
Facility-based care for delivery and management of complications related to pregnancy and childbirth in Mexico
Bernardo Hernández, DScI, II; Eduardo Ortiz-Panozo, MScII; Ricardo Pérez-Cuevas, DSc.III
IInstitute for Health Metrics and Evaluation. University of Washington. USA
IICentro de Investigación en Salud Poblacional. Instituto Nacional de Salud Pública. México
IIIUnidad de Investigación en Epidemiología y Servicios de Salud. Centro Médico Nacional Siglo XXI. Instituto Mexicano del Seguro Social. México
ABSTRACT
OBJECTIVE: To describe the incidence and management of severe maternal and newborn complications in selected health facilities in Mexico.
MATERIALS AND METHODS: As part of the WHO Multicountry Survey on Maternal and Newborn health, information was collected from medical records of women with deliveries and/or severe maternal complications during pregnancy or puerperium in 14 hospitals in Mexico City and the state of Guanajuato, Mexico.
RESULTS: Of 13 311 women, 157 (12 per 1 000 live births) had severe maternal complications including 4 maternal deaths. The most frequent complications were preeclampsia, postpartum hemorrhage, and chronic hypertension. Adverse perinatal outcomes were more frequent among women with severe maternal complications. A high use of uterotonics and parenteral antibiotics was found. A small proportion of women with eclampsia received magnesium sulfate.
CONCLUSION: This study provides indicators on the incidence and management of maternal and neonatal complications in Mexico, which may be useful in studying and evaluating the performance of obstetric services.
Key words: maternal mortality; pregnancy complications; puerperal disorders; Mexico
RESUMEN
OBJETIVO: Describir la incidencia y manejo de complicaciones maternas y neonatales severas en hospitales seleccionados de México. ]]>
MATERIAL Y MÉTODOS: En el marco de la Encuesta Multipaís de la OMS sobre Salud Materna y Neonatal, se recolectó información de los expedientes médicos de las mujeres que tuvieron su parto o experimentaron complicaciones maternas severas durante el embarazo o puerperio en 14 hospitales de la Ciudad de México y el estado de Guanajuato, México.
RESULTADOS: De 13 311 mujeres, 157 (12/1 000 nacidos vivos) tuvieron complicaciones maternas severas, incluyendo 4 muertes maternas. Las complicaciones más frecuentes fueron preeclampsia, hemorragia postparto e hipertensión crónica. Los resultados perinatales adversos fueron más frecuentes en las mujeres con complicaciones severas. Hubo un uso amplio de uterotónicos y antibióticos parenterales. Una baja proporción de mujeres con eclampsia recibió sulfato de magnesio.
CONCLUSIONES: Esta encuesta proporciona indicadores sobre la incidencia y manejo de las complicaciones maternas y neonatales en México, los cuales pueden ser de utilidad para estudiar y evaluar el desempeño de los servicios obstétricos.
Palabras clave: mortalidad materna; complicaciones del embarazo; trastornos puerperales; México
Maternal and neonatal mortality are important health priorities worldwide. It was forecasted that 273 500 maternal deaths and 2.8 million neonatal deaths would occur worldwide in 2011.1 The reduction of both maternal and child mortality have been set as two of the eight Millennium Development Goals,2 helping to fuel interventions to improve maternal, neonatal, and child health.3,4 Nevertheless, progress towards achieving such goals varies substantially from country to country.1,5,6
In 2010, Mexico had a maternal mortality ratio of 51.1 per 100 000 live births7 and an infant mortality rate of 14.2 per 1 000 live births. 8 In 2006, 38.1% of women began prenatal care in first trimester of pregnancy,9and 93% of deliveries were attended by health professionals, mainly medical doctors.10 The cesarean section rate among adult women who had a live birth in the five preceding years was 37.6%.10
Quality of care plays an important role in reducing maternal and neonatal mortality. Increasing care for delivery and obstetric emergencies has been recognized as a key intervention for reducing maternal mortality.3,4,11 This is substantiated by a growing body of evidence from research studies on maternal deaths. However, it is possible to learn about the effectiveness of interventions to improve maternal health by focusing not only on maternal deaths, but also on the near-misses, which are cases of women who nearly died as a result of severe complications related to pregnancy or delivery.12 This approach is also useful to analyze neonatal health.
