Uso inapropiado de fármacos de prescripción: dependencia a benzodiazepinas en adultos mayores
Prescription drugs misuse: benzodiazepine dependence in the elderly
Omar Minaya1, Oscar Ugalde1, Ana Fresán2
1 Clínica de Psicogeriatría. Dirección de Servicios Clínicos. Instituto Nacional de Psiquiatría Ramón de la Fuente.
2 Subdirección de Investigaciones Clínicas. Instituto Nacional de Psiquiatría Ramón de la Fuente.
]]>Correspondencia:
Dra. Ana Fresán.
Subdirección de Investigaciones Clínicas.
Instituto Nacional de Psiquiatría Ramón de la Fuente.
Calz. México–Xochimilco 101,
San Lorenzo Huipulco, 14370,
México DF.
E–mail: fresan@imp.edu.mx
]]> Recibido primera versión: 13 de enero de 2009.
Abstract
Misuse and potential abuse of prescription drugs are growing problems in elderly people over 65 years old. Although the prevalence of this condition is difficult to estimate, drug misuse is most common in elderly women.
A great proportion of the psychoactive prescriptions in old people include tranquilizers and hypnotics. There are several risk factors related to increased risk misuse, abuse, and dependence of prescription drugs. The following are among these risk factors: the female gender, social isolation, history of substance abuse or dependence, history of mental illness and medical exposure to prescription drugs with abuse potential.
Also, BDZ consumption for a period longer than four weeks has also been associated to BDZ dependence, even at therapeutic doses.
Until now, BDZ dependence in the elderly has been poorly studied, so the present study may increase our knowledge of this complex phenomenon.
Objective
]]> The aim of the present study was to describe and compare sociodemographic and clinical features related to the prescription and benzodiazepines use in old people with and without dependence to these drugs in an outpatients psychogeriatric service.Method
A total of 39 patients from the outpatients service at the psychogeriatric clinic of the National Institute of Psychiatry Ramón de la Fuente in Mexico City were recruited. All of the participants signed an informed consent to be included in the study.
Several assessments were performed to determine the psycho–pathological status. Diagnosis of BDZ dependence was obtained with the SCID–I Interview, the severity of depression and anxiety symptoms were evaluated through the Montgomery & Asberg Scale (MADRS) and the Hamilton Anxiety Scale, respectively. For the evaluation of the functionality level, the Katz Index and GAF were used.
Results
No significant differences were found between patients with and without BDZ dependence in terms of social and demographic characteristics and medical comorbidity.
The main Axis I diagnoses of the patients were depressive disorder or anxiety disorders.
The first medical prescription of BDZ in patients with BDZ dependence was the presence of anxiety symptoms, while for patients without BDZ dependence the aim of BDZ prescription was the treatment of insomnia.
The mean age of BDZ use onset and the time of consumption were 57.5 years and 675.2 weeks, respectively. The average dose of BDZ used by the patients was 14.4mg of diazepam equivalents. Significant differences were found between groups in terms of BDZ consumption features. Patients with BDZ dependence exhibited more drug seeking behavior, more abandonment of daily activities, and more tolerance and abstinence symptoms.
Patients with BDZ dependence exhibited more prominent symptoms of anxiety and depression than patients without BDZ dependence. Also, these patients had a poorer cognitive performance and lower psychosocial functioning.
]]> DiscussionBDZ dependence is a complex phenomenon related to the severity of depressive and anxiety symptoms. These symptoms were the main reason for the medical prescription of BDZ.
Although BDZ use was indicated for the treatment of anxiety disorders, the use of BDZ in the elderly has been contraindicated for the treatment of depression with anxiety features.
The potential risk to develop BDZ dependence in elderly patients can be related to pharmacological variations due to changes in the metabolism process of aging and the interactions with other drugs. Both factors could increase half life of BDZ and their pharmacological effect in the organism.
