











 nueva página del texto (beta)
nueva página del texto (beta) Inglés (pdf)
Inglés (pdf)
 Artículo en XML
Artículo en XML Referencias del artículo
Referencias del artículo
 Enviar artículo por email
Enviar artículo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkIntroduction
Ureteral injury can be divided into traumatic and iatrogenic. Iatrogenic ureteral injury represents around 75% of all ureteral injuries1. The main causes of iatrogenic injury are obstetric and gynecological surgery, representing 64%-82%. Traumatic ureteral injury is associated with car accidents or firearm injuries. Treatment of ureteral injury depends on several factors, such as the time of diagnosis, the location, and the extent of the injury. Treatment methods range from endoscopic therapy to reconstruction of the ureter with intestinal segments2. There are bibliographic precedents such as the case report in Mexico with ureter replacement with cecal appendage in patients with ureteral stenosis3. In the same way, there are other cases of ureteral replacement with cecal appendage for post-surgical management in the case of lesions due to retroperitoneal tumors and post radiation therapy, also in cases of external trauma and its main use today in pediatric patients4-6. However, there are no reports prior to the case of presenting a 20-year-old male patient with a single right kidney secondary to left nephrectomy with iatrogenic lesion of the right ureter with total absence of it. Here, the replacement by cecal appendix is shown, the imaging studies and the multidisciplinary management by the radio intervention service are presented, as well as the clinical evolution until the removal of the nephrostomy and urination uresis are achieved.
Surgical repair of ureteral injury
The principle of treatment for ureteral injury is to reconstruct the ureter, restore the continuity and integrity of the urinary tract, reduce the occurrence of complications, and protect renal function. The main treatment for long-segment ureteral injury is surgical repair and reconstruction. During the operation, the anastomotic stoma should be free of tension and water leakage, and attention should be paid to protecting the blood supply of the ureter and its substitute tissue7.
End-to-end ureteral anastomosis
The end-to-end ureteral anastomosis is the simplest operation to repair ureteral injuries and is suitable for crush or ligation injuries within 3 cm of the upper or middle ureter. Prior to end-to-end anastomosis, the two ureteral stumps are cut longitudinally and spatulated, which may reduce the occurrence of complications8.
Ureteral reimplantation technique used (Lich-Gregoir).
The extra bladder procedure is known as Lich-Gregoir, in which a longitudinal incision is made outside the bladder wall down to the muscle layer, the incision is about 3-4 cm long and then the ureter is removed, the opening is anastomized with the bladder mucosa and, finally, the end of the ureter is sutured in the incised seromuscular layer to achieve the purpose of antireflux in the submucosal tunnel9.
Ureteral replacement
At present, when the ureteral lesion is too long or cannot be repaired with the urinary tissue itself for other reasons, the first treatment option for long-segment ureteral injury is the repair and reconstruction of the urinary tissue itself. Autologous replacement of ureteral organ tissue is an effective treatment. Currently, the most common ureteral autologous replacement tissue is the ileum, with others including the appendix, colon, oral mucosa, fallopian tubes, and veins.
Replacement of ureter by ileum
The ileum is the most commonly used autologous tissue in mid, lower, or total ureter replacement. The ileum is similar to the ureter in terms of tubularity and peristalsis, which can restore urinary tract continuity and protect renal function10. Although ureter-ileal segment substitution has been widely promoted, it also has drawbacks; the ileal mucosa secretes intestinal mucus, and excessive secretion of intestinal mucus blocks the lumen in the long term. Electrolyte disturbances and acid-base balance disorders; it can also favor urinary tract infections secondary to urinary stasis, urinary reflux is common; another long-term complication is strictures of the anastomoses. The optimal length of the ileum to replace the ureter is between 15 and 25 cm, and should not exceed 40 cm. An ileum that exceeds 40 cm considerably increases the risk of postoperative electrolyte imbalance11.
Suspicious ureter replacement
The replacement of the ureter by the cecal appendix was described for the first time by Melnikoff et al in 1912 (Fig. 1)12. In Mexico, a ureter replacement technique with cecal appendage was described by Dr. Delfino Gallo Aranda in 1956; its main indication is uretero-vesical fistulas13. This introduced the ureter replacement surgery. Appendiceal replacement is suitable for long ureteral defects and is generally used on the right side. The necessary characteristics are sufficient length of the appendage, diameter proportional to the defect of the ureter, adequate mobility of the meseapex. The advantages of using appendicular replacement are: technically simpler, diameter similar to the ureter, proper irrigation, intrinsic motility, feasible in pediatric use. Other additional advantages are that it does not have an absorption function, decreasing hydroelectrolytic alterations like other intestinal segments. The main disadvantages are the production of mucus that causes infections and stone formation, as well as the impossibility of determining if there are favorable anatomical conditions when using the cecal appendix before surgery, so the decision is trans-surgical14. The most frequent complications described are stenosis of the anastomosis of the appendicular segment and leakage of the anastomosis.

