Características familiares y trastornos de la conducta alimentaria en una muestra de mujeres adolescentes internadas en un hospital psiquiátrico
Family characteristics and eating disorders in a sample of female adolescent inpatients in a psychiatric hospital
Mauricio Leija Esparza,1 Juan Manuel Sauceda García,2 Rosa Elena Ulloa Flores3
1 Instituto Jalisciense de Salud Mental.
]]> 2 Departamento de Psicología Médica, Psiquiatría y Salud Mental de la Facultad de Medicina, UNAM.3 Departamento de Psicofarmacología del Desarrollo. Hospital Psiquiátrico Infantil Dr. Juan N. Navarro.
Correspondencia:
Dr. Mauricio Leija Esparza.
Instituto Jalisciense de Salud Mental.
Av. Zoquipan 1000–A, col. Zoquipan, 45170, Zapopan,
Jalisco, México. Tel. (0133) 3633 9383 ext. 254.
E–mail: mauricio.leija@gmail.com
]]> Recibido primera versión: 19 de marzo de 2010.
ABSTRACT
Background
From the first descriptions of the eating disorders, researchers have found that the families of patients with anorexia nervosa or bulimia nervosa present high levels of family dysfunction. These families tend to differ from the control families, mainly because they present a greater frequency of conflicts and disorganization, less adaptability and cohesion, poor care of the parents towards their children, presence of overprotection, less orientation towards recreational activities and less emotional support.
Several authors have suggested that a family adverse environment might represent an important etiologic factor for the development of an eating disorder. Nevertheless, the symptoms more related to degree of dysfunction or to quality of family environment in such patients have not been identified.
Objective
To describe the frequency of the eating disorders as well as eating disorder not otherwise specified in a sample of inpatient female adolescents; and to establish the relationship that functioning and quality of the family environment hold with the severity and/or characteristics of the eating psychopathology.
]]> Subjects and methodsThe study included a group of 36 female adolescents hospitalized due to any type of psychopathology in the Children's Psychiatric Hospital Dr. Juan N. Navarro. The study sample consisted of all the patients who wanted to be included and who fulfilled the inclusion criteria. A written informed consent was obtained from parents as approved by the Department of Research of the Children's Psychiatric Hospital Dr. Juan N. Navarro.
Diagnostic categories in the sample, including eating disorders, were based on the Mini-International Neuropsychiatrie Interview -Kid (MINI-Kid). Those that presented an eating disorder not otherwise specified were diagnosed with a clinical interview based on DSM-IV criteria.
In addition, the patients answered a series of self reports: the Eating Disorder Inventory, the General Functioning Subscale of the McMaster Family Assessment Device and the Child Figure Rating Scale.
The body dissatisfaction was considered if the patient had negative scores (she wanted to be thinner) in the Child Figure Rating Scale.
The score on the Global Family Environment Scale was obtained through a non-structured interview concerning the quality of the family environment (assessed in retrospect) and this information was complemented with that contained in each patient's medical chart.
Results
From the 36 patients included, 39% presented an eating disorder (17% a specific disorder and 22% an eating disorder not otherwise specified), 42% presented only body dissatisfaction and 19% of the sample was free of eating psychopathology.
The average of the body mass index was within the normal range (23.2 kg/m2); nevertheless the average score of the Eating Disorder Inventory (58.22) was higher than what some authors have suggested as cut point score for anorexia nervosa. The average score of the General Functioning Subscale of the McMaster Family Assessment Device (2.16) was in the low normal limit and the Global Family Environment Scale showed an average (62.8) that would correspond to a moderately unsatisfactory family environment.
The total sample was divided in two subgroups; the first included the patients who fulfilled the criteria for eating disorder (including an eating disorder not otherwise specified) and the second subgroup included the rest of the patients. There were not significant differences in the type or number of comorbid disorders. The mean scores of the Eating Disorder Inventory were higher in the subgroup with eating disorder with a statistically significant difference (p<0.01). In a similar way, the dissatisfaction with the weight and the current figure as well as the dissatisfaction to future showed statistically significant differences (p<0.01). The score in the scales of functioning and quality of the family environment did not show statistically significant differences.
]]> We also divided the whole sample in two subgroups, one with family dysfunction (as determined by the General Functioning Subscale of the McMaster Family Assessment Device ≥2.17), and the other without family dysfunction (scored <2.17). The group with family dysfunction presented a higher frequency of major depressive disorder and social phobia with a statistically significant difference (p<0.05).In a similar fashion, we divided the sample in two subgroups, one with high to moderate quality family environment (score in the Global Family Environment Scale >70) and a second one with low quality family environment (score <70). Nevertheless, these subgroups did not show statistically significant differences concerning psychopathological disorders.
We found a positive correlation (r=0.34) among the total score of the Eating Disorder Inventory and the score of the General Functioning Subscale of the McMaster Family Assessment Device (p<0.05). The subscale of the Eating Disorder Inventory that had higher correlation was bulimic symptomatology (r=0.51) followed by ineffectiveness (r=0.43), both statistically significant (p<0.01). On the other hand, the Global Family Environment Scale did not show significant correlations with the Eating Disorder Inventory.