There were statistical differences in the drug–taking pattern of BDZ consumption in the patients. Patients with BDZ dependence had an earlier onset of BDZ consumption and longer use. The chronic use of BDZ is one of the most important risk factors for dependence development.
For the present study, BDZ dependence was clinically defined in terms of tolerance and abstinence symptoms. This definition is in accordance to what has been described in international scientific literature as BDZ physiologic dependence. In this way, tolerance and abstinence symptoms might be the main reason why patients with BDZ dependence needed higher BDZ dosages for the treatment of anxiety symptoms.
Sociodemographic characteristics in this sample were not related to the presence of BDZ dependence; nevertheless, it has been reported that the female gender and the presence of chronic pain are risk factors for BDZ abuse and dependence. Future longitudinal studies with an increased number of patients should assess the effect of these variables in BDZ dependence development in the elderly.
Differences found in terms of cognitive performance may be related to the psychomotor retardation conferred by the use of BDZ, which may in turn have a direct impact on the velocity of mental performance in the patients. Also, the presence and severity of depressive and anxiety symptoms may also have a negative impact on cognitive performance.
Generalization of the findings of the present research is limited by sample size. Nevertheless, the relevance of the present results highlight the importance of the careful prescription and inherent risks related to potentially addictive medications. Increasing our knowledge in the prescription of these medications will improve our medical attention and our patients' quality of life.
Key words: Benzodiazepine dependence, elderly, misuse, depression, anxiety.
]]>Resumen
El abuso potencial y el uso inapropiado de fármacos de prescripción en adultos mayores de 65 años o más está en aumento. Aunque la prevalencia de esta condición es difícil de estimar, se sabe que es más frecuente en mujeres.
Una gran proporción de los tranquilizantes e hipnóticos son prescritos a adultos mayores. El género femenino, el aislamiento social y una historia de abuso de sustancias y de trastornos mentales son los principales factores de riesgo asociados al uso inapropiado de fármacos. Por otro lado, el uso prolongado de benzodiazepinas (BDZ) —mayor a cuatro semanas– también se ha asociado al desarrollo de dependencia, aun cuando las BDZ se utilicen a dosis terapéuticas
Objetivo
El objetivo del presente estudio es describir y comparar las características sociodemográficas y clínicas relacionadas con la prescripción y el uso de benzodiazepinas en adultos mayores con y sin dependencia a las mismas en un servicio especializado de psicogeriatría.
Método
Se reclutó un total de 39 pacientes de la Clínica de Psicogeriatría del Instituto Nacional de Psiquiatría Ramón de la Fuente en la Ciudad de México. Todos los participantes consintieron por escrito su participación en el estudio. El diagnóstico de dependencia a BDZ se realizó a partir del SCID–I; la gravedad de los síntomas de depresión se evaluó mediante la Escala de Montgomery y Asberg (MADRS); los síntomas de ansiedad, con la Escala de Ansiedad de Hamilton (HAM–A), y el nivel de funcionalidad, mediante el Índice de Katz y el GAF.
Resultados
No se encontraron diferencias significativas entre los grupos en las variables sociodemográficas y la comorbilidad médica. Los pacientes incluidos cursaron en su mayoría con un cuadro depresivo o algún trastorno de ansiedad como diagnóstico principal. La indicación médica inicial para el consumo de BDZ fue el tratamiento de la ansiedad para los pacientes con dependencia y del insomnio para los no dependientes. La edad de inicio del consumo de las BDZ y el tiempo de consumo fue de 57.5 años y 675.2 semanas en promedio, respectivamente. La dosis promedio utilizada por los pacientes fue de 1 4.4mg en equivalentes de diazepam.
