0001 Links
- Kang, K. A., Taylor, E. J., & Chun, J. (2022). Nurse Spiritual Care Therapeutics Scale: Validation Among Nurses Who Care for Patients With Life-Threatening Illnesses in South Korea. Journal of hospice and palliative nursing, https://doi.org/10.1097/NJH.0000000000000895. Advance online publication. https://doi.org/10.1097/NJH.0000000000000895 Links
- Levine, E. G., Vong, S., & Yoo, G. J. (2015). Development and Initial Validation of a Spiritual Support Subscale for the MOS Social Support Survey. Journal of Religion and Health, 54(6), 2355-2366. https://doi.org/10.1007/s10943-015-0005-x Links
- Lin, Y. L., Rau, K. M., Liu, Y. H., Lin, Y. H., Ying, J., & Kao, C. C. (2015). Development and validation of the Chinese Version of Spiritual Interests Related Illness Tool for patients with cancer in Taiwan. European journal of oncology nursing, 19(5), 589-594. https://doi.org/10.1016/j.ejon.2015.03.005 Links
- Lloret-Segura, Susana, Ferreres-Traver, Adoración, Hernández-Baeza, Ana, & Tomás-Marco, Inés. (2014). El Análisis Factorial Exploratorio de los Ítems: una guía práctica, revisada y actualizada. Anales de Psicología, 30(3), 1151-1169. https://dx.doi.org/10.6018/analesps.30.3.199361 Links
- Lo, G., Chen, J., Wasser, T., Portenoy, R., & Dhingra, L. (2016). Initial Validation of the Daily Spiritual Experiences Scale in Chinese Immigrants With Cancer Pain. Journal of Pain and Symptom Management, 51(2), 284-291. https://doi.org/10.1016/j.jpainsymman.2015.10.002 Links
- López-Aguado, M., & Gutiérrez-Provecho, L. (2019). Cómo realizar e interpretar un análisis factorial exploratorio utilizando SPSS. REIRE Revista d’Innovaciói Recerca en Educació, 12(2), https://doi.org/10.1344/reire2019.12.227057 Links
- López-Tarrida, Á. C, Ruiz-Romero, V., & González-Martín, T. (2020). Cuidando con sentido: la atención de lo espiritual en la práctica clínica desde la perspectiva del profesional. Revista Española de Salud Pública, 94, 202001002. Recuperado en 08 de enero de 2025, de http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1135-57272020000100083&lng=es&tlng=es. Links
- Lundman, B., Årestedt, K., Norberg, A., Norberg, C., Fischer, R. S., & Lövheim, H. (2015). Psychometric Properties of the Swedish Version of the Self-Transcendence Scale Among Very Old People. Journal of Nursing Measurement, 23(1), 96-111. https://doi.org/10.1891/1061-3749.23.1.96 Links
- Makkar, S., & Singh, A. K. (2021). Development of a spirituality measurement scale. Current Psychology, 40(3), 1490-1497. https://doi.org/10.1007/s12144-018-0081-7 Links
- Martins, H., Caldeira, S., Domingues, T., Vieira, M., & Koenig, H. (2021). Validation of the Duke University Religion Index (DUREL) in Portuguese Cancer Patients Undergoing Chemoterapy. Journal of Religion and Health, 60(5), 3562-3575. https://doi.org/10.1007/s10943-020-01143-z Links
- Moeini, B., Zamanian, H., Taheri-Kharameh, Z., Ramezani, T., Saati-Asr, M., Hajrahimian, M., & Amini-Tehrani, M. (2018). Translation and Psychometric Testing of the Persian Version of the Spiritual Needs Questionnaire Among Elders With Chronic Diseases. Journal of Pain and Symptom Management, 55(1), 94-100. https://doi.org/10.1016/j.jpainsymman.2017.08.024 Links
- Mokkink, L. B., de Vet, H. C. W., Prinsen, C. A. C., Patrick, D. L., Alonso, J., Bouter, L. M., & Terwee, C. B. (2018). COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Quality of life research, 27(5), 1171-1179. https://doi.org/10.1007/s11136-017-1765-4 Links
- Morales Contreras, B. N., & Palencia Sierra, J. J. (2021). Dimensión espiritual en el cuidado enfermero. Enfermería Investiga, 6(2), 51-59. https://doi.org/10.31243/ei.uta.v6i2.1073.2021 Links
- Morales-Ramón, F., & Ojeda-Vargas, M. G. (2014). El cuidado espiritual como una oportunidad de cuidado y trascendencia en la atención de enfermería. Salud en Tabasco, 20(3), 94-97. Links