Case Report
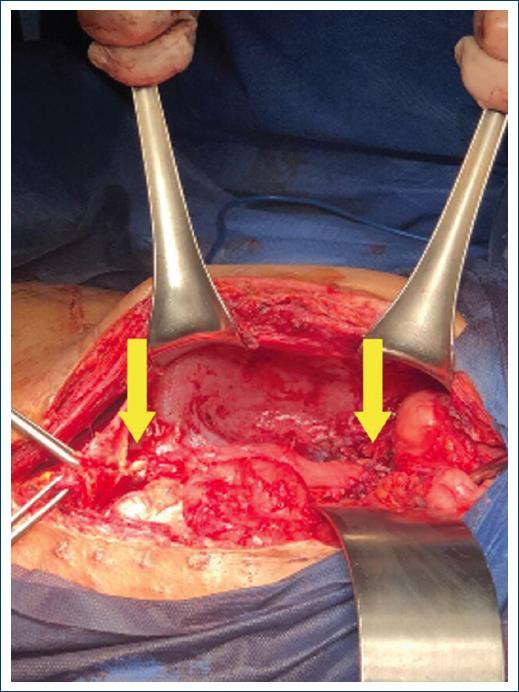
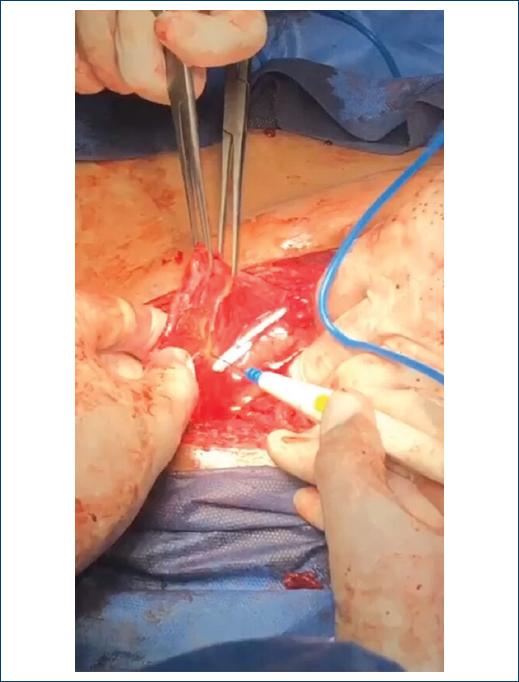
A 20-year-old male patient attends a rural hospital in Chiapas for acute abdominal data. Left nephrectomy was performed presenting incidental injury to the contralateral ureter. A right ureterostomy is performed with a 12 Fr Nélaton catheter to temporarily divert the urinary tract (Fig. 2). Proband was referred to the Urology service of the General Hospital of Mexico for management of the ureteral lesion and preservation of right kidney. Lab studies were creatinine 2.5 mg/dL, urea 48 mg/dL, complete blood count: leukocytes 10,000 x mm3, neutrophils 67%, hemoglobin 13.4 g/dL, hematocrit 38.6%, platelets 195,000 per mm3, urine with cloudy yellow color, 500 leukocytes per field, positive nitrites, countless bacteria and erythrocytes, positive urine culture for Escherichia coli 100,000 CFU/ml sensitive to carbapenems. A protocol was established for exploratory laparotomy and it was decided to perform complete right ureteral replacement with cecal appendage quietly. The intestinal segment is prepared (Fig. 3) and the mesoappendix is maintained to preserve irrigation. A proximal (renal pelvis- appendix) end-terminal anastomosis and a distal (appendix-bladder) anastomosis are performed using the Lich-Gregoir technique (Fig. 4). A double J catheter is placed in the neoureter (Fig. 5), a right penrose is placed, and it is maintained with a transurethral catheter. A post-surgical control plate was made (Fig. 6).