]]> Los pacientes con dependencia a las BDZ mostraron una mayor gravedad de los síntomas de depresión y ansiedad, menor desempeño cognoscitivo y menor funcionamiento psicosocial, así como conductas de búsqueda y abandono de actividades relacionadas con el consumo y mayores síntomas de tolerancia y abstinencia a las BDZ.Discusión
La dependencia a las BDZ se presentó como un fenómeno complejo relacionado con la intensidad de los síntomas de depresión y ansiedad, un consumo crónico y una mayor dosificación. La depresión con síntomas de ansiedad en el adulto mayor no debería tratarse con BDZ, ya que, además del riesgo de desarrollar dependencia, éstas pueden efectuar negativamente el desempeño cognoscitivo y el funcionamiento global de los pacientes.
Al momento de prescribir una BDZ a la población geriátrica se deben tomar en consideración variables sociodemográficas y clínicas de los pacientes. De la misma forma, será necesario evaluar en futuros estudios la influencia de la personalidad y otras variables clínicas sobre el desarrollo de esta dependencia.
Palabras clave: Dependencia a benzodiazepinas, adulto mayor, uso inapropiado, depresión, ansiedad.
INTRODUCCIÓN
El abuso potencial y uso inapropiado de fármacos de prescripción es un problema creciente1 relacionado con el potencial adictivo de algunos de ellos.2 Aunque la prevalencia del abuso de fármacos de prescripción es difícil de determinar, se sabe que es más prevalente en adultos mayores de 65 años, sobre todo mujeres, que en cualquier otro grupo etario de Estados Unidos.3,4 En 1991, más de un cuarto de los tranquilizantes y un tercio de las benzodiazepinas (BDZ) vendidas para el control de problemas relacionados con dolor, insomnio y ansiedad se prescribieron para adultos mayores, y era más probable que éstos continuaran su uso por un tiempo más prolongado que los individuos más jóvenes.5
El abuso de fármacos de prescripción es un continuum6 con rangos que van desde el uso apropiado con indicación médica hasta el uso inapropiado, con un patrón de abuso persistente y dependencia. En adultos mayores, el abuso y uso inapropiado de BDZ tiene un patrón de consumo cualitativa y cuantitativamente diferente que en los adultos jóvenes, ya que su consumo no va dirigido a experimentar emociones de euforia y generalmente no las obtienen de manera ilegal.7
Las BDZ son un grupo de fármacos frecuentemente prescritos para el control de la ansiedad y el insomnio en adultos mayores, que se han relacionado con un alto riesgo para su uso inapropiado, abuso y dependencia.1,2,.8 En el desarrollo de dependencia a las BDZ9 se presenta uno o más signos de la llamada <<dependencia fisiológica>>, un síndrome residual que aparece cuando se suspende o disminuye su dosificación y tolerancia a los efectos de la sustancia10 cuando se prescriben por más de cuatro semanas,11 incluso a dosis terapéuticas.2
]]> La dependencia a las BDZ en adultos mayores se ha estudiado poco.8 En su abordaje clínico es importante considerar la compulsión subjetiva a su uso, el deseo por dejar de consumirlas, el patrón de uso, las evidencias de neuroadaptación y el alivio y la evitación a la abstinencia, así como el significado que tienen para ellos.10Se han identificado diversos factores de riesgo asociados al uso inapropiado de BDZ en adultos mayores; entre los más reportados se encuentran: el género femenino, el aislamiento social e historia de abuso de sustancias.4 Los adultos mayores con antecedentes de alcoholismo, representan un subgrupo de alto riesgo para el abuso concomitante y dependencia a BDZ.12,13
El objetivo del presente estudio es describir y comparar las características sociodemográficas y clínicas relacionadas con la prescripción y uso de BDZ en adultos mayores, con y sin dependencia a las mismas en un servicio especializado de psicogeriatría.
MÉTODO
Sujetos
Se reclutó un total de 39 pacientes que acudieron de forma consecutiva a la Clínica de Psicogeriatría del Instituto Nacional de Psiquiatría Ramón de la Fuente en la Ciudad de México, que tuvieran como diagnóstico primario un trastorno depresivo mayor o trastorno de ansiedad de acuerdo con criterios diagnósticos del DSM–IV. Todos los participantes dieron su consentimiento informado para participar en el estudio. El estudio fue aprobado por los Comités de Ética y de Investigación del mismo instituto.