In 2005, the World Health Organization (WHO) launched a global survey (WHOGS), which obtained information to construct criteria for the definition of maternal and neonatal near-misses;13-16 in 2010 it began data collection for a second wave, called Multicountry Survey on Maternal and Newborn health (WHOMCS). The objective of this survey was to analyze the incidence and management of maternal and neonatal complications associated with maternal and neonatal mortality in a sample of hospitals around the world. In this paper we present the general results of WHOMCS in Mexico, describing the main characteristics of delivery care and the incidence and management of severe maternal and newborn complications in selected health facilities.
]]>Materials and methods
WHOMCS is a large facility-based survey being implemented in 370 hospitals around the world. The survey is a multicountry, multicenter near-miss criterion-based clinical audit based on hospital records review being implemented between 2010 and 2012, as described elsewhere.17
Population and sample
WHOMCS aimed to collect data on all births and all cases with severe maternal complications which have occurred over a period of time in selected hospitals. In each country, the capital was included with certainty in the sample, and two states were selected at random. In Mexico, for logistic reasons only one state was included, and therefore two study sites were selected: the country's capital (Mexico City) and the State of Guanajuato. Within each study site, 7 hospitals were selected with a probability of selection proportional to their annual number of births. No other criteria were considered in the selection of hospitals. The final sample was made up of 14 facilities: 1 tertiary and 5 secondary hospitals from the Ministry of Health (MoH), 3 tertiary and 3 secondary hospitals from the Mexican Institute of Social Security (IMSS), and 2 private sector hospitals.
The study sample included all deliveries and cases of severe maternal complications treated in the participating hospitals within 2-3 months after August 2010. The data collection period was 2 months for 5 facilities with >6 000 annual births and 3 months for 9 facilities with < 6 000 annual births.17
All women giving birth in the participating hospitals and their respective newborns were eligible. All maternal near-miss cases admitted in the participating hospitals for up to seven days postpartum/postabortion as well as all maternal deaths taking place in the participating hospitals up to seven days postpartum/ postabortion (regardless of the gestational age and delivery status) were also eligible.17 Women referred from other hospitals were included only if they were a maternal death or a near-miss case.
Procedure
The general study was coordinated by WHO in Geneva and in the Latin American participating countries by the Centro Rosarino de Estudios Perinatales (CREP). Data collection in Mexico was coordinated by the National Institute of Public Health (INSP) and by IMSS. The study protocol and the standardized data collection instruments were approved by the research and ethics committees of WHO, MoH, IMSS, and INSP, as well as by participant hospitals when required.
Information at the individual level was collected using a standardized format.17 Trained personnel reviewed all hospital records of eligible women who were discharged from the participating hospitals the previous day during the data collection period. Data related to delivery, complications and care and medications provided were collected. Data collected were entered into a web-based online data entry system.17 CREP monitored data quality. Data queries were addressed by comparing the data collected with their respective hospitals records.
]]> DefinitionsWe defined a maternal near-miss case as a woman presenting at least one of the 25 WHO near-miss identification criteria at delivery/abortion, antepartum or within seven days postpartum/postabortion. The WHO near-miss identification criteria are based on cardiovascular, respiratory, renal, coagulation/hematologic, hepatic, neurologic, and uterine dysfunctions.12-15,17 Severe maternal outcome (SMO) was defined as the case of a woman who either died or was a near-miss.
Eligible women were classified asantepartum, delivery, postpartum, or abortive outcome: Antepartum referred to women who were still pregnant when discharged; Delivery included all women who gave birth; Postpartum included all women who were admitted anytime within seven days after delivery; Abortive out-come was defined as the presence of any of the following: ectopic pregnancy, abortion, product birth weight <500g, or gestational age <22 weeks if product birth weight was unknown.
Statistical analysis
We performed a descriptive analysis focusing on the maternal near-miss indicators as well as the criterion-based clinical audit indicators. Several frequency measures on maternal near-miss cases, maternal deaths, maternal and newborn complications, and outcome and process near-miss indicators were estimated following previously defined analyses algorithms17. The distribution of selected variables was compared between women with and without SMO by chisquare or Fisher's exact tests, as appropriate. The level of significance was 0.05, two-tailed.
Results
Medical record review coverage was 90%, accounting for 13 311 clinical records. Of them, 13 275 (99.7%) were women admitted for delivery. Among them, 12 258 (92.3%) had no complication, 896 (6.8%) had a no near-miss complication (i.e., a complication that was not severe enough to be considered a near-miss), and 121 (0.9%) had SMO. There were 36 women with no delivery in participating facilities, of which 16 (44%) had postpartum severe complication, 10 (28%) had an abortive outcome and 10 (28%) had an antepartum severe complication. SMO occurred in 157 of all women (12 per 1 000 live births).
