











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Corneal ulcers are a major cause of corneal blindness that are often underreported but may result in 1.5 to 2.0 million new cases of monocular blindness each year1.
Infectious keratitis is an ophthalmic emergency that threatens the vision and structural integrity of the eye and requires immediate treatment and timely identification of the causative agent, since, without the initiation of appropriate treatment, only 50% of the eyes with microbial keratitis will have good visual results2-4.
The diagnosis is usually based on the clinical features found by slit lamp examination, such as a corneal epithelial defect and stromal infiltration. The evaluation of the depth and extent of the pathological characteristics is subjective and depends on the experience of the examiner5. The monitoring of the response to treatment is through measuring the dimensions of the epithelial defect by slit lamp exam, and with the aid of anterior segment photographs6.
The identification of the causative organism is of great importance; however, although the smear and culture of the corneal lesion remain the gold standard in the diagnosis of infectious keratitis, some microorganisms are difficult to detect in vitro and some others are slow-growing6.
Spectral domain optical coherence tomography (OCT) is an imaging test that has been used to evaluate the anatomical structures and to diagnose pathologies, and has shown excellent reproducibility regarding pachymetry, anterior chamber depth, as well as iridocorneal angle measurements7-9.
Regarding the usefulness of OCT in inflammatory and infectious corneal pathologies, there are several publications that suggest it is a valuable tool to assess the extension of the lesion and to monitor the response to antimicrobial treatment, as well as in the follow-up of corneal pathologies in which is difficult to visualize corneal structures and the anterior segment10-14.
Konstantopoulos, et al. quantified the treatment response of bacterial keratitis and the reduction of corneal edema using time-domain OCT, and demonstrated its usefulness for monitoring, with the limitation of not being able to determine the borders of the infiltrates in 50% of the cases, attributed to the lower resolution of the equipment used10,13.
Wael Soliman, et al. in 2012, aimed to find patterns to identify the causative agent and conducted a study that included 20 patients with infectious bacterial and fungal keratitis, confirmed by cultures. They recorded the changes found by spectral-domain OCT and reported 12 patterns, of which 11 were observed in both bacterial and fungal keratitis, and it was not possible to differentiate the etiology through these patterns. They highlighted a unique pattern in fungal etiology described as “ full thickness stromal cystic spaces” that correlated with stromal necrosis15.
Objective
To distinguish the existence of characteristic corneal morphological patterns, detected by spectral-domain OCT in patients with infectious keratitis.
Methods
A descriptive, cross-sectional, prospective and observational study was carried out in 19 patients from the cornea and refractive surgery department at the Hospital Fundación de Nuestra Señora de la Luz, who were clinically diagnosed with infectious keratitis of bacterial, fungal and viral etiology.
A complete ophthalmological examination was performed, including visual acuity, biomicroscopy and clinical photographs of the lesion, with a minimum of three images with diffuse illumination at a 10X magnification to include the entire corneal lesion and selecting the best image to correlate with the ones obtained by spectral-domain OCT.
One to three images were taken with the high-resolution spectral-domain OCT (Spectralis, Heidelberg Engineering, GmbH, Germany) using the anterior segment module. Patients were asked to keep their eyesight in the fixation light with the contralateral eye to maintain ocular alignment. Using the anterior segment software in the cornea module, version 5.1, a customized study panel was selected, configured with a measurement of 15 mm horizontal by 5 mm vertical, positioned at the center of the corneal lesion, with a quality of 40 frames, resulting in 41 sections of 69 microns each.
From the images obtained, the best image was selected for its morphological description by one of the authors of this work and a cornea specialist, considering hyperreflective and hyporeflective patterns found in the lesion, observing preservation or loss of the normal architecture of the corneal structures, changes in reflectivity at the epithelium and stroma, differentiation between affected and healthy tissue, as well as the visualization of the deep stroma beneath the lesion. The images were compared looking for similar patterns that helped to differentiate between bacterial, fungal and viral etiologies.
After taking the clinical pictures and the spectral-domain OCT, a sample of the lesion was taken with a rayon swab at the borders of the lesion after applying topical anesthesia with tetracaine hydrochloride. Then the swab was placed in a tube with transport medium for processing and performing polymerase chain reaction (PCR).
Results
We included 19 cases of patients with infectious keratitis. PCR reported the cases as 7 bacterial, 5 fungal, 1 viral, and 6 non-reactive. All of them were included and classified by clinical photographs, finding the following patterns:
– Bacterial keratitis: patterns of subepithelial hyperreflectivity in the area of the lesion, loss of differentiation of the epithelial layer and the Bowman layer, stromal hyporeflectivity underlying the lesion, and it was possible to delineate the deep corneal layers in the region adjacent to the lesion and an adequate delimitation of the affected area compared to healthy areas (Figs. 1 and 2).