Instrumentos
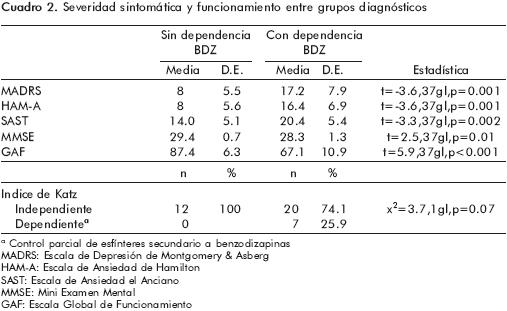
El diagnóstico psiquiátrico de los pacientes y la dependencia a las BDZ se realizó a partir del SCID–I.14 La gravedad de los síntomas de depresión se evaluó mediante la Escala de Depresión de Montgomery y Asberg (MADRS);15–17 los síntomas de ansiedad se evaluaron con la Escala de Ansiedad de Hamilton (HAM–A)18–20 y la Escala de Ansiedad del Anciano (SAST) ;21,22 el estado cognoscitivo actual se evaluó con el Mini Examen Mental (MMSE)23–25 y el nivel de funcionalidad se evaluó mediante el Índice de Katz.26,27 El nivel de funcionamiento global de los pacientes se determinó mediante el GAF.6
Análisis estadístico
]]> La descripción de las características demográficas y clínicas se realizó con frecuencias y porcentajes para las variables categóricas y con medias y desviaciones estándar (±) para las variables continuas. Para examinar las diferencias en las características demográficas, las características clínicas y entre pacientes con y sin dependencia a benzodiazepinas, se utilizó la chi cuadrada ( χ2) para contrastes categóricos y la t de Student para muestras independientes para contrastes continuos. El nivel de significancia se fijó en p<0.05.
RESULTADOS
Características demográficas y clínicas de la muestra
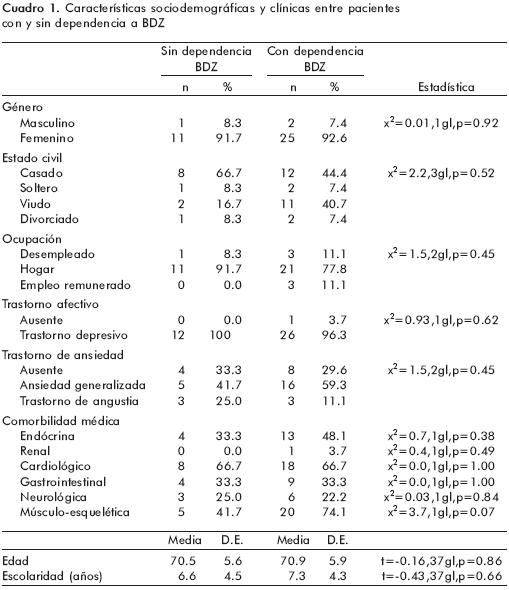
Del total de la muestra, 92.3% (n=36) de los pacientes fueron mujeres y 7.7% (n=3), hombres, con una edad promedio de 70.8±5.8 años (rango 62–83 años). El 51.3% (n=20) de los pacientes se encontraban casados al momento del estudio, seguidos por 33.3% (n=13) que eran viudos, 7.7% (n=3), divorciados y 7.7% (n=3), solteros. El nivel de escolaridad promedio fue de 7.1±4.3 años (rango 0–16) y la principal ocupación eran las actividades del hogar (n=32, 82.1%) seguidas del desempleo (n=4, 10.3%) y el empleo remunerado (n=3, 7.1%).
En cuanto a las características clínicas, 38 pacientes (97.5%) tenían como diagnóstico principal un trastorno depresivo mayor. Hubo uno (2.6%) cuyo diagnóstico principal fue un trastorno de ansiedad. En relación con la presencia de algún trastorno de ansiedad, 53.8% (n=21) cumplieron con los criterios diagnósticos para un trastorno de ansiedad generalizada, seguidos por 15.4% (n=6) con trastorno de angustia. El 30.8% (n=12) de los pacientes no presentaron trastornos de ansiedad.