Conclusions
Eating disorders represent an important cause of morbidity in adolescent female inpatients; likewise, the patients were more frequently diagnosed with an eating disorders not otherwise specified than with anorexia nervosa and bulimia nervosa (in the sample recruited for the present study, we found that the eating disorders not otherwise specified represented 56% of the total of eating disorders), making the early detection necessary for the beginning of treatments directed to avoid the evolution to severe forms. We need to pay attention to atypical conditions that do not fulfill the full diagnostic criteria for anorexia or bulimia, as they may be in fact associated with important levels of dysfunction and comorbidity.
The dissatisfaction with the weight and figure was shown by the majority of the patients who were hospitalized in a psychiatric unit. Adolescence can be accompanied by great dissatisfaction with self appearance; nevertheless, to determine the relevance of this phenomenon as a risk factor for the development of an eating disorder, follow-up studies with bigger samples are needed.
Family dysfunction is a variable that relates to the severity of the eating disorders, mainly the bulimic symptoms. From this perspective these findings seem to support the psychodynamic interpretation of bulimia nervosa, where bingeing symbolizes the marked dependence to significant figures, and vomiting the desire to expel an evil introjected object. Nevertheless, given the impossibility to do inferences beyond a simple association among variables, another explanation could be that the aforementioned symptoms were damaging the family functioning, creating in this way a vicious circle.
This finding may be important to determine which group of symptoms could be expected to improve after a family intervention directed to treat an eating disorder.
The lack of correlations between the Global Family Environment Scale and the Eating Disorder Inventory could be explained by the fact that the Global Family Environment Scale evaluates functioning during the worst year of the patients' life, which could be during their first five years, thus its effect⁄impact on current psychopathology could not be established.
Key words: Family environment, family functioning, eating disorders, body dissatisfaction, adolescent inpatients.
]]>RESUMEN
Introducción
Desde las primeras descripciones de los trastornos alimentarios, los investigadores han encontrado que las familias de las pacientes con anorexia nerviosa o bulimia nerviosa presentan un alto nivel de disfunción familiar. Sin embargo, aún no se ha establecido qué síntomas se encuentran más relacionados con el grado de disfunción o con la calidad del ambiente familiar en este tipo de pacientes.
Objetivo
Describir la frecuencia de los trastornos de la conducta alimentaria, incluyendo los trastornos de la conducta alimentaria no especificados, en una muestra de pacientes adolescentes hospitalizadas por diversos tipos de psicopatología; y establecer el tipo de relación existente entre el funcionamiento-calidad del ambiente familiar y la gravedad y características de la psicopatología alimentaria.
Material y métodos
El estudio incluyó a un grupo de 36 pacientes mujeres adolescentes hospitalizadas debido a cualquier tipo de psicopatología en el Hospital Psiquiátrico Infantil Dr. Juan N. Navarro.
Se realizó la entrevista Mini-Kid para determinar las categorías diagnósticas presentes en la muestra (los trastornos de la conducta alimentaria no especificados fueron diagnosticados a través de una entrevista no estructurada basada en los criterios del DSM-IV). Además, se aplicó el Eating Disorder Inventory, la Subescala de Funcionamiento General de la Familia, la Escala del Ambiente Familiar Global y la Escala de Figuras de Niños.
Resultados
]]> El 39% de la muestra presentó un trastorno alimentario (17% un trastorno específico y 22% un trastorno no especificado), el 42% presentaba únicamente insatisfacción corporal y sólo el 19% de la muestra se encontraba libre de psicopatología alimentaria.El grupo con disfunción familiar (puntuación en la Subescala de Funcionamiento General de la Familia ≥2.17) presentó una mayor tendencia a cursar con episodio depresivo mayor y fobia social en contraste con el grupo sin disfunción familiar, con una diferencia estadísticamente significativa (p<0.05).
El grupo de pacientes con alta-moderada calidad del ambiente familiar (puntuación en la Escala del Ambiente Familiar Global ≥70) no mostró diferencias estadísticamente significativas con el grupo de baja calidad del ambiente familiar en cuanto a los trastornos de la conducta alimentaria y el resto de las categorías diagnósticas obtenidas por el Mini-Kid.
Se encontró una correlación positiva (r=0.34) entre la puntuación total del Eating Disorder Inventory y la puntuación de la Subescala de Funcionamiento General de la Familia (p<0.05). La subescala del Eating Disorder Inventory que tuvo mayor correlación fue la de sintomatología bulímica (r=0.51), seguida por la de inefectividad y baja autoestima (r=0.43), ambas estadísticamente significativas (p<0.01).
Conclusiones
Los trastornos de la conducta alimentaria representan una importante causa de morbilidad en las poblaciones clínicas de mujeres adolescentes; asimismo, los trastornos de la conducta alimentaria no especificados superan en prevalencia a la anorexia nerviosa y la bulimia nerviosa.