Maternal characteristics and complications
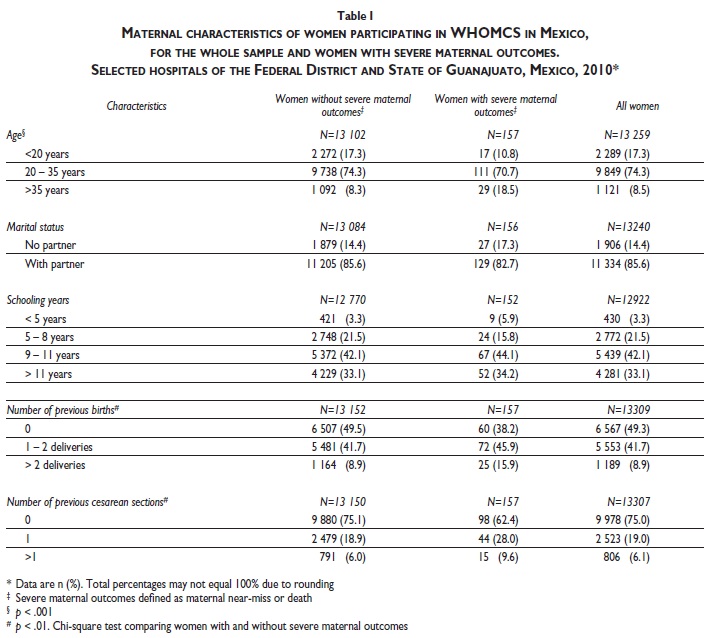
Table I depicts the maternal characteristics. Most women were in the 20-35 age group (74.3%) [range 12-50 years], had a partner (85.6%), and had 9 or more years of schooling (75.2%). Half of them (49.3%) were in their first pregnancy, and 75% had not had previous cesarean section. These distributions were very similar in the group of women with SMO, excepting that 38.2% were in their first delivery and 37.6% had a previous cesarean section.
]]> Table II shows the frequencies of maternal complications (comorbidity may occur). Postpartum hemorrhage, preeclampsia and chronic hypertension were the most frequent. Among women with SMO, postpartum hemorrhage occurred in 40.1% and preeclampsia in 26.8%. Coagulation/hematologic (50%), uterine (41%), and cardiovascular (26%) were the most prevalent organ dysfunctions among women with SMO. Considering the entire sample, frequencies of maternal complications were lower than 1%, except for preeclampsia (3.9%), postpartum hemorrhage (1.7%), and chronic hypertension (1.2%). Hypertensive disorders occurred in 5.3% of all women and in 42.7% of women with SMO.Perinatal outcomes
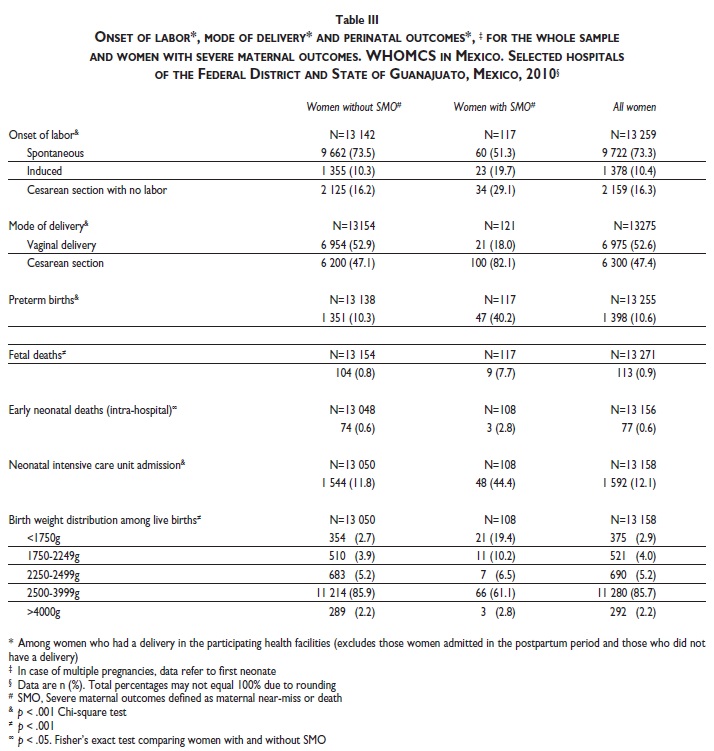
Table III shows the distribution of onset of labor, mode of delivery, and perinatal outcomes. Among all women, 73.3% experienced spontaneous onset of labor, 52.6% had vaginal delivery and 47.4% had cesarean section delivery. Spontaneous onset of labor (51%) and vaginal delivery (18%) occurred at lower percentages among women with SMO. The low birth-weight rate was 121 per 1 000 live births. The proportion of cases with adverse perinatal outcomes (preterm births, fetal deaths, early neonatal deaths, admissions to neonatal care unit and low birth-weight) was higher (roughly 4- to 8-fold) in the SMO group than in the total sample.