El 97.4% (n=38) de los pacientes reportaron comorbilidad médica. Los padecimientos cardiológicos (n=26, 66.7%) y músculo–esqueléticos (n=25, 64.1%) fueron los que se reportaron con mayor frecuencia, seguidos de las enfermedades endocrinas (n=17, 43.6%), las gastrointestinales (n=13, 33.3%) y las neurológicas (n=9, 23.1%).
Características del uso de benzodiacepinas
La indicación médica inicial para el uso de BDZ en el total de la muestra fue la presencia de ansiedad (n=23, 59.0%) e insomnio (n=16, 41.0%). La edad de inicio del consumo reportada por los pacientes fue a los 57.5±13.4 años (rango 16–78 años), con un tiempo promedio de consumo de 675.2±630.6 semanas (rango 8–2444 semanas).
Al momento del estudio, 56.4% (n=22) usaban clonazepam, seguidos por 25.6% (n=10) con lorazepam, 7.7% (n=3) con alprazolam y bromazepam, respectivamente, y un paciente con loflazepato de etilo (2.6%). La dosis promedio empleada fue de 14.4±14.8mg de diazepam (rango 1.5–80.0mg).
]]> A partir de la entrevista clínica, 69.2% (n=27) de los pacientes incluidos en el estudio presentaron dependencia a las BDZ. De éstos, 33.3% (n=13) presentaron una dependencia leve, 33.3% (n=13), una dependencia moderada y 2.6% (n=1), una dependencia grave.Características demográficas y clínicas entre pacientes con y sin dependencia a las BDZ
En el cuadro 1 se muestra la comparación de las características demográficas y clínicas entre grupos. No se observaron diferencias significativas entre ellos.
Gravedad de la depresión, ansiedad y funcionalidad entre grupos
Los pacientes con dependencia a las BDZ mostraron una mayor gravedad de los síntomas de depresión y los síntomas de ansiedad en contraste con los pacientes sin dependencia a las BDZ. Por otro lado, los pacientes con dependencia tuvieron un menor desempeño cognoscitivo y un menor funcionamiento psicosocial global (cuadro 2).
Características del consumo de BDZ entre grupos diagnósticos
]]> De acuerdo con la entrevista SCID–I, 92.6% (n=25) de los pacientes con dependencia a las BDZ reportaron haber tenido síntomas de abstinencia a ellas en contraste con 16.7% (n=2) de pacientes sin dependencia (p<0.001). De la misma forma, 59.35% (n=16) de los pacientes dependientes reportaron tolerancia a las BDZ y sólo un paciente (8.3%) sin dependencia reportó tolerancia (p=0.003). Ninguno de los pacientes sin dependencia a las BDZ reportó conductas de búsqueda o abandono de actividades cotidianas, mientras que 22.2% (n=6) y 3.7% (n=1) de los pacientes dependientes reportaron, respectivamente, estas acciones.El 88.9% (n=24) de los pacientes dependientes a las BDZ reportaron haber presentado síntomas residuales tras la reducción o cese del consumo de BDZ en comparación con 25.0% (n=3) de los pacientes sin dependencia. El principal síntoma residual reportado por los pacientes dependientes fue el insomnio (n=21, 77.8%), seguido de la hiperactividad autonómica (n=11, 40.7%), agitación psicomotriz (n=10, 37.0%), incremento en el temblor de manos y ansiedad (n=9, 33.3%, respectivamente) y náusea (n=5, 18.5%). Un paciente reportó la presencia de alucinaciones (3.7%).
