Activated protein C resistance and lupus anticoagulant activity induced by plasma and purified monospecific human IgG anti–β2–glycoprotein–I antibodies
Resistencia a la proteína C activada y actividad de anticoagulante lúpico inducidas por plasma y por anticuerpos purificados humanos del IgG anti β2–glicoproteína I
Martha E. Viveros,** Javier Cabiedes,* Elba Reyes,** Antonio R. Cabral*
* Department of Immunology and Rheumatology. Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán.
** Morphology Department, Escuela Nacional de Ciencias Biológicas, Instituto Politécnico Nacional.
]]>Correspondence and reprint request:
Antonio R. Cabral, MD
Department of Immunology and Rheumatology,
Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán.
Vasco de Quiroga 15,
14000, México, D.F.
Fax (525) 5573–2096.
E–mail: acabral@quetzal.innsz.mx
]]> Recibido el 8 de marzo de 2005.
ABSTRACT
Introduction. We investigated the activated protein C resistance (APCR) phenotype and the lupus anticoagulant (LA), activity induced by anti–β2–glycoprotein–I (anti–β2GP–I) antibodies.
Patients and methods. We studied plasma and sera samples from 29 patients with persistently positive anti–β2GP–I: 22 with thrombosis (12 with primary APS, 10 with APS secondary to SLE) and seven without thrombosis (all with SLE); 25 healthy subjects were studied as controls. We detected anticardiolipin antibodies (ACA); IgG (and its subclasses) and IgM anti–β2GP–I, on irradiated and non–irradiated plates by ELISA. APCR was assessed by the activated partial thromboplastin time (APTT)–based assay and by the modified test. The FV Leiden mutation was studied by PCR. LA determination included screening and confirmatory dRVVT. Serum anti–β2GP–I were affinity purified on sepharose columns and their isotype, subclass, and reactivity against various antigens were studied by ELISA.
Results. We found that titers of IgG anti–β2GP–I on irradiated plates were higher than on non–irradiated plates (p = 0.002), IgG2 was the predominant subclass. Fifteen patients (13 with thrombosis) had LA and 15 (also 13 with thrombosis) induced the APCR phenotype. Eleven (all with thrombosis) had both. Two patients were heterozygous for the Leiden mutation. Two purified antibodies, monospecific for β2GP–I, induced an in vitro APCR phenotype and LA activity.
Conclusions. Our results seem to indicate that the inhibition of the APC anticoagulant function by IgG2 anti–β2GP–I with LA activity may be one of the responsible mechanisms of thrombophilia in patients with APS.
Key words. Antiphospholipid antibodies. Activated protein C resistance. Anti–β2–glycoprotein–I antibodies. Thrombosis.
]]> RESUMEN
Introducción. Investigamos la resistencia a la proteína C activada (RPCA) y la actividad de anticoagulante lápico (AL), inducidas por anticuerpos anti–β2–glicoproteína–I (anti–β2GP–I).
Pacientes y métodos. Estudiamos los plasmas y sueros persistentemente positivos para anti–β2GP–I de 29 pacientes: 22 tuvieron trombosis (12 con síndrome de antifosfolípidos (SAF) primario y 10 con SAF secundario a lupus erítematoso generalizado (LEG)) y siete sin trombosis (todos con LEG). Como controles estudiamos 25 sueros de personas clínicamente sanas. Detectamos anticuerpos anticardiolipina, anti–β2GP–I IgG (y sus subclases) e IgM por ELISA en placas irradiadas y no irradiadas. Evaluamos la RPCA por medio del tiempo parcial de tromboplastina activada y por la prueba modificada. Estudiamos la mutación FV de Leiden por PCR y el anticoagulante lápico con el método de dRVVT screening y confirmatorio. Después de purificar los anti–β2GP–I séricos con una columna de antígeno unido a sefarosa, analizamos por ELISA sus isotipos, subclases y reactividad contra β2GP–I y algunos fosfolípidos.
Resultados. Los títulos de anti–β2GP–I IgG fueron más altos en placas irradiadas que en no irradiadas (p = 0.002), predominó la subclase IgG2. Quince plasmas (13 de pacientes con trombosis) tuvieron AL y 15 (13 también de pacientes con trombosis) indujeron el fenotipo de RPCA. Once plasmas (todos de pacientes con trombosis) indujeron ambas actividades. Dos pacientes fueron heterocigotos para la mutación de Leiden. Dos anticuerpos purificados monoespecíficos para β2GP–I indujeron el fenotipo de la RPCA y la actividad de AL in vitro.
Conclusiones. Nuestros resultados sugieren que la RPCA, inducida por los anti–β2GP–I que concomitantemente tienen actividad de AL, puede tener implicaciones patogénicas en la trombofílía del SAF.