- Muñiz, J., & Fonseca-Pedrero, E. (2019). Diez pasos para la construcción de un test. Psicothema, 1(31), 7-16. https://doi.org/10.7334/psicothema2018.291 Links
- Muñoz Devesa, A., Morales Moreno, I., Bermejo Higuera, J. C., & Galán González Serna, J. M. (2014). La Enfermería y los cuidados del sufrimiento espiritual. Index de Enfermería, 23(3), 153-156. https://doi.org/10.4321/s1132-12962014000200008 Links
- Nawafleh, H. A., Al Hadid, L. A., Al Momani, M. M., & Al Barmawi, M. (2018). Measuring the psychometric properties of the Arabic version of the spirituality questionnaire among university students in South Jordan. Applied Nursing Research, 39, 115-120. https://doi.org/10.1016/j.apnr.2017.11.008 Links
- Nooripour, R., Ghanbari, N., Hosseinian, S., Ronzani, T. M., Hussain, A. J., Ilanloo, H., Majd, M. A., Soleimani, E., Saffarieh, M., & Yaghoob, V. (2023). Validation of the Spiritual Well-being Scale (SWBS) and its role in Predicting Hope among Iranian Elderly. Ageing International, 48(2), 593-611. https://doi-org.ugto.idm.oclc.org/10.1007/s12126-022-09492-8 Links
- Oñate, M. E., Resett, S., Sanabria, M. E., & MenghI, M. S. (2015). Propiedades psicométricas de la dimensión espiritualidad de la evaluación multidimensional de la religiosidad y la espiritualidad, VII Congreso Internacional de Investigación y Práctica Profesional en Psicología XXII Jornadas de Investigación XI Encuentro de Investigadores en Psicología del MERCOSUR. Facultad de Psicología, Universidad de Buenos Aires. https://www.aacademica.org/000-015/941.pdf Links
- Pagán-Torres, O. M. (2022). Abriendo nuevas puertas: Relevancia clínica de integrar la religión y la espiritualidad en la disciplina de la psicología. Revista Puertorriqueña de Psicología, 33(2), 258–271. https://www.repsasppr.net/index.php/reps/article/view/761 Links
- Pais, N., Suresh, S., & DCunha, S. (2022). Spirituality and Spiritual Care in Nursing: Validity of the Spirituality and Spiritual Care Rating Scale in an Indian Context. Journal of Religion and Health, 62, 2131-2143. https://doi.org/10.1007/s10943-022-01634-1 Links
- Pastrana, T., Frick, E., Krikorian, A., Ascencio, L., Galeazzi, F., & Büssing, A. (2021). Translation and Validation of the Spanish Version of the Spiritual Care Competence Questionnaire (SCCQ). Journal of Religion and Health, 60(5), 3621-3639. https://doi.org/10.1007/s10943-021-01402-7 Links
- Pena-Gayo, A., González-Chordá, V. M., Cervera-Gasch, Á., & Mena-Tudela, D. (2018). Cross-cultural adaptation and validation of Pamela Reed’s Self-Transcendence Scale for the Spanish context. Revista Latino-Americana de Enfermagem, 26, https://doi.org/10.1590/1518-8345.2750.3058 Links
- Pérez-García, E. (2016). Enfermería y necesidades espirituales en el paciente con enfermedad en etapa terminal. Enfermería: Cuidados Humanizados, 5(2), 41-45. Links
- Pinto, S. M. O., Berenguer, S. M. A. C., Martins, J. C. A., & Kolcaba, K. (2016). Cultural adaptation and validation of the Portuguese End of Life Spiritual Comfort Questionnaire in Palliative Care patients. Porto Biomedical Journal, 1(4), 147-152. https://doi.org/10.1016/j.pbj.2016.08.003 Links
- Pizarro Romero, K. P., & Martínez Mora, O. M. (2020). Análisis factorial exploratorio mediante el uso de las medidas de adecuación muestral kmo y esfericidad de bartlett para determinar factores principales. Journal of Science and Research, 5, 903-924. https://doi.org/10.5281/zenodo.4453224 Links
- Proyer, R. T., & Laub, N. (2017). The German-Language Version of the Expressions of Spirituality Inventory-Revised: Adaptation and Initial Validation. Current Psychology, 36(1), 1-13. https://doi.org/10.1007/s12144-015-9379-x Links
- Rabitti, E., Cavuto, S., Iani, L., Ottonelli, S., De Vincenzo, F., & Costantini, M. (2020). The assessment of spiritual well-being in cancer patients with advanced disease: which are its meaningful dimensions? BMC Palliative Care, 19(1), 26. https://doi.org/10.1186/s12904-020-0534-2 Links