La indicación médica inicial de las BDZ para los pacientes sin dependencia fue el insomnio (n=8, 66.7%), mientras que, para los pacientes con dependencia, la indicación médica inicial fue la ansiedad (n=19, 70.4%) (x2=4.7, 1 gl, p=0.03). Los pacientes con dependencia a las BDZ mostraron una edad de inicio de consumo más temprana (54.2±14.1 años vs 65.0±7.6; t=2.4, 37 gl, p=0.01), un mayor tiempo de consumo (878.2± 644.7 semanas vs 218.5 ± 250.4 semanas; t=–4.5, 37 gl, 0<0.001) y una mayor dosis de BDZ en equivalentes de diazepam (17.2±16.5mg vs 7.5±5.6 mg; t=–2.6, 37 gl, p=0.01) en comparación con los pacientes sin dependencia a las BDZ.
DISCUSIÓN
La dependencia a las BDZ se presentó como parte de un complejo fenómeno relacionado con la gravedad clínica de los síntomas de depresión y ansiedad, lo cual influyó en la prescripción médica de BDZ. Aunque el uso de BDZ está indicado en el tratamiento de los trastornos de ansiedad,28 su uso como tratamiento principal o coadyuvante en el manejo de los síntomas de ansiedad asociados a un cuadro de depresión mayor se ha contraindicado en adultos mayores11 por el riesgo de uso inapropiado, abuso potencial y dependencia.1,2
El riesgo de desarrollar un cuadro de dependencia a las BDZ en los adultos mayores es multifactorial y guarda una estrecha relación con las variaciones metabólicas de los fármacos en el envejecimiento, el uso concomitante de otros fármacos y con los cambios por neurosenescencia de los sistemas de neurotransmisión.2,930 Estos factores pueden incrementar la vida media de las BDZ y condicionar una mayor permanencia de los metabolitos en el organismo, así como una mayor susceptibilidad a los efectos de las BDZ, aun a dosis bajas.
Los pacientes con dependencia a las BDZ mostraron diferencias significativas en el patrón de consumo de las mismas con respecto a los pacientes sin dependencia. Fundamentalmente presentaron un inicio del consumo de estos fármacos a una edad más temprana, lo cual condicionó un mayor tiempo de consumo. El uso crónico de BDZ se ha descrito como uno de los principales factores de riesgo para el desarrollo de dependencia.31
En los pacientes estudiados, la dependencia a las BDZ se presentó en términos clínicos de síntomas de tolerancia a los efectos de la sustancia, por lo que tendían a utilizar una mayor dosificación para el control de los síntomas y un cuadro de abstinencia ante la disminución de la dosificación o suspensión del fármaco,32 fenómenos ampliamente descritos en la bibliografía como parte de la dependencia fisiológica a las BDZ,33 incluso a dosis terapéuticas2 como en el presente estudio.
Aunque los factores sociodemográficos y la carga de enfermedad médica no psiquiátrica no se presentaron como factores relacionados para la presencia de dependencia a las BDZ, se puede observar que una alta proporción de los pacientes estudiados fueron mujeres que cursaban con dolor crónico por la presencia de trastornos de origen músculo–esquelético. Ambos factores se han descrito en el abuso y uso inapropiado de las BDZ en adultos mayores.1,4
]]> Los pacientes con dependencia a las BDZ mostraron también un funcionamiento psicosocial menor que los pacientes sin dependencia, además de presentar un menor desempeño cognoscitivo al momento del estudio. Lo anterior puede relacionarse no sólo con la gravedad de los síntomas de depresión y ansiedad,34 sino también con los efectos adversos graves que pueden tener las BDZ sobre la cognición35 y la calidad de vida de los pacientes.36La principal limitación del presente estudio fue el tamaño de la muestra. Estudios futuros deberían incluir un mayor número de sujetos adultos mayores y considerar otras variables, como los rasgos de personalidad, para profundizar en la comprensión de la dependencia a las BDZ en población geriátrica.