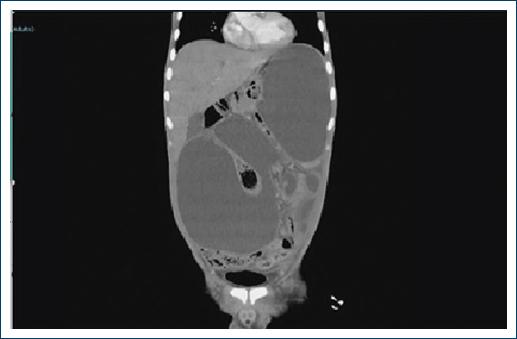
During the postoperative period, the patient presented a decrease in urinary output and an increase by the Penrose test, for which a control tomography was performed and an intra-abdominal collection compatible with urinoma was observed (Fig. 7). A right percutaneous catheter is placed and 3500 mL of urine is drained. Therefore, radiological control is performed where contrast medium leakage is observed in the proximal anastomosis, right nephrostomy is placed to divert the urinary tract. The radiointervention service removed the double J stent previously placed in surgery and a long percutaneous catheter was successfully placed anterogradely through the previously placed right nephrostomy to maintain splinted neoureter, preventing leakage from the proximal anastomosis (Fig. 8). During follow-up in the outpatient clinic, the patient presented urination uresis and was kept under surveillance.

The long catheter is removed at 3 months and the following 3 months the right nephrostomy catheter is left, alternating its closure with uresis through urination of the patient. Finally, at 6 months the nephrostomy catheter is removed. Currently the patient presents urination uresis and follow-up by Nephrology and Urology (Fig. 9).

Discussion
In this clinical case, renal function could be preserved with the help of ureter replacement with transposition of the cecal appendix, an unusual maneuver.
Ureteral cecal appendage substitutions are a treatment option for extensive ureteral lesions. It is an unusual technique today. However, with multiple advantages, but certain necessary features are required.
This surgical technique was described by Melnikoff in 1912. The many advantages offered by this technique are: a simpler technique, a diameter similar to that of the ureter, its own irrigation, peristalsis, and its disadvantages: obstruction due to the production of intestinal mucus, length of appendage, stenosis of anastomosis, risk of stone formation used in cases of ureteral stricture in pediatric patients also in some cases of iatrogenic ureteral injury, since there was no segment of the ureter and there was previous loss of the left renal unit, an end-to-side ureteral anastomosis could not be offered, and in the case of ileal ureteroplasty with multiple adhesions it was risky and with little chance of success14.
The perfect substitute for ureter defects, nowadays it is an unreality despite technological advances; the other options are segments of ileum, uterine tubes. The cecal appendix offers advantages: diameter similar to the ureter, own irrigation, peristalsis; the disadvantages are mucus production, appendectomized patients, high risk of complications such as strictures, fistulas, and anastomosis dehiscence15. The use of the cecal appendix in cases of ureteral stenosis has been used in pediatric patients; the main limitation in this technique is the small size in length and diameter of the appendix. In a series of cases, the main long-term complication is stenosis of the anastomoses; however, management can be endoscopic16.
As an early complication, urinary leakage occurred in the postoperative period, due to a dehiscence of the anastomosis at the upper end. The radiointervention service drained the urinoma with a transabdominal percutaneous catheter guided by ultrasound; u urinary tract derivation was performed with the placement of a nephrostomy catheter and the defect of the dehiscence of the upper anastomosis was splinted with a long catheter. This was placed anterogradely through the nephrostomy, since previously placed the catheter runs from the upper end of the renal pelvis passing through the cecal appendage neoureter to the bladder.
Conclusion
In the case of ureteral lesions, there are multiple techniques with replacement of intestine segments, a therapeutic option is replacement of the ureter with cecal appendage, in addition to having the advantages of having motility, own irrigation; however, and a diameter similar to that of the ureter, as limitations due to intrinsic anatomy, production of mucoid secretion, therefore obliteration of the lumen, risk of infection. Within the late complications, there are the stenosis of the anastomoses and the formation of lithiasis in the neoureter. Complications that can be managed endoscopically, so patient follow-up is necessary for timely and adequate management.