La disfunción familiar es una variable que se relaciona con la gravedad de los trastornos de la conducta alimentaria, principalmente los síntomas bulímicos y la baja autoestima. Este hallazgo resulta relevante ante el hecho de poder determinar qué grupo de síntomas podrían mejorar inicialmente con una intervención familiar encaminada a tratar un trastorno alimentario.
Al parecer, la calidad del ambiente familiar medido de forma retrospectiva no tiene un impacto específico en la presencia de un trastorno alimentario, lo que puede quizá solamente propiciar la presencia de variables mediadoras que se relacionen con la generación de psicopatología.
Palabras clave: Ambiente familiar, funcionamiento familiar, trastornos de la conducta alimentaria, insatisfacción corporal, adolescentes hospitalizados.
]]> INTRODUCCIÓN
No cabe duda que los trastornos de la conducta alimentaria han venido a formar parte de una transición epidemiológica de la cual hemos sido testigos en los últimos años.
Diversos autores1 han encontrado que las familias de pacientes con trastornos de la conducta alimentaria tienden a diferenciarse de las familias controles principalmente por presentar mayores conflictos, mayor desorganización familiar, deficientes cuidados de los padres hacia los hijos, presencia de sobreprotección de uno de los padres, menor orientación hacia las actividades recreativas y menor apoyo emocional.
Minuchin2 describió la interacción típica de las familias de pacientes con anorexia en quienes encontró la presencia de límites poco definidos entre sus miembros, tendencia a la negación y a evitar la resolución de conflictos. Denominó a estas familias «psicosomáticas» pues las consideraba un terreno fértil para la respuesta somática.
Kinzl et al.3 estudiaron a 202 mujeres de la población general a quienes se aplicó el Eating Disorder Inventory (EDI) y el Biographie Inventory for Diagnosis of Behavioral Disturbances. Tras analizar los resultados, los autores sugirieron que un ambiente familiar adverso podría representar un importante factor etiológico para el desarrollo de un trastorno de la conducta alimentaria.
Tras aplicar el Family Adaptability and Cohesion Scales y el Parent-Adolescent Communication Form, Vidovic et al.4 encontraron que las pacientes con trastornos alimentarios consideraban a sus familias con menor cohesión y menor adaptabilidad que la percepción que tenían de sus familias un grupo de controles. Además, las pacientes percibieron la comunicación con sus madres como alterada. Las madres de las pacientes percibieron también menor cohesión y flexibilidad en su familia con respecto a las madres de los controles.
Es importante tomar en cuenta que los padres de adolescentes que sufren un trastorno de la conducta alimentaria generalmente presentan mayores dificultades en su relación conyugal y un mayor grado de insatisfacción que los padres de adolescentes sin estos trastornos.5
Dare et al.6 han utilizado las puntuaciones del EDI para valorar los progresos en la terapia familiar para pacientes con anorexia nerviosa. Al dar seguimiento por un año a un total de 40 pacientes anoréxicas y a sus familias, concluyeron que las subescalas del EDI son sensibles a los cambios que ocurren durante la terapia familiar de pacientes con anorexia nerviosa.
A pesar de estos hallazgos, aún no se ha establecido qué grupo de síntomas alimentarios se encuentra más relacionado con el grado de disfunción o con la calidad del ambiente familiar en este tipo de pacientes.
]]> MATERIAL Y MÉTODOS
El estudio incluyó a un grupo de 36 pacientes adolescentes hospitalizadas debido a cualquier tipo de psicopatología en la Unidad de Adolescentes Mujeres del Hospital Psiquiátrico Infantil Dr. Juan N. Navarro. La muestra estuvo constituida por todas las pacientes que quisieron participar en el estudio y que cumplieron los criterios de inclusión: ser paciente del sexo femenino, tener una edad comprendida entre 10 y 17 años y desear participar en el estudio. Los criterios de exclusión fueron: tener alguna deficiencia cognitiva incapacitante, presentar síntomas psicóticos al momento de realizar las evaluaciones y no saber leer o escribir.
Los padres o responsables legales de las pacientes firmaron una carta de consentimiento bajo información. El proyecto fue aprobado por la División de Investigación del Hospital Psiquiátrico Infantil Dr. Juan N. Navarro.