- Reed, P. G. (2018). Theoryof self-transcendence. In: M. J. Smith, & P. Liehr (Eds.), Middle Range Theory for Nursing, 4th Edition, Vol. 3, pp. 119-145. Springer Publishing Company. https://doi.org/10.1891/9780826159922.0007 Links
- Reed, P. G. (2021). Self-Transcendence: Moving from Spiritual Disequilibrium to Well-Being Across the Cancer Trajectory. Seminars in Oncology Nursing, 37(5), 151212. https://doi.org/10.1016/j.soncn.2021.151212 Links
- Reed, P. G., & Haugan, G. (2021). Self-Transcendence: A Salutogenic Process for Well-Being. In: G. Haugan & M. Eriksson (Eds.), Health Promotion in Health Care – Vital Theories and Research. Springer. http://www.ncbi.nlm.nih.gov/books/NBK585654/ Links
- Riveros, F., Bernal, L., Bohórquez, D., Vinaccia, S., & Quiceno, M. (2018). Inventario de sistema de creencias (SBI-15 R) en Colombia: estructura factorial y confiabilidad en población universitaria y en pacientes crónicos. Revista Colombiana de Enfermería, 17, 13-20. https://doi.org/10.18270/rce.v17i13.2103 Links
- Roof, R. A., Bocarnea, M. C., & Winston, B. E. (2017). The spiritual engagement instrument. Asian Journal of Business Ethics, 6(2), 215-232. https://doi.org/10.1007/s13520-017-0073-y Links
- Saffari, M., Amini, H., Sheykh-oliya, Z., Pakpour, A. H., & Koenig, H. G. (2017). Validation of the Persian version of the Daily Spiritual Experiences Scale (DSES) in Pregnant Women: A Proper Tool to Assess Spirituality Related to Mental Health. Journal of Religion and Health, 56(6), 2222-2236. https://doi.org/10.1007/s10943-017-0393-1 Links
- Sánchez-Villena, A. R., de La Fuente-Figuerola, V., & Ventura-León, J. (2021). Importancia de los estudios semánticos en la adaptación transcultural y validación de instrumentos de medida en Ciencias de la Salud. Enfermería Clínica, 31(2), 126-127. https://doi.org/10.1016/j.enfcli.2020.08.002 Links
- Sarrazin Martínez, J. P. (2021). La relación entre religión, espiritualidad y salud: una revisión crítica desde las ciencias sociales. Hallazgos, https://doi.org/10.15332/2422409x.5232 Links
- Schiappacasse Cocio, G., & González Soto, P. (2016). Validación del test Meaning in Life Scale (MILS) modificado para evaluar la dimensión espiritual en población chilena y latinoamericana con cáncer en cuidados paliativos. Gaceta Mexicana de Oncología, 15(3), 121-127. https://doi.org/10.1016/j.gamo.2016.05.004 Links
- Simão, T. P., Lopes Chaves, E.deC., Campos de Carvalho, E., Nogueira, D. A., Carvalho, C. C., Ku, Y. L., & Iunes, D. H. (2016). Cultural adaptation and analysis of the psychometric properties of the Brazilian version of the Spiritual Distress Scale. Journal of clinical nursing, 25(1-2), 231-239. https://doi.org/10.1111/jocn.13060 Links
- Simkin, H. (2017). Adaptación y Validación al español de la Escala de Evaluación de Espiritualidad y Sentimientos Religiosos (ASPIRES): la trascendencia espiritual en el modelo de los cinco factores. Universitas Psychologica, 16(2). https://doi.org/10.11144/javeriana.upsy16-2.aeee Links
- Soósová, M. S., & Mauer, B. (2021). Psychometrics Properties of the Daily Spiritual Experience Scale in Slovak Elderly. Journal of Religion and Health, 60(1), 563-575. https://doi.org/10.1007/s10943-020-00994-w Links
- Soto-Rubio, A., Perez-Marin, M., Rudilla, D., Galiana, L., Oliver, A., Fombuena, M., & Barreto, P. (2020). Responding to the Spiritual Needs of Palliative Care Patients: A Randomized Controlled Trial to Test the Effectiveness of the Kibo Therapeutic Interview. Frontiers in Psychology, 11. https://doi.org/10.3389/fpsyg.2020.01979 Links
- Steger, M. F., Frazier, P., Oishi, S., & Kaler, M. (2006). The meaning in life questionnaire: Assessing the presence of and search for meaning in life. Journal of Counseling Psychology, 53(1), 80-93. https://doi.org/10.1037/0022-0167.53.1.80 Links