Of 10 women who had abortive outcome and SMO, 2 had vaginal delivery, 3 underwent laparotomy for ectopic pregnancy, 4 underwent curettage or vacuum aspiration, and one case was not determined.
Maternal near-miss indicators
Table IV shows the near-miss indicators. One-hundred-fifty-three women had maternal near-miss complications and four died. The maternal near-miss incidence ratio was 11.6 per 1 000 live births. The maternal near-miss mortality ratio (i.e., the ratio between maternal near-miss cases and maternal deaths) was 38 to 1. Organ dysfunction or death occurred in the first 24 hours of hospital stay in 46% of SMO cases (SMO24). Of them, 43% were referred from other facilities. The intra-hospital SMO rate was 6.5 per 1 000 live births. SMO24 and intra-hospital mortality indices were 5.6% and 0.0%, respectively.
Among the 1.6% (211/13 311) of women who were admitted to the intensive care unit (ICU), 36% were women with SMO. The ICU admission rate among women with SMO was 48% and the proportion of maternal deaths without being admitted to the ICU was 25%. Maternal death occurred in 1.4% of women admitted to the ICU.
]]> Process and outcome indicatorsThis survey documented process and outcome indicators related to specific conditions among women who gave birth in participating hospitals (Table V). Oxytocin was widely used to prevent postpartum hemorrhage (PPH) and as a therapeutic measure for severe PPH. Two-hundred-thirteen women had PPH. Of them, 91.5% received uterotonics, 8.9% had intrauterine tamponade or arterial ligation, and 16.9% underwent hysterectomy. About 25% of cases with PPH had organ dysfunction, and one died. Magnesium sulfate was used as an anticonvulsant in 46.7% of the 30 women with eclampsia. Nine of them had organ dysfunction; all survived. Among the 6 295 women who underwent cesarean section, 82.2% received prophylactic antibiotics. Eighty-one out of the ninety-three women who had infection/sepsis received parenteral therapeutic antibiotics. Nine women with infection/sepsis presented organ dysfunction, and one died. Regarding 1 190 women who had preterm delivery after three hours of hospital stay, 37% received corticosteroids for fetal lung maturation.
Discussion
These findings of WHOMCS in selected Mexican hospitals show that the rate of SMO was 12 per 1 000 live births, including 4 maternal deaths; postpartum hemorrhage, preeclampsia, and chronic hypertension were the most prevalent complications; hematologic, uterine, and cardiovascular dysfunctions were the most frequent in women with SMO; adverse perinatal outcomes were more prevalent in women with SMO than in the total sample; and process and outcome indicators on preventive and therapeutic measures for postpartum hemorrhage and infection/sepsis showed better results than indicators for eclampsia and preterm birth.
The maternal near-miss incidence ratio in this study (11.6 per 1 000 live births) contrasts with the findings of WHOGS, which showed ratios of 34.3 and 32.6 per 1 000 deliveries for Latin American countries and Mexico, respectively.15 This difference is probably due to the different definitions of maternal near-miss cases in these two studies. By 2005, the near-miss identification criteria had not yet been developed, and in WHOGS a maternal near-miss was defined as a woman who had experienced admission to ICU, blood transfusion, hysterectomy, eclampsia, cardiac or renal complications.15 The used in WHOMCS are stricter than those of WHOGS (e.g., evidence of organ dysfunction is required instead of the simple registry of admission to ICU).12-15,17 Development of near-miss concept is detailed elsewhere.12
The cesarean delivery rate was 47% for all women and 82% for women with SMO. These results are consistent with the high rates of cesarean deliveries reported in Mexico and other Latin American countries.13,18,19 WHO recommends cesarean delivery rates should be between 5 and 15%,20 and Mexican standards establish they should be around 15 and 20% for secondary and tertiary hospitals, respectively.21 High rates of cesarean delivery might be associated with increased maternal and perinatal morbidity, especially in cases in which cesarean section has no medical indication.13,18 Although the incidence of cesarean section found in this study should be considered with caution due to the characteristics of the sample (discussed later), further analyses are needed to gain better understanding of the impact of high cesarean delivery rates on maternal and perinatal outcomes in Mexico.