Se aplicaron los siguientes instrumentos a las pacientes participantes:
Inventario de Trastornos Alimentarios (Eating Disorder Inventory). Es un cuestionario autoaplicable diseñado para evaluar rasgos psicológicos y comportamentales comunes a la anorexia nerviosa y a la bulimia nerviosa.7 Consta de 64 reactivos que se agrupan en ocho subescalas diferentes, a saber: impulso por la delgadez, sintomatología bulímica, insatisfacción corporal, inefectividad y baja autoestima, perfeccionismo, desconfianza interpersonal, conciencia interoceptiva y miedo a madurar. La puntuación total de este cuestionario puede oscilar entre 0 y 192. El EDI ha sido adecuadamente validado en la población mexicana.8,9
Escala del Ambiente Familiar Global (Global Family Environment Scale). Es un instrumento que evalúa la calidad del ambiente familiar de forma retrospectiva, tomando en cuenta el peor ambiente familiar durante un periodo de al menos 12 meses.10 La forma de calificar es con base en un continuo hipotético entre el uno y el 90, siendo las puntuaciones más altas (81-90) la descripción de un ambiente familiar estable, seguro y enriquecedor, con una crianza consistente, así como disciplina y expectativas razonables; mientras que las calificaciones más bajas (1-10) reflejan un ambiente familiar muy perturbado. Se ha reportado la confiabilidad de su uso en la versión en español.11 Dicho instrumento se ha utilizado para estudiar población mexicana.12
Subescala de Funcionamiento General de la Familia (General Functioning Subscale of the McMaster Family Assessment Device). Este instrumento es una versión abreviada del Family Asessment Device y proporciona una medida del funcionamiento psicológico de la familia que evalúa las dimensiones relacionadas con la resolución de problemas, comunicación, roles, respuestas afectivas, compromiso emocional y control de conducta.13 Consta de 12 reactivos, de los cuales seis reflejan un funcionamiento adecuado y los otros seis un funcionamiento patológico. La calificación final va del 1.0 al 4.0, los puntajes más altos se relacionan con mayor patología familiar. Una puntuación por arriba del percentil 90 es la que corresponde a 2.17, arriba de la cual se considera que la familia es disfuncional. Esta escala ha sido ampliamente utilizada en población mexicana.12,14,15
Escala de Figuras de Niños (Child Figure Rating Scale). Esta escala, diseñada por Collins et al.16 consiste en varias series de dibujos que representan a niños y niñas, así como a mujeres y hombres adultos con diferente peso corporal. Se pide al niño(a) que señale cuál de todas ellas representa mejor la percepción que tiene de su propio peso y figura; posteriormente se le pide que indique cuál de las figuras representa su peso y cuerpo idealizado; finalmente se le pide que señale cuál de las figuras de adultos representa mejor su ideal de peso y figura para el futuro. Al restar la posición numérica que ocupa cada figura idealizada de la figura escogida como el peso y figura real se obtiene un indicador que representa el grado de insatisfacción corporal. Se han publicado los datos relacionados a la confiabilidad y validez de este instrumento.16
Mini-International Neuropsychiatric Interview para niños y adolescentes (MINI-Kid). La MINI es una entrevista diagnóstica estructurada de duración breve que explora, para detección u orientación diagnóstica, los principales trastornos psiquiátricos del Eje I del DSM-IV y la CIE-10. Existen datos publicados sobre su confiabilidad17 y su validez de acuerdo con el SCID.18 La entrevista MINI-Kid fue desarrollada por los mismos autores con la finalidad de contar con un instrumento que fuese más corto y fácil de administrar en comparación con otros aplicables a niños y adolescentes. Utiliza un lenguaje más fácil de entender para este grupo de edad conservando las características esenciales del MINI.19
Se utilizaron los expedientes clínicos de las pacientes con el fin de obtener la información necesaria para evaluar de forma retrospectiva la calidad del ambiente familiar. Esta información se complementó con una entrevista no estructurada realizada a la paciente en la que se evaluó principalmente los aspectos sugeridos por Rey,20 a saber: estabilidad de la residencia familiar, cambios en las figuras parentales a lo largo del tiempo, disarmonía parental, consistencia y adecuación de la disciplina y de la imposición de límites, consistencia de las expectativas, afecto y cuidados apropiados, pobreza y enfermedades o minusvalías en los padres o hermanos.
]]> La muestra total se dividió en diversos subgrupos (pacientes con trastornos de la conducta alimentaria vs pacientes sin trastornos de la conducta alimentaria; pacientes con disfunción familiar vs pacientes sin disfunción familiar; pacientes con alta-moderada calidad del ambiente familiar vs pacientes con baja calidad del ambiente familiar) cuyas variables fueron comparadas a través de las pruebas t de Student y chi cuadrada. También se utilizó el coeficiente de correlación de Pearson para determinar la correlación existente entre la calidad del ambiente-nivel de funcionamiento familiar y el grado de psicopatología alimentaria.
