











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Melanomas are malignant tumors arising from melanocytes. They can arise from both cutaneous and mucosal surfaces. Most melanomas are originated in the skin, while only 0.8- 3.7% are mucosal melanomas1. Primary mucosal melanomas (MM) can arise in any of the mucosal membranes lining the gastrointestinal and urogenital tracts2. Most mucosal melanomas occur in occult sites not accessible through a simple physical examination: the highest incidence is reported in the head and neck, vulvovaginal, anal, and rectal region3. Therefore, the disease commonly develops without any signs or symptoms for a long period of time before a definitive diagnosis is established - usually at a disseminated stage - with a more aggressive behavior and less favorable prognosis. Patients with advanced mucosal melanoma have a worse prognosis than those with advanced cutaneous melanoma (CM). In a retrospective observational study, the median overall survival of patients with advanced MM was 8.9 months and 14.5 months for CM4. With the introduction of immunotherapy in recent years, the management of patients with metastatic cutaneous melanoma has seen enormous progress and is comprehensively described in many published reviews. However, optimal management for mucosal melanoma is less clear because of the rarity of this disease. Options for systemic therapy are extrapolated from the approach used for metastatic cutaneous melanoma. Currently, the recommendation for patients with advanced mucosal melanoma is treatment with checkpoint inhibitor immunotherapy that incorporates a programmed cell death 1 (PD-1) inhibitor5. For patients with good performance status, combined therapy with nivolumab and ipilimumab is recommended, however, single-agent immunotherapy with nivolumab or pembrolizumab is a viable alternative: observational data in real-world patient populations with mucosal melanoma suggest that this approach has similar efficacy with less toxicity6. Despite a clear benefit in efficacy, both single-agent and combination immunotherapy are only accessible to a limited number of patients with advanced melanoma in low-and-middle-income countries due to their cost. Patients who can afford out-of-pocket costs are also at a high risk of financial toxicity. One of the proposed strategies to lower treatment costs and expand access to immunotherapy is the use of a lower dose than currently recommended in clinical practice guidelines.
Clinical case
A retired 77-year-old man with a past medical history of uncontrolled type 2 diabetes, hypertension, and pulmonary fibrosis, presented to our hospital with a recurrent left cervical mass. This mass had been treated 3 months prior to presentation with surgical resection and drainage due to a suspected cervical abscess with thick black drainage; no microorganisms were detected in pathology. The patient received multiple antibiotics, with recurrence of the cervical mass. On physical examination, a black/bluish lesion was observed on the right side of posterior third of the oral tongue, extending to the base of the tongue, as well as a 4 cm fixed left cervical mass. A CT scan of the neck showed a 22-mm solid lesion at the base of the tongue on the right side, with bilateral enlarged lymph nodes suggestive of metastatic disease.