Palabras clave. Anticuerpos antifosfolípidos. Resistencia a la proteína C activada. Anticuerpos anti–β2–glicoproteína–I Trombosis.
INTRODUCTION
The antiphospholipid syndrome (APS), defined as the presence of antiphospholipid antibodies (aPL), venous and arterial thrombosis, recurrent abortions, thrombocytopenia and hemolytic anemia,1 can be found in patients without an underlying disease (primary APS)2–4 or associated with other autoimmune disease, mainly systemic lupus erythematosus (SLE) (secondary APS).15 Recently, it has become apparent that aPL is heterogeneous populations of autoantibodies, some of which react against various phospholipid–binding proteins. These include β2–glycoprotein–I (β2GP–I),6–8 prothrombin,9 high molecular weight kininogen,10 coagulation protein C11 and annexing V.12 Among these, β2–glycoprotein–I, a natural anticoagulant that inhibits the intrinsic blood coagulation pathway13 and the prothrombinase activity of human platelets,14 has been identified as the main antigenic target. This has led to the hypothesis that antibodies to β2GP–I (anti–β2GP–I) interfere with the natural anticoagulant homeostatic properties of β2GP–I, resulting in a thrombophilic state.15–17
The prothrombotic mechanisms of anti–β2GP–I are not well understood, but available evidence suggests that anti–β2GP–I inhibit phospholipid–dependent reactions17 and that this activity depends upon the presence of β2GP–I.18 It has also recently been described that anti–β2GP–I interfere with the protein C pathway and induce an acquired resistance to activated protein C (APC phenotype), that is, anti–β2GP–I inhibit the inactivation of activated Factor V (FVa) by APC on a phospholipid surface.19 Although this finding seems to be independent of the presence of the FV Leiden mutation (APC genotype),19 the prevalence of the Factor V Leiden mutation (APC resistance genotype) has not been widely studied in patients with anti–β2GP–I antibodies.
]]> Antibodies to β2GP–I from APS patients induce lupus anticoagulant activity (LA).20 Together, LA and high levels of anti–β2GP–I antibodies have been proposed as thrombotic risk markers.21–22 Still, the strength of the association of anti–β2GP–I that induce both LA and APCR activities with thrombosis remains to be established.There is still controversy as to the exact nature of the epitope to which antibodies to β2GP–I (anti–β2GP–I) bind. Available evidence suggests that antiphospholipid (aPL) antibodies bind to β2GP–I immobilized on anionic phospholipids6 (or certain oxygen modified synthetic surfaces as irradiated ELISA plates,23 although the existence of antibodies to phospholipid–free β2GP–I in the serum of patients with APS has also been demonstrated.24 IgG isotype of anti–β2GP–I is associated with a higher risk of thrombosis,25 but little is known as to whether any of the IgG subclasses predominates or has any correlation with the clinical behavior of the disease.
To contribute to these issues, we analyzed the anti–β2GP–I isotypes and IgG subclasses on two different plastic surfaces, we studied its coexistance with lupus anticoagulant (LA), acquired APC resistance, and FV Leiden mutation. We also purified anti–β2GP–I antibodies from patients' sera by affinity column and studied their ability to induce APC resistance and LA activity in vitro.
MATERIALS AND METHODS
Patients
We studied 29 patients (25 women) with a median age of 35 years (range 20– 66) and persistently positive IgG anti–β2GP–I antibodies. Twenty–two patients had a history of thrombosis, 12 of them had primary APS2 and 10 had APS secondary1 to SLE.26 Seven of 29 patients had SLE without thrombosis. Twenty–five clinically healthy subjects were studied as controls.
Standard aCL ELISA
Antibodies to cardiolipin (Sigma Chemicals, St Louis, MO, USA) were detected by ELISA as described.27–28
]]>Purification of β2GP–I
β2GP–I was isolated from normal human plasma by a published method29 with some modifications of our own.24 Protein concentration was determined by the method of Bradford30 and its purity was assessed by immunoelectrophoresis in sodium dodecyl sulfate polyacrylamide gel electrophoresis (SDS–PAGE).31
Detection of anti–β2GP–I
Antibodies to highly purified human phospholipid–free β2GP–I were detected by ELISA as described.15 Briefly, β2GP–I was coated on to irradiated and non–irradiated plates (Costar, Cambridge, MA USA). After three washes with 0.05% tween–20 (Bio–Rad, Richmond, CA, USA) in PBS pH 7.2, wells were blocked with PBS containing 1.5% bovine serum albumin (Sigma, BSA). After washing, samples (1:100 in PBS/BSA) were incubated one hour at room temperature, washed and incubated with an alkaline phosphatase conjugated with goat anti–human IgG (anti–y–chain specific), anti–human IgM (anti–p–chain specific) or anti–human IgA (anti–a–chain specific, all from Sigma) for isotype determination; for IgG subclasses determination, we used anti γl, γ2, γ3, and γ4–chain specific (ICN laboratories). After 3 additional washings, color was developed by the addition of p–nitrophenyl phosphate (Sigma) in diethanolamine buffer, pH 9.8. The absorbance was read at 405 nm in a Labsystems Multiskan MS. The ODs of wells containing no antigen were subtracted from all samples. As a positive control, a 1:800 dilution of a rabbit anti–P2GP–I was included while a 1:100 dilution of a pool of 30 normal sera was included as internal negative control. Positive values were considered as > 2 SD of the mean value obtained from 30 normal sample sera.