RESULTADOS
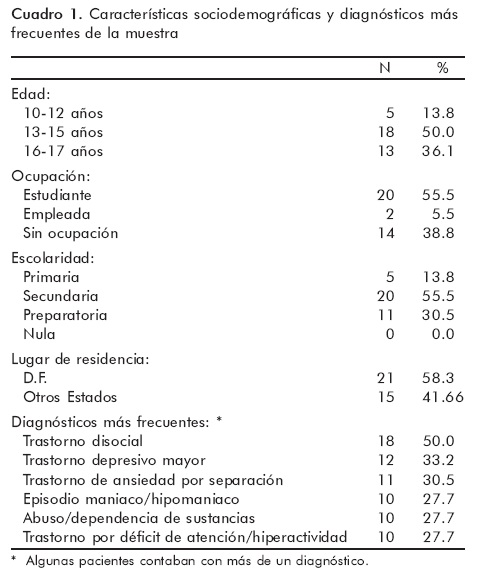
En el cuadro 1 se muestran las características socio-demográficas de las 36 pacientes reclutadas para la realización del presente estudio, así como los diagnósticos más frecuentes de acuerdo con las categorías del Mini-Kid.
La media del número de diagnósticos presentes en cada paciente fue de 4.91, con una desviación estándar de 6.75.
En esta muestra de pacientes hospitalizadas se confirmó la presencia de trastornos de la conducta alimentaria en 39% de los casos: 17% de la muestra correspondía a casos de bulimia nerviosa y 22% a trastornos de la conducta alimentaria no especificados (TANE). No hubo casos de anorexia nerviosa. De la muestra, 42% presentaba algún grado de insatisfacción corporal a pesar de no cumplir criterios para un trastorno alimentario, casi la mitad (46%) de este subgrupo había presentado síntomas relacionados con la conducta alimentaria en el pasado. Solo 19% se encontraba libre de psicopatología alimentaria.
En el cuadro 2 se muestran las medias y desviaciones estándar de la edad, el índice de masa corporal y las puntuaciones de las escalas aplicadas a la muestra. Como puede notarse, la media del índice de masa corporal se situó en el rango normal; sin embargo, esto contrastó con la puntuación del EDI cuya media se encontró por arriba de lo que algunos autores han sugerido como punto de corte para anorexia nerviosa. La media de la puntuación en la Subescala de Funcionamiento General de la Familia se encontró en el límite inferior normal y la Escala del Ambiente Familiar Global mostró una media que correspondería a un ambiente familiar situado entre la categoría de malo y moderadamente insatisfactorio.
]]>
Es de resaltar que un porcentaje elevado de pacientes expresó el deseo de tener un cuerpo más delgado (en promedio, una figura y media de discrepancia con la percepción del peso actual en la Escala de Figura de Niños), y aún más para la vida adulta (en promedio, casi dos figuras de discrepancia con la percepción del peso actual).
La muestra fue dividida en dos grupos: uno de ellos agrupó a las pacientes que cumplían los criterios para un trastorno de la conducta alimentaria (incluidos los TANE) y el otro grupo incluyó al resto de las pacientes. El cuadro 3 muestra los resultados de la prueba t de Student aplicada a estos grupos. Como puede notarse existen diferencias estadísticamente significativas entre ambos grupos en la puntuación total del EDI (p<0.01), así como algunas de sus escalas (p≤0.01) y en la insatisfacción corporal tanto actual como a futuro (p<0.01).
También se realizó la prueba de chi cuadrada para determinar si existían diferencias en las frecuencias de los diagnósticos proporcionados por el Mini-Kid en cada uno de estos subgrupos, pero el análisis no mostró diferencias estadísticamente significativas.
Para determinar si existían diferencias significativas en cuanto a la frecuencia de cada una de las categorías diagnósticas proporcionadas por el Mini-Kid en relación con el funcionamiento familiar, se decidió dividir el total de la muestra en dos subgrupos, uno de ellos con disfunción familiar (puntuación en Subescala de funcionamiento General de la Familia ≥2.17) y otro sin disfunción familiar (puntuación <2.17). Como se observa en el cuadro 4, el grupo con disfunción familiar presentó una mayor tendencia a cursar con episodio depresivo mayor y fobia social, con una diferencia estadísticamente significativa (p<0.05). El resto de los diagnósticos no mostró diferencias.
Para determinar si existían diferencias significativas en cuanto a la frecuencia de cada categoría diagnóstica proporcionada por el Mini-Kid, esta vez en relación con la calidad del ambiente familiar medido de forma retrospectiva por la Escala del Ambiente Familiar Global, se decidió dividir el total de la muestra en dos subgrupos, uno de ellos con alta-moderada calidad del ambiente familiar (puntuación ≥70) y otro con baja calidad del ambiente familiar (puntuación <70). El análisis no arrojó diferencias estadísticamente significativas.
Finalmente se realizó la prueba de Correlación de Pearson para estimar el grado de asociación entre la sintomatología alimentaria medida por el EDI y las variables relacionadas con la familia (funcionamiento y calidad del ambiente). Como se observa en el cuadro 5, existió una correlación positiva estadísticamente significativa entre la puntuación obtenida en la Subescala de Funcionamiento General de la Familia y la puntuación del EDI (p=0.03). Las subescalas que mayor correlación tuvieron fueron las de sintomatología bulímica (p=0.001) y la de inefectividad y baja autoestima (p=0.009).

No se encontró correlación entre el EDI y la Escala del Ambiente Familiar Global.