- Tomás, C., & Rosa, P. J. (2021). Validation of a Scale of Religious and Spiritual Coping (RCOPE) for the Portuguese Population. Journal of religion and health, 60(5), 3510-3529. https://doi.org/10.1007/s10943-021-01248-z Links
- Tricco, A. C., Lillie, E., Zarin, W., O’Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., &Straus, S. E. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Annals of Internal Medicine, 169(7), 467-473. https://doi.org/10.7326/m18-0850 Links
- Urrutia Egaña, M., Barrios Araya, S., Gutiérrez Núñez, M., & Mayorga Camus, M. (2014). Métodos óptimos para determinar validez de contenido. Educación Médica Superior, 28(3), 547-558. https://ems.sld.cu/index.php/ems/article/view/301 Links
- Vespa, A., Giulietti, M. V., Spatuzzi, R., Fabbietti, P., Meloni, C., Gattafoni, P., & Ottaviani, M. (2017). Validation of Brief Multidimensional Spirituality/Religiousness Inventory (BMMRS) in Italian Adult Participants and in Participants with Medical Diseases. Journal of Religion and Health, 56(3), 907-915. https://doi.org/10.1007/s10943-016-0285-9 Links
- Waltz, C., Strickland, O., & Lenz, E. (2017). Measurement in Nursing and Health Research (5th ed.). Springer Publishing Company, New York. https://www.springerpub.com/measurement-in-nursing-and-health-research-9780826170613.html Links
- Wang, Q., Zhou, X., & Ng, S. (2022). The experiences of spiritual enlightenment: A mixed-method study of the development of a Spiritual Enlightenment Experience Scale. Archive for the Psychology of Religion, 44(3), 175-201. https://doi.org/10.1177/00846724221121686 Links
- Watts, R., Kettner, H., Geerts, D., Gandy, S., Kartner, L., Mertens, L., Timmermann, C., Nour, M. M., Kaelen, M., Nutt, D., Carhart-Harris, R., & Roseman, L. (2022). The Watts Connectedness Scale: a new scale for measuring a sense of connectedness to self, others, and world. Psychopharmacology, 239(11), 3461-3483. https://doi.org/10.1007/s00213-022-06187-5 Links
- Weathers, E., Coffey, A., McSherry, W., & McCarthy, G. (2020). Development and validation of the Spirituality Instrument-27© (SpI-27©) in individuals with chronic illness. Applied Nursing Research, 56, 151331. https://doi.org/10.1016/j.apnr.2020.151331 Links
- White, M. L., & Schim, S. M. (2013). Development of a Spiritual Self-Care Practice Scale. Journal of Nursing Measurement, 21(3), 450-462. https://doi.org/10.1891/1061-3749.21.3.450 Links
- Wu, H., Bertrand, K. A., Choi, A. L., Hu, F. B., Laden, F., Grandjean, P., & Sun, Q. (2013). Persistent Organic Pollutants and Type 2 Diabetes: A Prospective Analysis in the Nurses’ Health Study and Meta-analysis. Environmental Health Perspectives, 121(2), 153-161. https://doi.org/10.1289/ehp.1205248 Links
- Wu, L., Koo, M., Liao, Y.-C., Chen, Y.-M., & Yeh, D.-C. (2016). Development and Validation of the Spiritual Care Needs Inventory for Acute Care Hospital Patients in Taiwan. Clinical Nursing Research, 25(6), 590-606. https://doi.org/10.1177/1054773815579609 Links
- Xie, H., Taylor, E. J., Li, M., Wang, Y., & Liang, T. (2019). Nurse Spiritual Therapeutics Scale: Psychometric evaluation among cancer patients. Journal of Clinical Nursing, 28(5-6), 939-946. https://doi.org/10.1111/jocn.14711 Links
- Yepes Martinez, M. V., Rossi, R., Ciani, M., & Ferrari, C. (2023). Validation of the Italian Version of the Daily Spiritual Experience Scale Among Psychiatric Patients. Journal of Religion and Health, 62(3), 2181-2195. https://doi.org/10.1007/s10943-022-01672-9 Links
- Zhao, G., Cheng, Q., Dong, X., & Xie, L. (2021). Mass hysteria attack rates in children and adolescents: a meta-analysis. Journal of International Medical Research, 49(12). https://doi.org/10.1177/03000605211039812 Links
- Zhao, Y., Wang, Y., Yao, X., Jiang, L., Hou, M., & Zhao, Q. (2019). Reliability and validity of the Chinese version of spiritual needs questionnaire with 27 items (SpNQ-Ch-27) in cancer patients. International Journal of Nursing Sciences, 6(2), 141-147. https://doi.org/10.1016/j.ijnss.2019.03.010 Links