Purification of anti–β2GP–I
Patient's sera containing high titers of IgG anti–β2GP–I were dialyzed against ethanolamine buffer pH 8.3 for 12 hours. Dialyzed sera were affinity purified on β2GP–I–N–hydroxysuccinimide–activated Se–pharose (HiTrap NHS activated; Amersham Pharmacia Biotech Europe). The coupling of P2GP–I was performed according to the manufacturer's instructions using an automated chromatographer (äkta Prime, Amersham Pharmacia Biotech). The protein/ gel ratio was 5 mg of β2GP–I per mL of gel; the coupling efficiency was measured by the method of Lowry32 which was approximately 90%. Anti–β2GP–I were recovered by acid elution with sodium acetate 0.1M, NaC1 0.5M pH 4.0. Fractions collected were quantified by the method of Lowry and their purity assessed on 10% polyacrylamide on a 7.5% stacking gel, under denaturing conditions to identify light and heavy immunoglobulin chains. Isotype and subclass were determined by ELISA assay as described above. Purified antibodies were also analyzed for antibody activity by ELISA using β2GP–I, prothrombin, cardiolipin, phosphatidylcholine or phosphatidylserine as antigens.
]]> APC resistance phenotype (functional APC resistance)
Resistance to APC was determined in all plasma samples by measuring the prolongation of aPTT in response to activated PC, using Coatest® (Chromogenix, Sweden). Test was considered positive when the ratio of aPTT clotting time of the sample in the presence of APC, by the time obtained using the same plasma in absence of APC, was less than 2.0.33 To overcome the interference of LA, APC resistance was confirmed using the modified aPC–resistance test that includes predilution of patient plasma with factor V depleted plasma34 (Coatest APC Resistance V; Chromogenix, Sweden). Results are reported as APC ratios.
APC resistance assay with affinity–purified anti–β2GP–I
The effect of affinity purified anti–β2GP–I antibodies over the inhibitory activity of APC was measured by mixing the purified anti–β2GP–I with normal pooled plasma (Chromogenix, Sweden) to a final concentration of 0.1 and 0.5 mg/mL, following this, the functional APC resistance assay was determined as described above.
APC resistance genotype (factor V Leiden mutation)
A RFLP analysis for the factor V R506Q gene mutation was performed according to Zoller and Dall–back.35 Briefly, genomic DNA was purified from citrated blood by standard procedures. Mutant Factor V was detected by amplification of the Factor V gene by polymerase chain reaction (PCR). A region of the factor V gene comprising the codon 506 was amplified by PCR, the amplified fragment (241–bp) was subjected to digestion with restriction endonuclease Hind III, generating fragments of 209–bp and 32–bp. The restricted products were separated by elecrophoresis through a 1.2% agarose gel stained with ethidium bromide and directly visualized and photographed under UV light.36
Lupus anticoagulants (LA)
]]> LA were assessed according to the general criteria of the scientific subcommittee for lupus anticoagulants using two–LA tests.37 The simplified dilute Russell's viper venom time test (DVV–test®, American Diagnostica Inc, Greenwich, USA) was first employed. Then, LA were confirmed with the phospholipid confirmatory reagent for Lupus anticoagulant (DVV confirm®). Results were expressed as the ratio of the clotting time result of the DVV test in seconds by the clotting time result of the DVV confirm, > 2SD was considered positive for LA. Normal and abnormal controls were also tested with each batch of samples.
Prothrombin (PT) and activated partial thromboplastin (aPTT) times
The PT and aPTT times were determined in all patients at the Coagulation Laboratory of our Institute in an automated analyzer (Behring Coagulation Timer, Behring Diagnostics). Thromborel S® was used for PT, results were reported in seconds and INR was calculated. Pathromtin® was used for aPTT. Results are expressed in seconds.
Statistical analysis
We compared groups by Student's t test or with X2 when appropriate.