]]>DISCUSIÓN
Los resultados obtenidos en la presente investigación muestran la elevada prevalencia de trastornos de la conducta alimentaria en una población clínica hospitalizada (39% de la muestra), en la cual los TANE superaban en frecuencia a las formas específicas. Cabe señalar que menos de 20% de la muestra se encontraba libre de algún trastorno de la conducta alimentaria y estaba además conforme con sus dimensiones corporales.
Los TANE han sido subestimados en la investigación, pese a que se ha reportado que representan hasta tres cuartas partes del total de trastornos alimentarios en poblaciones no clínicas.21 En la muestra reclutada para el presente estudio se encontró que los TANE representan 56% del total de los trastornos alimentarios. Si bien los TANE pueden representar formas iniciales de trastornos específicos, cuya pronta detección podría influir en su futuro desarrollo, también pueden representar trastornos de gravedad considerable. Un hallazgo relevante que apoya esta postura se obtuvo al estudiar una muestra de mujeres mexicanas en el Instituto Nacional de Psiquiatría. Aquellas que presentaban un TANE tuvieron una puntuación media en el EDI más alta que la que correspondía a las pacientes con anorexia nerviosa restrictiva y muy similar a las pacientes con anorexia nerviosa compulsivo-purgativa.9
Se ha estimado que si se modifican los criterios de los trastornos específicos, casi 40% de los casos de TANE se considerarían anorexia o bulimia nerviosa. Estas observaciones pueden ser la base para la modificación de criterios en posteriores clasificaciones.22
La Escala de Figuras de Niños de Collins evidenció la alta prevalencia de insatisfacción corporal en la población clínica adolescente. Pese a no cumplir con los criterios para anorexia nerviosa, bulimia nerviosa o un TANE, 42% de la muestra deseaba tener un cuerpo más delgado. Este mismo porcentaje fue encontrado por Collins16 al evaluar la insatisfacción corporal en un grupo de niñas (media= 7.9 años) que cursaban los primeros años de educación básica. Aquí cabe señalar que el proceso mismo de la adolescencia puede acompañarse de una gran insatisfacción con la propia apariencia.23
Otro hallazgo relevante fue la alta comorbilidad psiquiátrica presente en el grupo de pacientes con trastornos alimentarios (cada paciente cumplió criterios para seis diagnósticos psiquiátricos en promedio), lo cual nos habla quizá de un grupo específico de pacientes cuyas características no sería posible extrapolar a una población no clínica o a un servicio ambulatorio. La presencia de un trastorno disocial en 64% de las pacientes con trastornos alimentarios (representada principalmente por pacientes con bulimia nerviosa y sus formas atípicas) nos conduce a las afirmaciones de algunos investigadores, que han considerado dividir la bulimia nerviosa en dos subgrupos: uno en que sólo existe la tendencia a presentar comorbilidad con depresión y otro que es altamente comórbido, en que existe la tendencia a presentar, además de depresión, trastorno antisocial de la personalidad, trastornos de ansiedad y consumo de sustancias.24
También se ha reportado que los TANE que se encuentran relacionados con la bulimia nerviosa cursan con mayor comorbilidad que los que se relacionan con la anorexia nerviosa.25 Desde la década de 1990, Lacey26 acuñó el término «bulimia multiimpulsiva» para designar a una variante de la bulimia nerviosa con alta tendencia a conductas impulsivas, principalmente dependencia a sustancias e intentos de suicidio. Cabe señalar que en la muestra reclutada para el presente estudio, 71% de las pacientes con un trastorno alimentario presentaba riesgo suicida de acuerdo con el Mini-Kid.
Resulta importante resaltar el hecho de que la disfunción familiar, estimada por la Subescala de Funcionamiento General de la Familia, marcó una diferencia en cuanto a la frecuencia con que se presentaban los diagnósticos de trastorno depresivo mayor y fobia social. La alta frecuencia de este último diagnóstico (42% de las pacientes con disfunción familiar, en contraste con el 4.7% reportado en la población general por Medina-Mora)27 nos muestra una característica esencial de este subgrupo, el temor a ser expuesto a la burla y la humillación. Estos síntomas podrían contribuir a la exacerbación de un trastorno alimentario, pues es bien sabido que la insatisfacción con el propio peso se acompaña de la creencia de que otros se burlarán. Es de resaltar el hecho de que una de las subescalas del EDI que mayor correlación tuvo con la Subescala de Funcionamiento General de la Familia fue la de inefectividad y baja autoestima.