The wide use of oxytocin for all women giving birth and prophylactic antibiotics for women who underwent cesarean delivery, but the lower proportion of use of corticosteroids for fetal lung maturation for women who had a preterm delivery after three hours of hospital stay suggest that preventive measures for neonatal respiratory complications are carried out less frequently than preventive measures for PPH and infection/sepsis. In addition, the survey found a high use of uterotonics for women with PPH and parental antibiotics for women with infection/sepsis, compared to the low proportion of women with eclampsia who received magnesium sulfate, despite the efforts of the health sector to promote the use of magnesium sulfate for the treatment of this condition. Moreover the near-miss mortality ratio (i.e., the ratio between maternal near-miss cases and maternal deaths) was 53:1 for PPH in comparison to 9:1 for sepsis. The differences among these indicators should prompt further research studies and intervention.
]]> This study shows the importance of addressing normative aspects, such as quality of care, appropriate use of medications and referral to mitigate or decrease the rate of women with SMO and neonatal complications. Regarding quality of care, the characteristics of women such as their reproductive age and social conditions should be taken into account during antenatal care. In addition some of the complications such as postpartum hemorrhage, sepsis and hypertensive disorders can be identified in a timely manner and even avoided with appropriate risk-assessment during antenatal care and the hospital stay. This survey provide information for clinicians to guide their decision-making process towards a risk-based approach (in which case it would be helpful to search or identify possible complications) vs. reactive-based approach in which their actions are guided to care for ongoing obstetric emergencies. Resolving too early a complicated pregnancy or labor may have deleterious effects on the neonate; the low rate of use corticosteroids for fetal lung maturation shows room for improvement. The analysis of the SMO24 also suggests opportunities for improving the referral system among hospitals. A significant percentage of women with SMO can be reduced with appropriate measures.The study has been supervised by a well-known research team, taking care of the mechanisms to increase data quality in different countries. However, analyzing solely the information from Mexico imposes limitations that should be taken into account when interpreting the results. First, the sample for this study was designed to provide information on the characteristics of delivery care and management of maternal and neonatal complications in the total sample of WHOMCS. Therefore, the sample at the national level is small, especially when trying to study low incidence adverse maternal outcomes. Although the sampling design determined stratification according to the size of the hospital, the study sample does not constitute a representative sample of facilities providing delivery care in Mexico. The characteristics of the sampling design may lead to different estimates of the incidence of complications than the ones we could obtain in a survey with national representativeness. Thus, the estimates derived from this study should not be extrapolated to the national situation or stratified by institution (MoH, IMSS). Despite of these limitations, this analysis provides initial estimates that may be useful for decision makers.
Another limitation is that the data used in this analysis rely on the completeness and accuracy of hospital records and, to some extent, on the expertise of data collectors at interpreting medical information. It is possible that records of cases with complications were not located, and therefore some information was missing, thus leading to underestimate the incidence of complications. Although given the high coverage of medical records reviewed, we would expect it to be minor. There are a number of complex factors that might result in inaccuracy of hospital records. Routine procedures (e.g., antibiotic prophylaxis) might not be fully documented. When severe complications occur, attention might be more focused on providing care than documenting it in hospital records. Completeness of medical records might be a particular issue in the case of women referred from other hospitals, since access to information on situation and procedures provided was only guaranteed after admission to participating hospitals. To minimize the potential errors, CREP monitored data entry by several quality control procedures; all data inconsistencies were clarified and/or amended by checking collected data with corresponding medical records; data collectors were trained before data collection.
The information from this survey, although it does not provide a representative sample of facilities providing delivery care in Mexico, contributes to the general dataset of WHOMCS, which can provide important insights regarding the treatment of maternal and neonatal complications. From a national level standpoint this survey provides data on indicators that may help to characterize and evaluate better obstetric care in Mexico, thus contributing to the efforts aimed at improving quality of care.