RESULTS
The clinical and demographic characteristics of our patients are shown in table 1.Twenty two of 29 patients had history of thrombosis, 12 patients (41.4%) had primary APS, 10 (34.4%) had APS secondary to SLE. All seven patients without thrombosis had SLE without APS. Venous thrombosis was more frequent than arterial occlusion (77.2% vs. 13.6% respectively), two patients had both (9%). Thrombocytopenia was present in 10 from 22 patients with thrombosis (34.4%) and in two from those without it (6.9%). Only two patients from the thrombosis group had recurrent abortions.
]]> Table 2 shows the serological data of patients with or without thrombosis. Nineteen patients (13 with thrombosis) had IgG aCL and 15 IgM aCL (12 with thrombosis). Fourteen patients had both isotypes and nine patients had neither (data not shown). Of these, fort have been persistently aCL–negative along disease evolution. Table 2 also shows that 15 patients had lupus anticoagulant (13 with thrombosis) and 15 (13 with thrombosis) had the APCR phenotype; 11 patients had concurrent LA and APCR, all had thrombosis while 10 (7 with thrombosis) were negative for both variables. Only two patients were heterozygous for the Factor V R506Q (FV Leiden) mutation.
Anti–β2GP–I titers and isotypes
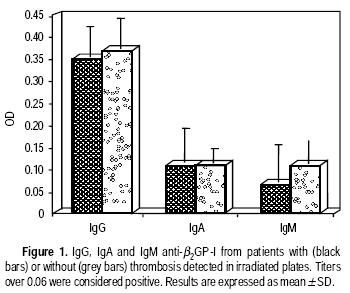
As per inclusion criteria, all patients had IgG anti–β2GP–I detected on non–irradiated plates. Figure 1 shows the titers of IgG, IgA and IgM anti–β2GP–I from patients with or without thrombosis detected in irradiated plates. As seen, IgG anti–β2GP–I titers were not significantly different between the two groups. Titers of IgG anti–β2GP–I from patients with or without thrombosis detected on irradiated plates were significantly higher than those detected on non–irradiated plates (p = 0.002); but anti–β2GP–I titers on non–irradiated plates were always positive (Data not shown). Figure 1 also shows that nine patients (six with thrombosis and three without it) were positive for IgA anti–β2GP–I, 5/9 IgA–positive patients (for with thrombosis) also had IgA anti–β2GP–I in non irradiated plates (Data not shown). All patients were negative for IgM anti–β2GP–I.
The results of the detection of IgGl, IgG2, IgG3 and IgG4 anti–β2GP–I are shown in figure 2. Two patients had IgGl, both had thrombosis. Twenty–eight patients had IgG2 anti–β2GP–I, of these 26 were IgA–positive on non–irradiated plates. None of our patients had IgG3 nor IgG4 anti–β2GP–I on either kind of plate.

]]> Characteristics of affinity–purified anti–β2GP–I antibodies
Anti–β2GP–I antibodies were isolated by affinity chromatography from the sera of 6 patients (for had thrombosis). One total IgG fraction was isolated from a healthy control sera. We found that purified anti–β2GP–I did not react with cardiolipin, phosphatidylcholine, phosphatidylserine or human prothrombin (data not shown). Purified antibodies were mainly of the IgG isotype, but the purified samples also contained IgA, IgM, as well as IgG2 and IgG1 subclasses. Interestingly, one anti–β2GP–I reactied with the native β2GP–I and with the protein modified by cardiolipina (data not shown).
APC resistance phenotype assay with affinity purified antibodies
The effect of three anti–β2GP–I preparations (two from patients with thrombosis and one without it) were tested for their effects on the prolongation of aPTT in response to activated protein C, using both the APTT based assay and the modified assay. At a concentration of 1.0 mg/mL, anti–β2GP–I preparations from patients with thrombosis inhibited the factor Va inactivation by APC by both methods, that is, they induced an in vitro APC resistance phenotype. The anti–β2GP–I isolated from the patient without thrombosis failed to induce the APC resistance phenotype.
DISCUSSION
While the induction of acquired APCR by serum–containing aPL antibodies has been the topic of several reports,19,22,34,38,39 two groups have studied human anti–β2GP–I–containing total IgG fractions to address this issue.19–38 Malia, et al., studied the effect of IgG fractions from 10 plasma samples containing lupus anticoagulant and/or aCL antibodies on the degradation of activated Factor V (FVa) by an activated protein C–protein S complex. Authors found that aPL have an inhibitory effect on the activated protein C/Protein S complex.38 More recently, Galli, et al, studied the effect of affinity–purified IgG phospholipid–dependent inhibitors of coagulation on the time course of FVa generation and inactivation in normal plasma. They found that IgG preparations with anti–β2GP–I activity, but not those with anti–prothrombin activity, hampered the inactivation of FVa by endogenous APC.19 One group has reported that monoclonal murine and human anti–β2GP–I antibodies induce an acquired APCR.40,41 Here, we studied anti–β2GP–I–positive plasmas and found that 15/ 29 induced an in vitro acquired APC resistance (APC phenotype). Ours is the first report that shows that this phenotype is induced by monospecific purified anti–β2GP–I antibodies.