Figure 1 Bacterial keratitis: hyperreflective subepithelial lesion, loss of differentiation of the epithelial layer and Bowman's layer (asterisk), hyporeflective stroma underneath the lesion, with adequate differentiation between affected and healthy tissue (arrow).

Figure 2 Bacterial keratitis: hyperreflective subepithelial lesion, loss of differentiation of the epithelial layer and Bowman's layer (asterisk), hyporeflective stroma underneath the lesion, with adequate differentiation between affected and healthy tissue (arrow).
– All the bacterial lesions studied by OCT: in the peripheral regions of the lesion the corneal anatomy was conserved; it was possible to differentiate clearly the corneal structures from the epithelium to Descemet's membrane.
– Viral keratitis: homogeneous patterns of subepithelial and superficial stromal hyperreflectivity were identified in the area of the lesion, loss of differentiation of the epithelium generating shadowing. In the corneal structures adjacent to the lesion, the demarcation line between the healthy tissue and the affected area was well defined (Fig. 3).

Figure 3 Viral keratitis: homogeneous hyperreflective subepithelial lesion, loss of differentiation of the epithelium (asterisk) that generates shadowing. In the corneal structures adjacent to the lesion, the demarcation line (arrow) between the healthy tissue and the affected area is well defined.
– Fungal keratitis: highly heterogeneous hyperreflective areas involving the superficial and middle stroma, simulating a dentate pattern, with areas of greater reflectivity and a vertical posterior shadowing that extends throughout the corneal thickness, hyperreflective endothelial lesions, as well as loss of the normal architecture of the cornea, without delimitation of the healthy areas from the affected ones (Figs. 4 and 5).