La relevancia de la presente investigación radica en resaltar la importancia del ejercicio médico en la prescripción de fármacos con un potencial adictivo y los riesgos inherentes a los mismos. Creemos que una mayor sensibilidad en este tema mejorará la calidad de vida de nuestros pacientes y la calidad de la atención que se les brinda.
CONCLUSIONES
El complejo fenómeno de la dependencia a las benzodiazepinas en los pacientes estudiados se presenta como una condición multifactorial y relacionada con la gravedad de la psicopatología de los pacientes. Tanto la gravedad de los síntomas depresivos y ansiosos como el uso crónico de benzodiazepinas parecen deteriorar el desempeño cognoscitivo y el funcionamiento global de los pacientes. Factores sociodemográficos y clínicos deberían tomarse en consideración en el momento de prescribir benzodiazepinas, las cuales parecen no ser fármacos de primera elección ni coadyuvantes apropiados para el tratamiento de la depresión con síntomas de ansiedad en adultos mayores.
REFERENCIAS
1. Culberson J, Ziska M. Prescription drug misuse/abuse in the elderly. Geriatrics 2008;63(9):22–31. [ Links ]
2. Ashton H. The diagnosis and management of benzodiazepine dependence. Curr Opin Psychiatry 2005;18:249–255. [ Links ]
3. Busto USE, Naranjo C, Cappell H, Sanchez–Craig M, Sykora K. Withdrawal reaction after long–term therapeutic use of benzodiazepines. New England J Medicine 1996;315:854–859. [ Links ]
4. Simoni–Wastia L, Yang H. Psychoactive drug abuse in older adults. American J Geriatric Pharmacotherapy 2006;4(4):380–394. [ Links ]
5. Blow F. Substance abuse among older adults. Treatment Improvement Protocol (TIP) Series, #26. DHHS Publication No. (SMA) 98–3179. Rockville, MD: SAMHSA; 1998. [ Links ]
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Cuarta edición. Washington, DC: 1994. [ Links ]
7. Bartels S, Blow F, Brockmann L, Van Citters A. Evidence–based practices for preventing substance abuse and mental health problem in older adults. Older Americans Substance Abuse and Mental Health Technical Assistance Center. Washington DC: SAMHSA; 2006; p.4–25. [ Links ]
8. Petrovik M, Vandierendonck A, Mariman A, Van Maele G, Afschrift M et al. Personality traits and socio–epidemiological status of hospitalised elderly benzodiazepine users. International J Geriatric Psychiatry 2002;17:733–738. [ Links ]
9. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Tercera edición revisada. Washington, DC: 1987. [ Links ]
10. Baillie A. Manual for the Benzodiazepine Dependence Questionnaire (BDEPQ). South Wales: University of New South Wales; 2001. [ Links ]
11. Harney M. Benzodiazepines: Good Practice Guidelines for Clinicians. En: Children DoHa, ed Roinn Sláinte agus Leanaí; 2002; p. 1–28. [ Links ]
12. Edgell R, Kunik M, Molinari V, Hale D, Orengo C. Nonalcohol–related use disorders in geropsychiatric patients. J Geriatric Psychiatry Neurology 2000;13(1):33–37. [ Links ]
13. Ayuso J. ¿Está justificado el tratamiento prolongado con benzodiacepinas? Salud Mental 2008;31 (6):429–430. [ Links ]
14. First M, Spitzer R, Gibbon M, Williams J. Structured Clinical Interview for DSM–IV Axis I Disorders (SCID–I), Clinician Version. Washington, D.C.: American Psychiatric Press; 1996. [ Links ]
15. Montgomery S, Asberg M. A new depressive scale designed to be sensitive to change. British J Psychiatry 1979;134:382–389. [ Links ]
16. Rosado A. Estudio de confiabilidad de la escala Montgomery–Asberg para la evaluación de la depresión. UNAM, México 1993. [ Links ]