Antibodies to β2GP–I have also been associated with lupus anticoagulant activity. Galli, et al, reported that different laboratory tests may distinguish different populations of lupus anticoagulants, they found that the kaolin clotting time (KCT) associates with anti–prothrombin antibodies meanwhile the diluted Russell's viper venom time (dRVVT) correlates more with anti–β2GP–I.19 More recently, Takeya, et al, studied murine monoclonal antibodies to β2GP–I and found that they inhibit the thrombin generation induced by Russell's viper venom in diluted plasma.41 These authors also reported that this phenomenon was abrogated by the presence of an excess amount of phospholipids, resembling the LA activity, and that this LA activity depends on the anti–β2GP–I epitope specificity.41 In our work, 52% of anti–β2GP–I–positive plasmas showed LA activity by the dRVVT coagulation profile. This agrees with Galli's, et al, contention that the dRVVT profile does not overlap with the ELISA's results in the detection of anti–β2GP–I.42 Taken together all these reports and the current one support the notion that β2GP–I binds to APC and that anti–β2GP–I indirectly inhibits the APC anticoagulant function.19 Recently, Hwang, et al; proposed another pathogenic mechanism of aPL.43 These authors showed that an anti–(pro)thrombin–cross–reactive human monoclonal "aCL" antibody directly binds to APC and inhibits its anticoagulant function in vitro.43
Our work also demonstrated the FV Leiden genotype in 2/29 Mexican patients (7%, both with lupus and APS). This is in agreement with previous studies by Ruiz–Argüelles et al who found this genetic trait in 1 of 22 Mexican Mestizo patients with primary APS,44 and with Davies, et al, in British patients with the same disease.45,46 In Mexico, Ruiz–Argüelles, et al, found the APCR phenotype in 40% of patients with primary thrombophilia, while only 10% of them have the FV Leiden mutation.47 Recently, the same researchers studied other polymorphisms of the FV gene, namely, the HR2 haplotype, Hong Kong, Cambridge and Liverpool mutations in 39 patients with primary thrombophilia.48 Authors concluded that these mutations do not substantially contribute to cause primary thrombophilia in Mexican Mestizo patients.48 It remains to be determined If, apart from anti–β2GP–I, any of the four FV non–Leiden mutations could be responsible for the APCR phenotype detected in APS patients.
]]> The prevalence and clinical significance of IgG anti–β2GP–I in primary and secondary APS have already been defined.16,49 In our study, we found a clear IgG2 restriction of anti–β2GP–I in patients with APS, both on irradiated and non–irradiated plates. Two published studies have analyzed the subclass of IgG anti–β2GP–I. Arvieux, et al, ana Samarkos, et al, found that 87 and 82% of anti–β2GP–I from patients with autoimmune disorders and from SLE and primary APS were of the IgG2 subclass, respectively.50,51 The latter authors also reported that 18 and 9.1% of anti–β2GP–I were IgG3 and IgGl. Our results are in good agreement with both studies. Arvieux, et al., ana ourselves, however, found that IgGl and IgG3 were less represented subclasses of anti–β2GP–I. The sensitivity of the ELISA assays may account for the discrepancies of these results. Of note is that none of the two aforementioned groups of investigators studied the binding of anti–β2GP–I to non–irradiated plates.50,51 Here, we found that, although positive when detected in non–irradiated plates, the binding of plasma–derived or affinity purified IgG2 anti–β2GP–I from patients with or without thrombosis was higher in irradiated plates. These results agree with the notion that anti–β2GP–I react with at least two different epitopes, one present in the native protein and another uncovered by anionic surfaces.16,52 The IgG2 predominance of anti–β2GP–I suggests that the antibody response against β2GP–I may be T–cell independent.It has been suggested that IgA anti–β2GP–I could be good markers for thrombosis.53 Here, we found that 6/22 (27%) patients with thrombosis (3 of them with very high titers) and 3/7 (42%) patients without thrombosis had positive IgA anti–β2GP–I. The difference is not statistically significant, but a larger number of patients is needed to settle this issue. As in previous works from our group,15–24 in the current study we found no IgM anti–β2GP–I in the sera of patients with primary or secondary APS.
More relevant than their isotype, antibodies to β2GP–I with LA activity that concomitantly induce the APCR phenotype may be better markers for thrombophilia. For instance, Potzsch et al. found that 13/14 patients with recurrent thrombotic episodes and 10/19 patients with a single event (altogether 73%), all with LA, had APCR in samples prediluted with factor V deficient plasma.54 In our study, we found that all patients positive for both LA activity and the APCR phenotype had thrombosis. In contrast, all patients without thrombosis were negative for both tests. This finding suggests that the inhibition of the APC anticoagulant function by anti–β2GP–I with LA activity may be one of the responsible mechanisms of the recurrent thrombophilia characteristic of APS patients. More studies are needed to confirm this hypothesis.