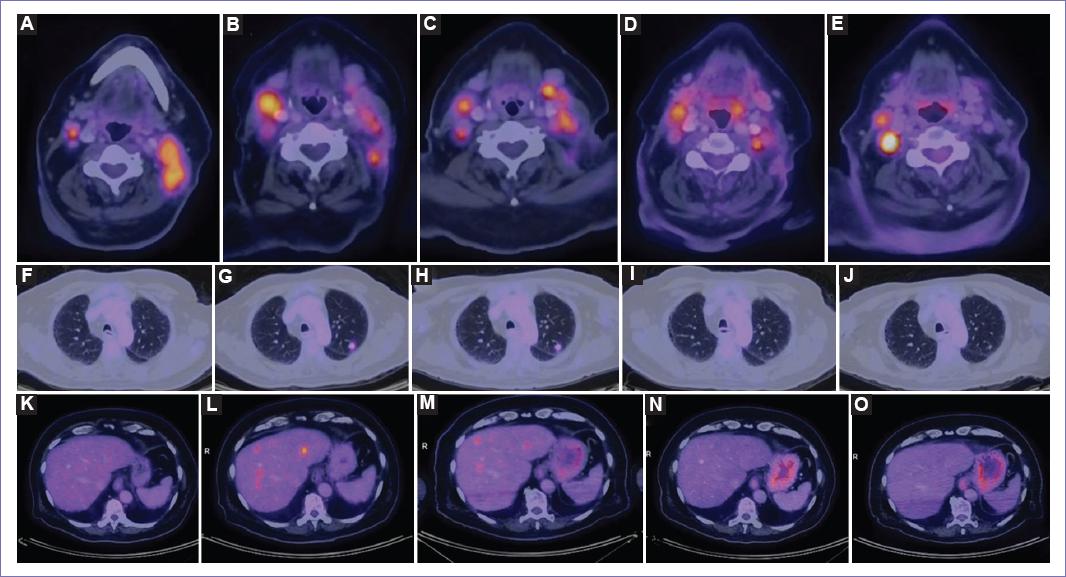
A percutaneous biopsy of the left cervical mass was performed, reporting metastatic melanoma. A 18F-fluorodeoxyglucose (FDG) PET/CT scan was performed, showing increased metabolism in the primary lesion at the base of the tongue with extension to the ipsilateral lingual tonsil, bilateral cervical lymph nodes and multiple pulmonary nodules, the largest of which measured 7 mm (Figs. 1A, 2A, 2F, and 2K). The patient received a geriatric assessment, in which multiple geriatric syndromes were detected, including visual impairment, disability for instrumental activities of daily living (IADL) (Lawton 4/8), mobility disability (he was able to walk 50 meters and climb a flight of stairs), falls, polypharmacy, and cognitive impairment. On multidisciplinary tumor board discussion, monotherapy with immune checkpoint inhibitors was recommended. However, due to financial constraints, the patient was not able to receive a full dose of either pembrolizumab or nivolumab. Therefore, nivolumab was started at a dose of 0.5 mg/kg, equaling a total dose of 40 mg every 2 weeks.
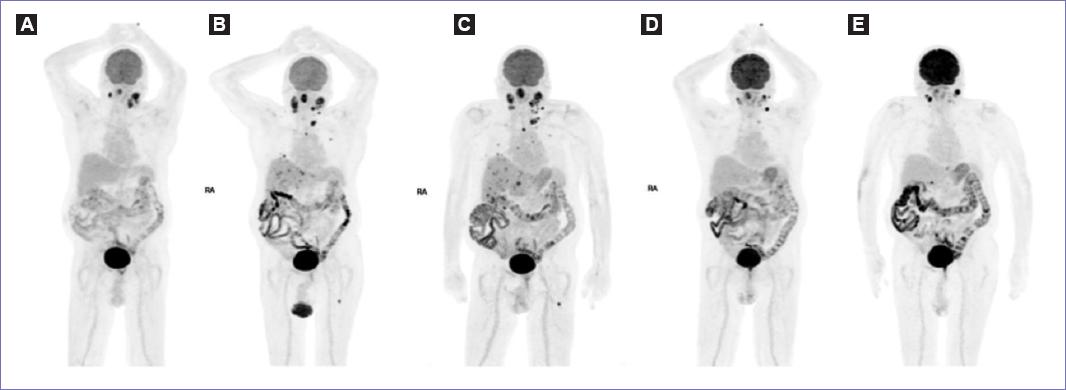
Figure 1 Whole-body 18F-FDG PET maximum-intensity. A: Baseline; B: After 6 cycles of nivolumab; C: After 11 cycles; D: After 17 cycles; E: After 26 cycles.