De acuerdo con los resultados obtenidos, es posible afirmar que la hipótesis que dio origen a este proyecto se confirmó de forma parcial. La gravedad de los síntomas de los trastornos de la conducta alimentaria, medidos por el EDI, tuvo una correlación positiva con el nivel de funcionamiento familiar estimado por la Subescala de Funcionamiento General de la Familia. Sin embargo, no existió una correlación entre el EDI y la calidad del ambiente familiar medido de forma retrospectiva por la Escala del Ambiente Familiar Global. La explicación a ello posiblemente consista en que los síntomas relacionados con los trastornos alimentarios son más reactivos a las características familiares actuales que a aquellas que se presentaron en el pasado. También es posible suponer que el funcionamiento familiar actual se puede ver afectado por la presencia de sintomatología relacionada con los trastornos de la alimentación en uno de sus miembros. No hay que olvidar que al tratarse de una correlación sólo es posible afirmar que hay una asociación entre las variables, sin que sea posible establecer si una variable se comporta como dependiente o independiente.
]]> Un hallazgo relevante del presente estudio es que la subescala de sintomatología bulímica del EDI fue la que mayor correlación tuvo con el funcionamiento familiar, resultando estadísticamente significativa. Podría suponerse que cuanto más alto es el nivel de disfunción familiar mayor tendencia tendrá una adolescente a presentar atracones y vómitos. Desde esta perspectiva podría parecer que los hallazgos de este estudio apoyan la interpretación psicodinámica de la bulimia nerviosa, donde los atracones simbolizan la marcada dependencia hacia figuras significativas y los vómitos el deseo de expulsar un objeto malo introyectado.28 Sin embargo, dada la imposibilidad de hacer inferencias más allá de una simple asociación entre variables, cabría la posibilidad de que por algunos periodos el bajo funcionamiento familiar propiciara los síntomas bulímicos y que en otros periodos dichos síntomas impactaran el funcionamiento familiar creando así un círculo vicioso. Espina et al.5 consideraron la presencia de este proceso circular en la expresión de los trastornos de la conducta alimentaria. Sin embargo, es necesario enfatizar el hecho de que las conductas purgativas (vómitos, uso de laxante o diuréticos) ocurren fuera de la vista de la familia. Igualmente sucede con los atracones como lo expresa el reactivo 61 del EDI «como o bebo a escondidas»; también el DSM-IV se refiere al síntoma de «comer a solas para esconder su voracidad».29Una aplicación posible de estos hallazgos puede consistir en evaluar con el EDI los progresos realizados en terapia familiar en las familias de pacientes con trastornos de la conducta alimentaria, considerando como mejores indicadores del nivel de funcionamiento la subescala de síntomas bulímicos y la de inefectividad y baja autoestima. La puntuación total del EDI puede ser igualmente útil para este fin, recordemos que algunos reactivos de este instrumento evalúan directamente aspectos relacionados con el ambiente familiar. Por ejemplo, el reactivo 13 expresa: «Mi familia sólo valora como buenos los logros o resultados que están por encima de lo habitual», y el 43 expresa: «Mis padres han esperado cosas excelentes de mí».
Dare et al.6 han utilizado el EDI para evaluar los progresos en terapia familiar de las pacientes anoréxicas. Los resultados de la presente investigación pueden hacer recomendable extender dicha aplicación a la totalidad de los trastornos alimentarios, incluidos los TANE.
Posiblemente las puntuaciones obtenidas en la Escala del Ambiente Familiar Global, que considera el peor ambiente familiar vivido por el paciente por un tiempo mayor a un año, influya solamente en la predisposición a la psicopatología y no en la intensidad de los síntomas actuales (al menos en lo que respecta a los trastornos alimentarios). Cabe señalar que la media de edad de la muestra fue de 14.7 años y que en la gran mayoría de las pacientes el peor periodo de tiempo al que estuvieron expuestas en cuanto a calidad del ambiente familiar, había estado presente en los primeros años de su vida. Es posible que estos eventos pasados hayan ejercido su impacto en la psicopatología de las adolescentes de la muestra; sin embargo, no fue posible medir este fenómeno con los instrumentos empleados en el presente estudio.
AGRADECIMIENTOS
Debemos un especial agradecimiento a la doctora Miriam del Valle Ortega, jefe de la Unidad de Adolescentes Mujeres del Hospital Psiquiátrico Infantil Dr. Juan N. Navarro, por el apoyo y las facilidades otorgadas para la realización de esta investigación.