ACKNOWLEDGMENTS
This study was supported by a grant from the Consejo Nacional de Ciencia y Tecnología, Mexico.
MSc Viveros' work was supported by scholarships from CONACYT (91197) and from PIFI of the Instituto Politécnico Nacional, Mexico. During the conduction of this study Dr. Cabral was recipient of the Beatriz Vázquez Sámano Career Investigator Award for research on Antiphospholipid/cofactor syndromes. We dedicate this work to our friend and colleague Dr. Donato Alarcón Segovia whose work and dedication in the study of the antiphospholipid syndrome will always be a source of inspiration to us all.
REFERENCES
1. Alarcón–Segovia D, Delezé M, Oria CV, Sánchez–Guerrero J, Gómez–Pacheco L, Cabiedes J, et al. Antiphospholipid antibodies and the antiphospholipid syndrome in systemic lupus erythematosus. A prospective analysis of 500 consecutive patients. Medicine 1989; 68: 353–65. [ Links ]
2. Alarcón–Segovia D, Sánchez–Guerrero J. Primary antiphospholipid syndrome. J Rheumatol 1989; 16: 482–8. [ Links ]
3. Asherson RA, Khamashta MA, Ordi–Ros J, Derksen RHWM, Machin S, Barquinero J et al. The "primary" antiphospholipid syndrome: major clinical and serological features. Medicine 1989; 68: 366–74. [ Links ]
4. Mackworth–Young CG, Loizou S, Walport MJ. Primary antiphospholipid syndrome: features of patients with raised anticardiolipin antibodies and no other disorder. Ann Rheum Dis 1989; 48: 362–7. [ Links ]
5. Cervera R, Piette JC, Font J, Khamashta MA, Shoenfeld Y, Camps MT et al. Antiphospholipid syndrome. Clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum 2002; 46: 1019–27. [ Links ]
6. Galli M, Comfurius P, Maassen C, Hemker HC, de Baets MH, Van Breda–Vriesmen PJC et al. Anticardiolipin antibodies (ACA) are directed not to cardiolipin but to a plasma protein cofactor. Lancet 1990; 335: 1544–7. [ Links ]
7. McNeil HP, Simpson RJ, Chesterman CN, Krilis SA. Antiphospholipid antibodies are directed against a complex antigen that includes a lipid–binding inhibitor of coagulation: β2–Glycoprotein I (apolipoprotein H). Proc Nati Acad Sci (USA) 1990; 87: 4120–4. [ Links ]
8. Matsuura E, Igarashi Y, Fujimoto M, Ichikawa T, Koike T. Anticardiolipin cofactor(s) and differential diagnosis of autoimmune disease (Letter). Lancet 1990; 336: 177–8. [ Links ]
9. Galli M. Non–β52–glycoprotien I cofactors for antiphospholipid antibodies. Lupus 1996; 5(5): 388–92. [ Links ]
10. Sugi T, Mcintyre JA. Autoantibodies to phosphatydilethanolamine (PE) recognize a kininogen–PE complex. Blood 1995; 86: 3083–9. [ Links ]
11. Ruíz–Argüelles A, Vázquez–Prado J, Delezé M, Pérez–Romano B, Drenkard C, Alarcón–Segovia D, et al. Presence of serum antibodies to coagulation protein C in patients with systemic lupus erythematosus is not associated with antigenic or functional protein C deficiencies. Am J Hematol 1993; 44: 58–9. [ Links ]
12. Matsuda J, Saitoh N, Gohchi K, Gotoh M, Tsukamoto M. Anti–annexin V antibody in systemic lupus erythematosus patients with lupus anticoagulant and/or anticardiolipin antibody. Am J Hematol 1994; 47(1): 56–8. [ Links ]
13. Schousboe I. β2–Glycoprotein I: a plasma inhibitor of the contact activation of the intrinsic blood coagulation pathway. Blood 1985; 66: 1086–91. [ Links ]
14. Nimpf J, Bevers EM, Bomans PHH. Prothrombinase activity of human platelets is inhibited by β2– Glycoprotein I. Biochem Biophys Acta 1986; 884: 142–9. [ Links ]
15. Cabiedes J, Cabral AR, Alarcón–Segovia D. Clinical manifestations of the antiphospholipid syndrome in patients with systemic lupus erythematosus associate more strongly with anti–β2–glycoprotein–I than with antiphospholipid antibodies. J Rheumatol 1995; 22: 1899–906. [ Links ]
16. Alarcón–Segovia D, Cabral AR. The antiphospholipid antibody syndrome: clinical and serological aspects. In: Alarcón GS, Catoggio LJ, editors. Balliéres' Clinical Rheumatology. London: Bailliere Tindall; 2000, p. 139–50. [ Links ]