Acknowledgements
The Multicountry Survey on Maternal and Newborn Health is a research project implemented by WHO in a global network of health facilities between 2010 and 2012. This project is part of the WHO response to the United Nations Secretary-General call for action for improving women's and children's health around the world. In this connection, the Organization is grateful to the extensive network of institutions and individuals who contributed to the project design and implementation, including researchers, study coordinators, data collectors, data clerks and other partners including the staff from the Ministries of Health and WHO offices. This study is financially supported by the UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction (HRP); WHO; United States Agency for International Development (USAID); Ministry of Health, Labour and Welfare of Japan, and Gynuity Health Projects.
We recognize the participation of the following persons and institutions in this project: Global coordination unit: João Paulo Souza, A Metin Gülmezoglu; Latin American countries coordinator: Guillermo Carroli; Data management and quality control procedures: CREP. We also recognize the collaboration of Dr. Bernardo Bidart (Secretaría de Salud, SSA), Dr. Federico Lazcano (SSA Gobierno del Distrito Federal), Dr. Jorge Aguirre and Dr. Luis García (SSA Estado de Guanajuato) for their support in data collection of this project.
Gloria Galván, María Elena Reyes, Sofía Reynoso, Rafael Rodríguez participated as field supervisors, and Andrea Cerecero, Margarita Torres, Karina Prieto, Karina Castillo, Belén Reyes, Virginia Ramos, Hortensia Gómez and Yenisey Valencia made up the support team.
We specially acknowledge the contribution and support of the following persons in each one of the participating hospitals:
]]> Mexico CityHospital Materno Infantil de Inguarán: Martín Viveros, Carmen Canchola, Laura García, Armando Chávez, Lourdes García, Tomás Pérez, Junne Gil Márquez, María Matilde Cruz, Alejandro Gómez, Israel Aguilar.
Hospital Asoc. Hispano Mexicana CIMIgen Tláhuac:
Carlos Vargas, Sergio Camal, María Micaela López, Rosalva Bolaños.
Hospital de la Mujer: Mauricio Pichardo, Francisco Arévalo, Ana Lilia Chávez, Dalia Zenteno, Adriana Salgado, Evelin Herrera, Ada Contreras.
Hospital de Gíneco-Obstetricia Nº 3 La Raza: Oscar Martínez, María Guadalupe Veloz.
Hospital de Gíneco-Obstetricia Nº 4 Dr. Luis Castelazo Ayala: Gilberto Tena, Carlos Moran, Lizethe Piedras.
Hospital General Manuel Gea González: Octavio Sierra, Lizette Munzo, Arturo Enríquez, Lourdes Suárez, Norberto Reyes.
Hospital Tehuantepec: Carlos Lowemberg, Eduardo Lowemberg.
State of Guanajuato
]]> Hospital General de Zona Nº 2 Irapuato: Alberto Patiño, Mercedes Patiño, Adrian Velázquez, Martha Georgina Franco.Hospital General de Zona Nº 4 Celaya: Faustino Aguilar, David Flores, María Guadalupe Arana.
Hospital General de Zona Nº 3 Salamanca: Juan Guillermo Regalado, José Luis Barrera.
Hospital de Gíneco-Pediatría Nº 48 León: Arturo Estrada, Víctor Godínez, Teresita Ríos.
Hospital General de Irapuato: Julián Valero, José Corrales, Daniel Vázquez.
Hospital General de León: Gregorio del Campo, Juan Carlos Gutiérrez, Leopoldo López.
Hospital General Guanajuato: Raúl Rojas, Norma Angélica Olmos
Declaration of conflict of interests. The authors declare that they have no conflict of interests.