After 6 cycles, the patient was found without significant changes on symptoms, physical examination, or laboratory findings. A PET/CT scan showed an increase in size and metabolism of the primary lesion at the base of the tongue, an increase in number, size and FDG uptake of cervical lymph nodes and pulmonary nodules, as well as new liver and bone lesions (Figs. 1B, 2B, 2G, and 2L). Due to the patient remaining clinically stable, it was considered that criteria for unconfirmed progression (iUPD) by iRECIST were met and treatment was continued. After 8 cycles, a grade 2 eczematous dermatitis appeared on the superior extremities and trunk. The dermatitis improved with topical betamethasone and nivolumab was continued without interruption. A new PET/CT scan performed after 11 cycles did not show any significant changes, therefore response remained classified as iUPD (Figs. 1C, 2C, 2H, and 2M).
After 17 cycles, a decrease in size of the left cervical mass was detected. At this moment, a PET/CT scan showed a decrease in the number of the cervical lymph nodes, a decrease in size, number and FDG uptake of the pulmonary and liver lesions, and complete resolution of the bone lesions (Figs. 1D, 2D, 2I, and 2N). At this point, the patient remained functional for activities of daily living) (ADLs) with occasional episodes of urinary incontinence and his weight had increased by 2 kilograms, however IADL disability (Lawton 2/8), mobility disability (able to walk 10 meters and climb a flight of stairs) and cognitive impairment worsened. On his last PET/CT scan at 1 year since starting treatment, the primary tumor showed no significant changes in size or metabolism; some of the cervical lymph nodes showed a decrease in size, some increased in size and some remained stable; a new portocaval 11 mm lymphadenopathy with increased metabolism was observed; the pulmonary nodules decreased in size (the largest of 8 mm) without abnormal metabolism; and no liver or bone lesions were observed (Figs. 1E, 2E, 2J, and 2O). The patient has currently received 26 cycles of nivolumab and remains clinically stable. No new immune related adverse events have been noted.
Discussion
While most melanomas originate from the skin, a very small percentage arise from the mucosal surfaces1. Since mucosal melanomas are often diagnosed at a disseminated stage, they tend to exhibit a more aggressive biological behavior and carry a less favorable prognosis compared to cutaneous melanomas2,4.
In this case, the patient presented progressive disease in the PET/CT at the first evaluation of response, with partial response in subsequent imaging. Distinctive response patterns were identified in early melanoma trials of immune-based therapies in melanoma, including pseudoprogression7. Unconfirmed progression, or iUPD, is a category of pseudoprogression that occurs when a patient has an increase in tumor burden that is not confirmed by subsequent imaging studies, and the patient remains clinically stable or shows signs of improvement8. The decision to continue or discontinue immunotherapy in the setting of iUPD should be based on several factors: a patient’s overall clinical condition, extent of disease progression, and risk of immune-related adverse events. In this case, due to clinical stablility despite initial radiologic progression, treatment was continued after discussing with the patient.
Currently, treatment recommendations for patients with advanced mucosal melanoma include combined or single-agent immunotherapy. Real-world observations of patients with mucosal melanoma indicate that single-agent immunotherapy may present a similar efficacy at lower levels of toxicity6. However, immune checkpoint inhibitors are not available for many patients who could benefit from these treatments in low- and middle-income countries (LMIC), including Mexico, mainly due to their high cost. For example, in Mexico, the cost of a dose of 240 mg of nivolumab is 90,000-100,000 MXN (approximately 4,900-5,400 USD]), without including additional costs related to the administration of the drug. Given that the minimum wage per month in most of the country is 6,223 MXN (339 USD), and that the monthly household income in the fifth decile is 11,122 MXN (605 USD), this carries a high risk of financial toxicity when patients do not have access to treatment through some form of insurance.