17. Brandt JT. Antibodies to β52–glycoprotein I inhibit phospholipid dependent coagulation reactions. Thromb Haemost 1993; 70: 598–602. [ Links ]
18. Roubey RAS, Pratt CW, Buyon JP, Winfield JB. Lupus anticoagulant activity of autoimmune antiphospholipid antibodies is dependent upon β2–glycoprotein I. J Clin Invest 1992; 90: 1100–04. [ Links ]
19. Galli M, Ruggeri L, Barbui T. Differential effects of anti–β2– glycoprotein I and antiprothrombin antibodies on the anticoagulant activity of activated Protein C. Blood 1998; 91: 1999–2004. [ Links ]
20. Roubey RA. Autoantibodies to phospholipid–binding plasma proteins: A new view of lupus anticoagulant and other "antiphospholipid" autoantibodies. Blood 1994; 84: 2854–67. [ Links ]
21. Carreras LO, Forastiero RR, Martinuzzo ME. Which are the best biological markers of the antiphospholipid syndrome? J Autoimmunity 2000; 15: 163–72. [ Links ]
22. Martinuzzo ME, Forastiero R, Adamczuk Y, Cerrato G, Carreras LO. Activated protein C resistance in patients with anti–β2 glycoprotein I antibodies. Blood Coagul Fibrinol 1996; 7: 702–04. [ Links ]
23. Matsuura E, Igarashi Y, Yasuda T, Triplett DA, Koike T. Anticardiolipin antibodies recognize β2–glycoprotein I structure altered by interacting with an oxygen modified solid phase surface. J Exp Med 1994; 179: 457–62. [ Links ]
24. Cabral AR, Cabiedes J, Alarcón–Segovia D. Antibodies to phospholipid–free β2 glycoprotein–I in the serum of patients with primary antiphospholipid syndrome. J Rheumatol 1995; 22: 1894–8. [ Links ]
25. Galli M, Luciani D, Bertolini G, Barbui T. Anti–β2–glycoprotein I, antiprothrombin antibodies, and the risk of thrombosis in the antiphospholipid syndrome. Blood 2003; 102: 2717–23. [ Links ]
26. Tan EM, Cohen AS, Fries JF, Masi AT, McShane DJ, Rothfield NF et al. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 1982; 25: 1271–7. [ Links ]
27. Loizou S, McCrea JD, Rudge AC, Reynolds R, Boyle CC, Harris EN. Measurement of anticardiolipin antibodies by an enzyme–linked immunosorbent assay (ELISA). Standardization and quantitation of results. Clin Exp Immunol 1985; 62: 738–45. [ Links ]
28. Gharavi AE, Harris EN, Asherson RA, Hughes GRV. Anticardiolipin antibodies: isotype distribution and phospholipid specificity. Ann Rheum Dis 1987; 46: 1–6. [ Links ]
29. Polz E, Wurm H, Kostner GM. Investigations on β2–glycoprotein in the rat: isolation from serum and demonstration in lipoprotein densitiy fractions. J Biochem 1980; 11: 265–70. [ Links ]
30. Bradford MM. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein–dye binding. Anal Biochem 1976; 72: 248–54. [ Links ]
31. Towbin H, Staehelin T, Gordon J. Electrophoretic transfer of protein from SDS and acid/urea polyacrylamide gels to nitrocellulose sheets: procedure and some applications. PNAS 1979; 76: 4350–4. [ Links ]
32. Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin phenol reagent. J Biol Chem 1951; 193: 265–75. [ Links ]
33. Bertina RM. Laboratory diagnosis of resistance to activated protein C (APC–resistance). Thromb Haemost 1997; 78: 478–82. [ Links ]
34. Benattar N, Schved JF, Biron–Andréani C. A new dilution for the modified APTT–based assay for activated protein C resistance: improvement of the reliability in patients with lupus anticoagulant. Thromb Haemost 2000; 83: 967–8. [ Links ]
35. Zöller B, Dallback B. Linkage between inherited resistance to activated protein C and factor V gene mutation in venous thrombosis. Lancet 1994; 343: 1536–8. [ Links ]
36. Gandrille S, Alhenc–Gelas M, Aiach M. A rapid screening method for the Factor V Leiden Arg 506–Gln mutation. Blood Coag Fibrinol 2001; 6: 245–8. [ Links ]
37. Jacobsen M, Barna–Cler L, Triplett DA, Wisloff F. The evaluation of clotting times in the laboratory detection of lupus anticoagulants. Thromb Res 2001; 104: 275–82. [ Links ]