17. Susuki A, Aoshima T, Fukasawa T. A three–factor model of the MADRS in major depressive disorder. Depression and Anxiety 2005;21:95–97. [ Links ]
18. Berlanga C, Canetti A, Chávez E, De la Fuente J, Lara M, et al. Tratamiento farmacologico de las crisis de angustia. Reporte comparativo de la eficacia y seguridad del alprazolam y la imipramina en un estudio controlado. Salud Mental 1991;14:1–5. [ Links ]
19. Hamilton M. The assessment of anxiety states by rating. British J Medical Psychology 1959;32:50–55. [ Links ]
20. Nicolini H, Villareal G, Ortega–Soto H, De la Fuente J. Alteraciones de la memoria de pacientes con crisis de angustia y efecto del tratamiento farmacológico con alprazolam e imipramina. Salud Mental 1988;11:11–14. [ Links ]
21. Saucedo D. Determinación de la confiabilidad y validez de la escala breve para la detección de ansiedad en el anciano [psicogeriatría clínica]. Universidad Nacional Autónoma de México, 2005. [ Links ]
22. Sinoff G, Ore L, Zlotogorsky D, Tamir A. Short anxiety screening test–a brief instrument for detecting anxiety in the elderly. International J Geriatric Psychiatry 1999;14:1062–1071. [ Links ]
23. Becerra B, Ortega–Soto H, Torner C. Validez y reproductibilidad del examen cognoscitivo breve (Mini–mental State Examination) en una unidad de cuidados especiales de un hospital psiquiátrico. Salud Mental 1992;15:41–45. [ Links ]
24. Anthony J, Reche L, Niaz V, Von–Korff M, Folstein M. Limits of the Mini Mental State as screening test for dementia and delirium among hospital patients. Psychological Medicine 1982;12:397–408. [ Links ]
25. Folstein M, Folstein S, McHugh P. Mini Mental State Examination. A practical method for grading the cognitive state of patients for the clinitian. J Psychiatric Research 1975;12:189–198. [ Links ]
26. Alvarez–Solar M, Alaiz–Rojo A, Brun–Gurpegui E, Cabaneros J, Calzon–Frechoso M et al. Functional capacity of patients over 65 according to the Katz index. Reliability of the method. Atencion Primaria 1992;10:812–816. [ Links ]
27. Katz S, Moskowitz R, Jackson B, Jaffe M. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psycho–social function. JAMA 1963;85:914–919. [ Links ]
28. Nutt D. Overview of diagnosis and drug treatments of anxiety disorders. CNS spectrums 2005;10:49–56. [ Links ]
29. Catterson M, Preskorn S, Martin R. Pharmacodynamic and pharmaco–kinetic considerations in geriatric psychopharmacology. Psychiatric Clinics North America 1997;20(1):205–218. [ Links ]
30. Dowling G, Wiess S, Condon T. Drugs of abuse and the aging brain. Neuropsychopharmacology 2008;33:209–218. [ Links ]
31. Ator N, Griffiths R. Principles of drug abuse liability assessment in laboratory animals. Drug Alcohol Dependence 2003;70:S55–S72. [ Links ]
32. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Cuarta edición revisada.Washington, DC: 2000. [ Links ]
33. Woods J, Katz J, Winger G. Benzodiazepines: Use, abuse and consequences. Pharmacological reviews 1992;44:151–347. [ Links ]
34. Austin M, Mitchell P, Wilhelm K, Parker G, Hickie I et al. Cognitive function in depression: A distinct pattern of frontal impairment? Psychological Medicine 1999;29:73–85. [ Links ]
35. Paterniti S, Dufouil C, Alperovitch A. Long–term benzodiazepine use and cognitive decline in the elderly: the Epidemiology of Vascular Aging Study. J Clinical Psychopharmacology 2002;22(3):285–293 [ Links ]
36. Stein M, Barrett–Connor E. Quality of life in older adults receiving medications for anxiety, depression, or insomnia: findings from a community–based study. American J Geriatric Psychiatry 2002;10(5) :568–574. [ Links ]
NOTAS
* Artículo sin conflicto de intereses
]]>