It is well-known that cancer can lead to a significant financial burden for patients and their families. Financial toxicity describes the unintentional and unanticipated objective financial burden and subjective financial distress that patients experience due to their treatment9,10. Several studies have documented this phenomenon and its consequences. For instance, a study found a relationship between financial insolvency and mortality among patients with cancer using a large cancer registry dataset. Patients who were financially insolvent after cancer diagnosis were more likely to die within five years of cancer diagnosis than those who were not financially insolvent11. Financial toxicity has traditionally been one of the largest barriers to cancer care in low-income and middle-income nations. In a survey in 112 patients with newly diagnosed acute leukemia, in Nepal, who completed consolidation chemotherapy, all patients suffered financial toxicity, the most common financial hardship involved asking for donations, followed by borrowing loans from friends or relatives12. In another study that included patients 65 years or older with the 10 most common malignancies in Mexico and their family members, up to 90% of participants reported some form of financial toxicity13. The study also found that participants had limited knowledge about financial assistance programs, and that there is a need for more comprehensive financial counseling services to support patients and families in managing the financial impact of cancer.
Some of the proposed strategies to improve access to immunotherapy by decreasing costs are the use of weight-based dosing, vial sharing, or prescribing lower doses than currently approved. Growing data has shown that low dose nivolumab is effective in some cancer types such as NSCLC, renal cell carcinoma (RCC), and Hodgkin lymphoma14,15,16. The main justification is that neither nivolumab nor pembrolizumab have shown a clear dose-response relationship. For example, in a phase 1/2 trial of nivolumab in patients with advanced hepatocellular carcinoma the doses were prescribed from 0.1 to 10mg/kg every 2 weeks, resulted in substantial tumor reductions and objective response rates of 1520% irrespective of line of therapy17. Based on the comparability of pharmacokinetic exposure, safety, and efficacy, the FDA later approved nivolumab at a fixed dose of 240 mg Q2W for all approved indications regardless of body weight18.
The use of a low dose of nivolumab as an adjuvant therapy following the removal of melanoma metastases has been studied in a phase II trial. In one of the cohorts of this trial, patients received a fixed dose of 10 mg of nivolumab every two weeks for nine doses, followed by four additional doses every eight weeks. Using this treatment schedule, 12-month recurrence free survival was 85.7%, showing promising efficacy as an adjuvant therapy for melanoma19. A similar approach has shown to be effective in other tumors as well: in a retrospective series of 18 patients treated with 10 mg nivolumab IV every two weeks, two complete responses and two prolonged partial responses were observed20. Another retrospective study reported on the use of pembrolizumab at a lower dose in patients with non-small cell lung cancer: no difference in progression-free survival or overall survival was found between patients receiving pembrolizumab at a dose of 100 mg or 200 mg every three weeks. This study included a cost minimization analysis which estimated a cost saving per patient of around 29,500 USD21. Furthermore, in the first reported randomized phase III trial addressing the use of low-dose immunotherapy, 20 mg flat dose of nivolumab every three weeks was added to triple metronomic chemotherapy with oral methotrexate, celecoxib and erlotinib in patients with recurrent or newly diagnosed advanced head and neck cancer. This study was positive for its primary outcome, showing a marked improvement in 1-year overall survival (43.4% vs. 16.3%), using a regimen that decreases the cost of therapy to 5-9% of the cost of the current standard of care (KEYNOTE-048 regimen)22. Therefore, low-dose treatment schedules could pose an effective alternative to standard dosing, with a clear economic advantage.
Patient perspective and ethical considerations
The patient provided written informed consent for the creation and publication of this case report. The patient stated that he is "very satisfied with the treatment with nivolumab", and that without the dose modification, "it would be very difficult to afford this treatment due to its cost".
Conclusions
Mucosal melanoma is a rare and aggressive form of melanoma that has limited treatment options due to its rarity. Checkpoint inhibitor immunotherapy is the current standard of care for patients with advanced melanoma but is costly and only accessible to a limited number of patients. This report presents the case of a patient with metastatic mucosal melanoma who has been successfully treated with a low dose of nivolumab due to financial constraints. Further research is needed to evaluate the efficacy and safety of lower doses of immune checkpoint inhibitors, including its impact on long term outcomes. In the meantime, administering immune checkpoint inhibitors at low doses may serve as a strategy to improve access to an effective therapy in settings with limited resources.