38. Malia RG, Kitchen S, Greaves M, Preston FE. Inhibition of activated protein C and its cofactor protein S by antiphospholipid antibodies. Br J Hematol 1990; 76: 101–7. [ Links ]
39. Bokarewa MI, Blomback N, Rosen S. A new variant of interaction between phospholipid antibodies and the protein C system. Blood Coag Fibrinol 1994; 5: 37. [ Links ]
40. Ieko M, Ichikawa K, Triplett DA, Matsuura E, Atsumi T, Sawada KI et al. β2–glycoprotein I is necessary to inhibit protein C activity by monoclonal anticardiolipin antibodies. Arthritis Rheum 1999; 42: 167–74. [ Links ]
41. Takeya H, Mori T, Gabazza EC, Kuroda K, Deguchi H, Matsuura E, et al. Anti–β2–glycoprotein I (β2GPI) monoclonal antibodies with lupus anticoagulant–like activity enhance the β2GPI binding to phospholipids. J Clin Invest 2003; 99: 2260–8. [ Links ]
42. Galli M, Finazzi G, Norbis F, Marchioli R, Barbui T. The risk of thrombosis in patients with lupus anticoagulants is predicted by their specific coagulation profile. Thromb Haemost 1999; 81(5): 695–700. [ Links ]
43. Hwang KK, Yang CD, Yan W, Gorssman J, Haln B, Chen PP. A thrombin–cross–reactive anticardiolipin antibody binds to and inhibits the anticoagulant function of activated protein C. Arthritis Rheum 2003; 48: 1622–30. [ Links ]
44. Ruíz–Argüelles GJ, Garcés–Eisele J, Alarcón–Segovia D. Activated protein C resistance phenotype and genotype in patients with primary antiphospholipid syndrome. Blood Coag Fibrinol 1996; 7: 344–8. [ Links ]
45. Davies KA, Ireland H, Athanassiou P, Lane D, Walport MJ. Factor V Leiden mutation and venous thrombosis (Letter to the Editor). Lancet 1995; 345: 132–3. [ Links ]
46. Simantov R, Lo S, Salmon JE. Factor V Leiden increases the risk of trombosis in patients with antiphospholipid antibodies. Thromb Res 1996; 84: 523–7. [ Links ]
47. Ruiz–Argüelles GJ, González–Estrada S, Garcés–Eisele J, Ruiz–Argüelles A. Primary thrombophilia in Mexico II: A prospective study. Am J Hematol 1999; 60: 1–5. [ Links ]
48. Ruiz–Argüelles GJ, Poblete–Naredo I, Reyes–Núñez V, Garcés–Eisele J, López–Martínez B, Gómez–Rangel J. Primary thrombophilia in Mexico IV: frequency of the Leiden, Cambridge, Hong Kong, Liverpool and HR2 haplotype polymorphisms in the factor V gene of a group of thrombophilic Mexican Mestizo patients. Rev Invest Clin 2004; 56: 600–4. [ Links ]
49. Sebastiani GD, Galeazzi M, Tincani A, Piette JC, Font J, Allegri F et al. Anticardiolipin and anti–β2GPI antibodies in a large series of European patients with systemic lupus erythematosus. Scand J Rheumatol 1999; 28: 344–51. [ Links ]
50. Arvieux J, Roussel B, Ponard D, Colomb MG. IgG2 subclass restriction of anti–β2 glycoprotein 1 antibodies in autoimmune patients. Clin Exp Immunol 1994; 95: 310–5. [ Links ]
51. Samarkos M, Davies KA, Gordon C, Walport MJ, Loizou S. IgG subclass distribution of antibodies against β2–glycoprotein–1 and cardiolipin in patients with systemic lupus erythematosus and primary antiphospholipid syndrome, and their clinical associations. Rheumatology 2001; 40: 1026–32. [ Links ]
52. Pengo V, Biasiolo A, Fior MG. Autoimmune antiphospholipid antibodies are directed against a cryptic epitope expressed when β2–glycoprotein I is bound to a suitable surface. Thromb Haemost 1995; 73: 29–34. [ Links ]
53. Lewis S, Keil LB, Binder WL, De Bari VA. Standard measurement of major immunoglobulin class (IgG, IgA, and IgM) antibodies to β2glycoprotein I in patients with antiphospholipid syndrome. J Clin Lab Anal 1998; 12: 293–7. [ Links ]
54. Potzsch B, Kawamura H, Preissner KT, Schmidt M, Seeling C, Muller–Berghaus G. Acquired protein C dysfunction but not decreased activity of thrombomodulin is a possible marker of thrombophilia in patients with lupus anticoagulant. J Lab Clin Med 1995; 125: 16–7. [ Links ] ]]>