References
]]>1. Lozano R, Wang H, Foreman KJ, Rajaratnam JK, Naghavi M, Marcus JR, et al. Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet 2011;378(9797):1139-1165. [ Links ]
2. United Nations General Assembly. United Nations Millennium Declaration. New York, NY: United Nations, 2000. [ Links ]
3. Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, Lawn JE. Continuum of care for maternal, newborn, and child health: from slogan to service delivery. Lancet 2007;370(9595):1358-1369. [ Links ]
4. McCoy D, Storeng K, Filippi V, Ronsmans C, Osrin D, Matthias B, et al. Maternal, neonatal and child health interventions and services: moving from knowledge of what works to systems that deliver. International Health 2010;2(2):87-98. [ Links ]
5. Institute for Health Metrics and Evaluation. Building Momentum: global progress toward reducing maternal and child mortality. Seattle, WA: Institute for Health Metrics and Evaluation, 2010. [ Links ]
]]>6. Lawn JE, Kerber K, Enweronu-Laryea C, Cousens S. 3.6 million neonatal deaths: what is progressing and what is not? Semin Perinatol 2010;34(6):371-386. [ Links ]
7. Secretaría de Salud. Dirección General de Epidemiología. Sistema Nacional de Vigilancia Epidemiológica. Informe Semanal N° 40 de Vigilancia Epidemiológica de Defunciones Maternas. México: SSA, 2011. [ Links ]
8. Gobierno de los Estados Unidos Mexicanos. Presidencia de la República. Quinto Informe de Gobierno. México: Presidencia de la República, 2011. [ Links ]
9. Secretaría de Salud. Boletín de información estadística. Servicios otorgados y programas sustantivos. México, D. F: SSA, 2009; No. 29, Vol. III. [ Links ]
10. Olaiz-Fernández G, Rivera-Dommarco J, Shamah-Levy T, Rojas R, Villalpando-Hernández S, Hernández-Avila M, et al. Encuesta Nacional de Salud y Nutrición 2006. Cuernavaca, México: Instituto Nacional de Salud Pública, 2006. [ Links ]
]]>11. Campbell OM, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet 2006;368(9543):1284-1299. [ Links ]
12. Say L, Souza JP, Pattinson RC. Maternal near miss: towards a standard tool for monitoring quality of maternal health care. Best Pract Res Clin Obstet Gynaecol 2009;23(3):287-296. [ Links ]
13. Villar J, Valladares E, Wojdyla D, Zavaleta N, Carroli G, Velazco A, et al. Caesarean delivery rates and pregnancy outcomes: the 2005 WHO global survey on maternal and perinatal health in Latin America. Lancet 2006;367(9525):1819-1829. [ Links ]
14. Shah A, Faundes A, Machoki MI, Bataglia V, Amokrane F, Donner A, et al. Methodological considerations in implementing the WHO global survey for monitoring maternal and perinatal health. Bull World Health Organ 2008;86:126-131. [ Links ]
15. Souza JP, Cecatti JG, Faundes A, Morais SS, Villar J, Carroli G, et al. Maternal near miss and maternal death in the World Health Organization's 2005 global survey on maternal and perinatal health. Bull World Health Organ 2010;88(2):113-119. [ Links ]
]]>16. Pileggi C, Souza JP, Cecatti JG, Faundes A. Neonatal near miss approach in the 2005 WHO global survey Brazil. J Pediatr (Rio J) 2010;86(1):21-26. [ Links ]
17. Souza JP, Gulmezoglu AM, Carroli G, Lumbiganon P, Qureshi Z, for WHOMCS Research Group. The World Health Organization multicountry survey on maternal and newborn health: study protocol. BMC Health Services Research 2011;11:286. [ Links ]
18. Villar J, Carroli G, Zavaleta N, Donner A, Wojdyla D, Faundes A, et al. Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study. Br Med J 2007;335(7628):1025. [ Links ]
19. Puentes-Rosas E, Gomez-Dantes O, Garrido-Latorre F. [Caesarean sections in Mexico: tendencies, levels and associated factors]. Salud Publica Mex 2004;46(1):16-22. [ Links ]
20. Chalmers B, Mangiaterra V, Porter R. WHO principles of perinatal care: the essential antenatal, perinatal, and postpartum care course. Birth 2001;28(3):202-207. [ Links ]
]]>21. Norma Oficial Mexicana. NOM-007-SSA2-1993. Atención a la mujer durante el embarazo, parto y puerperio y al recién nacido: Criterios y procedimientos para la prestación del servicio. México: Diario Oficial de la Federación, 1995. [ Links ]
 Corresponding author:
Corresponding author:
Mtro. Eduardo Ortiz-Panozo.
Instituto Nacional de Salud Pública. Av. Universidad 655, col.
Santa María Ahuacatitlán. 62100, Cuernavaca, Morelos, México.
E-mail: eduardo.ortiz@insp.mx
Received on: October 28, 2011 ]]> Accepted on: February 15, 2012
]]>
{kind=link}
{kind=link}