REFERENCIAS
1. Kucharska-Pietura K, Nikolaou V, Masiak M, Treasure J. The recognition of emotion in the faces and voice of anorexia nervosa. Int J Eat Disord 2004;35:42-47. [ Links ]
2. Minuchin S, Rosman BL, Baker L. Psychosomatic families; anorexia nervosa in context. United States of North America: Harvard University Press; 1978. [ Links ]
3. Kinzl J, Traweger C, Guenther V, Biebl W. Family background and sexual abuse associated with eating disorders. Am J Psychiatry 1994;151:1127-1131. [ Links ]
4. Vidovic V, Juresa V, Begovac I, Mahnik M et al. Perceived family cohesion, adaptability and communication in eating disorders. Eur Eat Disorders Rev 2005;13:19-28. [ Links ]
5. Espina A, Ochoa I, Ortego A. Dyadic adjustment in parents of daughters with eating disorder: Eur Eat Disorders Rev 2003;11:349-362. [ Links ]
6. Dare C, Chania E, Eisler I, Hodes M et al. The Eating Disorder Inventory as an instrument to explore change in adolescents in family therapy for anorexia nervosa. Eur Eat Disorders Rev 2000;8:369-383. [ Links ]
7. Garner D, Olmsted M, Polivy J. Development and validation of a multidimensional Eating Disorder Inventory for anorexia nervosa and bulimia. Int J Eat Disord 1983;2:15-34. [ Links ]
8. García E, Vázquez V, López J, Arcila D. Validez interna y utilidad diagnóstica del Eating Disorder Inventory en mujeres mexicanas. Salud Pública Méx 2003;45:206-210. [ Links ]
9. Unikel C, Bojorquez I, Carreño S, Caballero A. Validación del Eating Disorder Inventory en una muestra de mujeres mexicanas con trastorno de la conducta alimentaria. Salud Mental 2006,29:44-51. [ Links ]
10. Rey JM, Singh M, Hung S, Dossetor DR et al. A global scale to measure the quality of the family environment. Arch Gen Psychiatry 1997;54:817-822. [ Links ]
11. Rey JM, Peng R, Morales-Blanuez C, Widyawati I et al. Rating the quality of the family environment in different cultures. J Am Acad Child Adolesc Psychiatry 2000;39(9):1168-1174. [ Links ]
12. Chan-Díaz G. Ambiente y funcionamiento familiar en adolescentes con depresión. México: Tesis. Universidad Nacional Autónoma de México; 2004. [ Links ]
13. Byles J, Byrne C, Boyle M, Offord D. Ontario Child Health Study: reliability and validity of the general functions Subscale of the McMaster Assessment Device. Fam Proc 1988;27:97-104. [ Links ]
14. Sauceda-Garcia JM, Ortiz-De la Rosa LT, Fajardo-Gutierrez A, Cárdenas-Zetina JA. La adaptación psicosocial en niños y adolescentes con malformaciones craneofaciales. Gac Méd Méx 1997;133(3):203-209. [ Links ]
15. López-Peña MA, Sauceda-García JM, Cuevas-Urióstegui ML. Funcionamiento familiar y su relación con bajo rendimiento escolar, la adaptación psicosocial y psicopatología en adolescentes mayores. Psiquis 2006;15(1):13-23. [ Links ]
16. Collins MA. Body Figure Perceptions and Preferences Among Preadolescent Children. Int J Eat Disord 1991;10:199-208. [ Links ]
17. Sheehan D, Lecrubier Y, Harnett-Sheehan K et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998;59(supl 20):22-33. [ Links ]
18. Sheehan D, Lecrubier Y, Harnett-Sheehan K et al. Reliability and validity of the MINI International Neuropsychiatric Interview (MINI): According to the SCID-P. European Psychiatry 1997;12:232-241. [ Links ]
19. Lecrubier Y, Sheehan D, Weiller E. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. European Psychiatry 1997;12:224-231. [ Links ]
20. Rey JM. Escala del Ambiente Familiar Global (EAFG). Descripción y manual de entrenamiento. Versión española: Victor Peralta, Manuel J. Cuesta, Alfredo Martínez-Larrea; 1997 (manual no publicado, obtenido de forma gratuita directamente con el autor, e-mail: jrey@mail.usyd.edu.au). [ Links ]
21. Machado P, Machado B, Goncalves S, Hoek H. The Prevalence of eating disorders not otherwise specified. Int J Eat Disord 2007;40:212-217. [ Links ]
22. Wilfley D, Bishop M, Wilson G, Agras W. Classification of Eating Disorders: Toward DSM-V. Int J Eat Disord 2007;40:S123-S129. [ Links ]
23. López-Gómez MI. La encrucijada de la adolescencia; psicología de la adolescencia normal. México: Distribuciones Fontamara; 1988. [ Links ]
24. Duncan AE, Neuman RJ, Kramer J, Kuperman S et al. Are there subgroups of bulimia nervosa based on comorbid psychiatric disorders? Int J Eat Disord 2005;37:19-25. [ Links ]
25. Eddy KT, Doyle AC, Hoste RR, Herzog DB et al Eating disorder not otherwise specified in adolescents. J Am Acad Child Adolesc Psychiatry 2008;47:156-164. [ Links ]
26. Lacey JH. Self-damaging and addictive behaviour in bulimia nerviosa. Br J Psychiatry 1993;163:190-194. [ Links ]
27. Medina-Mora ME, Borges G, Lara C, Benjet C et al. Prevalencia de trastornos mentales y uso de servicios: resultados de la encuesta nacional de epidemiología psiquiátrica en México. Salud Mental 2003;26:1-16. [ Links ]
28. Gorjón-Cano S. Aspectos psicodinámicos y sistémicos de los trastornos de la alimentación. Psiquiatría 2001;17(3):89-93. [ Links ]
29. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Cuarta edición. Washington: Masson; 1994. [ Links ]
]]>