Figure 4 Fungal keratitis: highly heterogeneous hyperreflective stromal lesion, with areas of greater reflectivity and full-thickness vertical posterior shadowing (arrow), as well as loss of architecture of the corneal anatomy, without delimitation of healthy from affected areas, as well as a retrocorneal plaque in the lesion (asterisk).
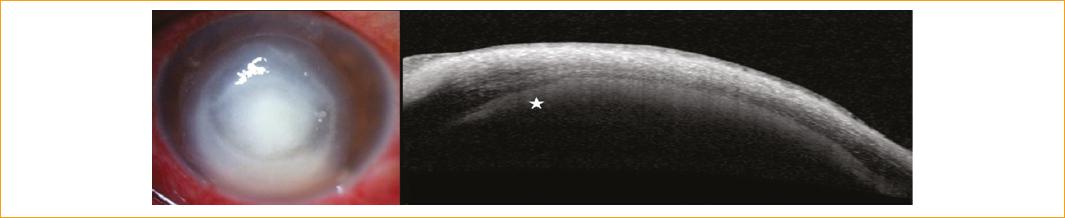
Figure 5 Fungal: Fungal keratitis: highly heterogeneous hyperreflective stromal lesion, with areas of greater reflectivity and full-thickness vertical posterior shadowing (arrow), as well as loss of architecture of the corneal anatomy, without delimitation of healthy from affected areas, as well as a retrocorneal plaque in the lesion (asterisk).
Discussion
Since our institution is a tertiary center, the evaluation of our patient population with keratitis can be very complex due to previous treatments and a long evolution; therefore, in this study we assessed ancillary methods for the differential diagnosis of infectious keratitis.
We identified morphological patterns that can be detected by spectral-domain OCT, which is useful to differentiate the causative agent (bacteria, virus and fungi) and to evaluate the degree of affectation and the inflammatory response.
Yokogawa, et al. reported irregular coin-shaped hyperreflective thickenings in the corneal endothelium in two patients diagnosed with cytomegalovirus endotheliitis, using spectral-domain OCT. In our study, viral keratitis was positive by PCR for herpes virus, and affected the epithelium and superficial stroma15.
Wael Soliman, et al. described 12 patterns in patients with infectious keratitis of bacterial and fungal etiology, of which 11 were present in both etiologies16. In the present study, a case of viral etiology was included, and hyperreflective and hyporeflective patterns were reported descriptively, looking for differences that would allow us to diagnose the type of keratitis, coinciding with that reported by Soliman regarding epithelial and stromal hyperreflectivity in the affected area. Regarding fungal etiology, a hyperreflective lesion attached to the corneal endothelium was observed in our study, but we did not observe the full thickness stromal cystic spaces, possibly due to the different time of evolution and the degree of corneal necrosis (Table 1).
Table 1 Comparison of corneal patterns detected by spectral OCT
| Soliman, et al. | Aguilar, et al. |
|---|---|
| Hyperreflective stromal lesion | Reported as stromal hyperreflectivity observed in the three etiologies |
| Epithelial defect | Described as loss of corneal epithelial demarcation in the three etiologies |
| Stromal edema | Not reported |
| Hyperreflective material underneath the epithelial defect or the hyperreflective stromal lesion | Specified as subepithelial homogeneous hyperreflectivity observed in the three etiologies |
| Hyperreflective lesion adhered to the corneal endothelium | A hyperreflective endothelial lesion was observed (fungal etiology) |
| Small stromal cystic spaces | Subepithelial hyporeflectivity in both bacterial and fungal etiology |
| Full thickness stromal cystic spaces | Not observed in our cases |
| Localized stromal thinning with epithelial defect | Observed in bacterial and viral etiologies |
| Loss of all corneal layers, except Descemet's membrane | Not observed in our cases |
| Hyperreflective stromal lesion with intact epithelium without stromal thinning | Observed in bacterial etiology with subepithelial and superficial stromal involvement |
| Hyperreflective stromal lesion with intact epithelium and localized stromal thinning | Observed in bacterial etiology with stromal involvement and in fungal etiology |
| Diffuse stromal thinning with epithelial defect | Observed in bacterial and viral etiology |
Abbouda, et al. used time-domain OCT for the follow-up of two patients with fungal keratitis treated by crosslinking and penetrating keratoplasty. As in our study, they described increased reflectivity in the anterior stroma in the area of the lesion, in addition to hyporeflective cysts due to tissue necrosis17.
Takezawa, et al. reported a retrocorneal plaque in patients with infectious keratitis of bacterial etiology, fungal and herpetic keratouveitis18. In four patients with fungal etiology in our study, we observed this type of retrocorneal findings like those reported by Takezawa (Fig. 5).
The patterns that may be useful to differentiate bacterial from fungal keratitis lie mainly in the preservation of the corneal anatomy of the unaffected areas and the ability to visualize deep structures underneath the lesion in bacterial ulcers. On the contrary, fungal ulcers show a greater involvement of the stromal anatomy, with more intense hyperreflective patterns that make difficult to differentiate deep and adjacent structures.
The loss of differentiation between affected and healthy tissue is more evident in fungal keratitis, making difficult to differentiate the corneal structures. This correlates with the destruction of both epithelial and stromal tissue caused by the necrosis and degree of inflammation generated by this type of infection.
Viral keratitis allowed to easily differentiate by OCT the affected tissue from the healthy one, possibly due to the delimitation of the virus and the localized inflammatory response of the cases studied.
Conclusions
We conclude the existence of corneal patterns that help us to differentiate the etiology in patients with infectious keratitis by spectral-domain OCT.
Its usefulness to determine the characteristics of the lesion and to evaluate the degree of involvement of the different corneal structures is emphasized, contributing to the decision-making in the medical and surgical treatment of the patients.

